

Abstract
Background:
Diabetes imposes a large economic burden on the individual, national healthcare systems, and countries.
Objective:
To determine the economic impact of diabetes mellitus on Saudi healthcare system, both now and in the future.
Materials and Methods:
This research study uses a prevalence-based approach that combines the demographics of the population (classified by nationality, sex and age group) with and without diagnosed diabetes in 1992 and 2010. The economic impact of diabetes is estimated in this study, using secondary sources of information provided by Ministry of Health, Ministry of Finance and Central Department of Statistics and Information databases.
Results:
People diagnosed with diabetes, on average, have medical healthcare expenditures that are ten times higher ($3,686 vs. $380) than what expenditures would be in the absence of diabetes. Over 96% of all medical healthcare expenditures attributed to diabetes are incurred by persons of Saudi nationality, with the remaining 4% incurred by persons of non-Saudi nationality. The population age 45-60 incurs 45% of diabetes-attributed costs, with the remaining population under age 15 incurs 3.8%, age 15-44 incurs 27.5%, and age 60 and above incurs 23.8%.
Conclusion:
The actual national healthcare burden because of diabetes is likely to exceed the $0.87 billion estimated in this study, because it omits the indirect costs associated with diabetes, such as absenteeism, lost productivity from disease-related absenteeism, unemployment from disease-related disability, lost productivity due to early mortality by disease. The social cost of intangibles such as pain and suffering and care provided by non-paid caregivers as well as healthcare system administrative costs, cost of medications, clinician training programs, and research and infrastructure development is also omitted from this research study. Further studies are needed to confirm the present findings and to improve our understanding of economic costs of diabetes and its related complications.
Keywords: Diabetes mellitus, economic costs, healthcare system, Saudi Arabia
INTRODUCTION
Diabetes imposes a large economic burden on the individual, national healthcare systems, and countries.[1–5] Healthcare expenditures due to diabetes account for 11% of the total healthcare expenditures in the world in 2011.[6] Estimated global healthcare expenditures to treat diabetes and prevent complications totaled $465 billion in 2011. By 2030, this number is projected to exceed some $595 billion. On average, the estimated healthcare spending due to diabetes was $5,063 per person with diabetes in high-income countries compared with $271 in low- and middle-income countries. Worldwide, the estimated number of adults living with diabetes has soared to 366 million, representing 8.3% of the global adult population. This number is projected to increase to 552 million people by 2030, or 9.9% of adults, which equates to approximately three more people with diabetes every 10 or almost 10 million per year.[7–8] The Kingdom of Saudi Arabia is not exception of this global pandemic.
Over the past four decades major socio-economic changes have occurred in Saudi Arabia. The ageing of populations, together with rapid socio-economic development (progressive urbanization, decreasing infant mortality and increasing life expectancy) and tremendous changes in lifestyle towards the westernized pattern reflected by changes in nutrition, less physical activity, tendency to increased obesity and more smoking, has resulted in the dramatic increase in the diabetes prevalence.[9–16] Worldwide, the desire of many healthcare players (governments, diabetes associations, health professionals, health economists, and people with diabetes themselves) to reduce the economic burden of diabetes and its related complications costs makes the question of economic impact of diabetes an important component in:[17,18]
Determining the present economic burden of diabetes and its related complications on government healthcare system
Predicting the likely future economic burden of diabetes and its related complications, and
Developing effective policies and strategies about treatment of diabetes and its related complications and the future public health spending related diabetes healthcare costs.
The purpose of this research study, therefore, is to determine the economic impact of diabetes mellitus (DM) on Saudi Arabia's healthcare system, both now and in the future. This research study, however, focuses on the prevalence of diabetes and aims at estimating and predicting the total and per capita healthcare expenditure for people diagnosed with diabetes.
MATERIALS AND METHODS
To examine and predict the economic impact of diabetes costs on Saudi Arabia's healthcare system, this study relied on data provided by Ministry of Health (MOH) and Ministry of Finance (MOF) for the years 1992 and 2010 databases.[19–21] The 1992 and 2010 time period is used as the study time frame. Population figures from the 1992 and 2010 MOH databases for patients who reported that they had diabetes were selected for this study. Data on government budget, total healthcare budget, and per capita health expenditure were obtained directly from the MOH and MOF databases. Data on population (by nationality, sex and age groups) with undiagnosed diabetes obtained directly from Central Department of Statistics and Information databases.[22,23] It should be noted that this study is based on single-source of diabetic data (MOH database) only; therefore, it does not account for the considerable number of people diagnosed with diabetes in other healthcare providers such as private and semi-private healthcare services (Military, Universities, Arabian American Oil Company (ARAMCO) healthcare services, etc.). Consequently, diabetes prevalence is probably much higher than figures presented in this study because a significant number of people diagnosed with diabetes are not included in the analysis. It should also be noted that the perspective adopted in this study is that of the MOH. If other perspective were used such as payer, society or health care provider, the results would be different. In addition, data on diabetes was obtained from MOH database is based on diabetic clinics visits in both MOH hospitals and healthcare centers, and it combined in- and out-diabetic-patients which is categorized by nationality (Saudi/non-Saudi); sex (male/female); and age groups (<1; 1-4; 5-14; 15-44; 45-60; and 60+). It should be noted that, it is not clear whether data provided by the MOH database is based on first visits related to diabetes. Therefore, it is not certain whether diabetic data is protected from double counting or not.
This research study used prevalence-based approach that combines the demographics of the population with and without diagnosed diabetes in 1992 and 2010. The general principle for estimating the healthcare costs of diabetes is straightforward.[24–27]
Healthcare use attributable to diabetes is determined by a comparison of the healthcare use patterns of individuals with and without diabetes. Dividing healthcare expenditures by the size of the population with and without diabetes provides an estimate of per capita healthcare expenditures.
By multiplying diabetes population figures by the per capita healthcare expenditures, the total healthcare budget for people diagnosed with diabetes is derived.
Assuming diabetes prevalence rates remained constant over time, the exponential projection method (i.e., annualized change) is used to reflect the growing prevalence of diabetes in the Saudi Arabia and the increasing costs of healthcare expenditures over the next 10 years (i.e., 2020).
It should be mentioned that, the modern approach to conducting cost-of-illness studies is based on system of health account (SHA) approach.[28] SHA is used to describe the health care system from an expenditure perspective. However, as there is no SHA in Saudi Arabia, other approaches had to be used. Knowledge of the costs of diabetes improves understanding of the importance of addressing healthcare and prevention issues associated with diabetes and help to inform and motivate decisions that can reduce the national burden of this disease.
RESULTS
Population size with diabetes
Based on the MOH database approximately 0.9 million people in 1992 and 2.5 million people in 2010 have been diagnosed with diabetes. Analysis of the 1992-2010 MOH database suggests that the number of people diagnosed with diabetes increased by 1.6 million (or 183%) during the last 18 years. This increases the proportion of the total population with diabetes from 5.3% in 1992 to 9.3% in 2010. Comparison of the 2010 diabetes figure to the 1992 figure suggests that the net number of people diagnosed with diabetes is growing by about 0.1 million per year. This increased prevalence of diabetes over the period of study is not only attributable to changing pattern of Saudi lifestyle due to rapid socio-economic development (together with increased obesity, smoking and less physical activities) but may also be attributed to increased awareness programs related to diabetes and its health complications, community screening campaigns for diabetes, better diagnostic facilities specially in health centers and healthcare units, and better diabetes management systems and protocols. In fact, several community-based screening campaigns studies for DM and hypertension were conducted in different parts of Saudi Arabia revealed that quite a large percentage of these participants (diabetic patients) were not detected and remain for a long time without significant symptoms. These studies concluded that community-based screening campaigns are extremely efficient in identifying undiagnosed diabetic and hypertensive individuals in the society.[29–33]
Table 1 summarizes the demographic component of population diagnosed with diabetes. The MOH database for population diagnosed with diabetes by nationality, sex, and age-group, suggests that Saudi citizens comprised 84% and 96% of total population diagnosed with diabetes in 1992 and 2010, respectively, while, non-Saudi population diagnosed with diabetes comprised 16% in 1992 and about 4% in 2010. The demographic analysis also revealed that over half of total population diagnosed with diabetes, in 1992 and 2010, are males while females represented about 47% and 48% of total population diagnosed with diabetes in 1992 and 2010, respectively. The analysis revealed that about 1 in 11 males being diabetic in 2010 as compared with 1 in 19 males in 1992. For females, about 1 in 9 were diabetic in 2010 compared with 1 in 17 in 1992.
Table 1.
Population (in millions) and percent of population with and without diabetes, 1992 and 2010
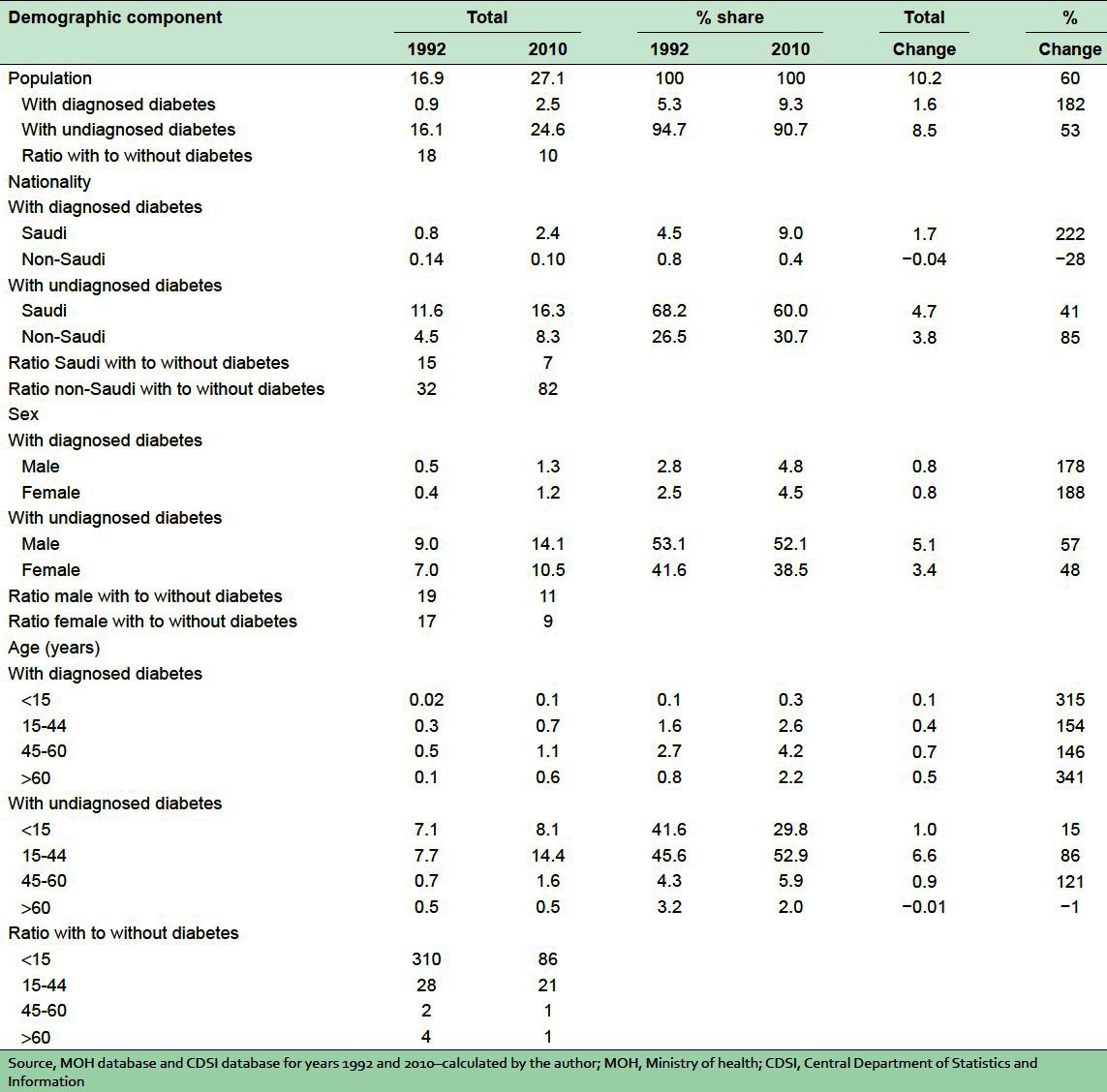
The population between 45 and 60 years represented the highest among population diagnosed with diabetes during the period of analysis. This age group comprised about 52% and 45% of total population diagnosed with diabetes in 1992 and 2010, respectively, with remaining population under age 15, age 15-44, and 60 years and above comprised about 3%, 21%, 15% in 1992 and about 4%, 27%, 24% in 2010, respectively. It is important to mention that the population age 60 years and above represents the highest percentage increase among population diagnosed with diabetes during the last 18 years of analysis. This age group increased by more than 340%. The population of age 60 years and above diagnosed with diabetes is growing by more than 33.6 thousand people per year. The analysis revealed that the ratio of population of age 60 years and above diagnosed with diabetes to with undiagnosed diabetes rose from (1:4) in 1992 to almost (1:1) in 2010. It is well documented that the population with the highest use of healthcare resources attributed to diabetes is the population aged 60 years and above.[34–38]
Healthcare expenditures attributed to diabetes
Healthcare expenditure attributed to diabetes reflects the additional expenditures the nation incurs because of diabetes. This equals to the total healthcare expenditures for people with diabetes minus the projected level of expenditures that would have been incurred in the absence of diabetes. In effect, this is estimates the excess healthcare use that is theoretically due to (or caused by) diabetes and its related complications. The term “attributed” also means the difference in healthcare use for people with diabetes compared with what their healthcare use would be in the absence of diabetes.[39]
Table 2 summarized national healthcare expenditures for MOH healthcare system. The MOH healthcare expenditures accounted for over $9.4 billion dollars in 2010. Approximately $0.9 billion in healthcare expenditures is incurred by people with diabetes, reflecting $1 of every $11 MOH healthcare dollars. Healthcare expenditures incurred by people with diabetes increased by more than 500% during the last 18 years. In 2010 on average, people diagnosed with diabetes have medical healthcare expenditures that are ten times higher ($3,686 vs. $380) than what expenditures would be in the absence of diabetes ($1 US dollar = 3.75 Saudi riyal).
Table 2.
Healthcare expenditures by diabetes status, nationality, sex, and age groups, 1992 and 2010 – (in USA dollars)
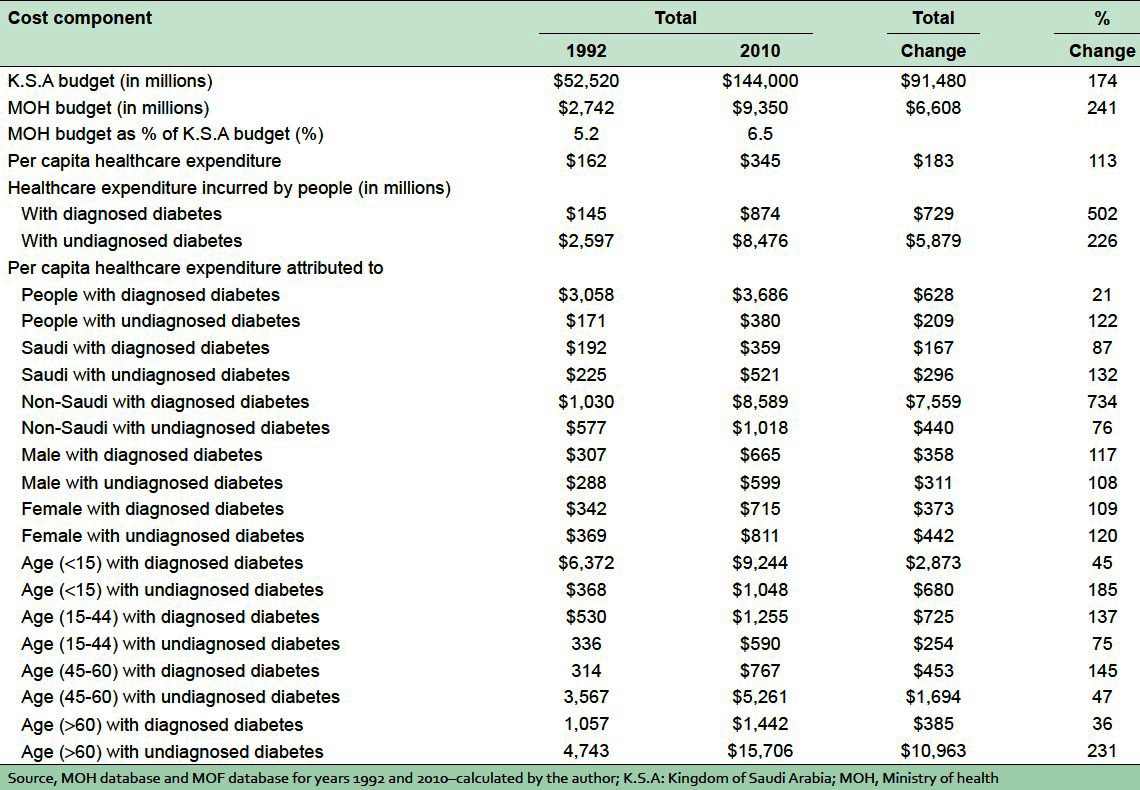
Dividing total attributed healthcare expenditures by the number of people diagnosed with diabetes, gives an estimate of the average annual excess expenditures for the population under age 15, age 15-44, age 45-60, and age 60 and above at $9,244, $1,255, $767, and $1,442, respectively. The population between age 45and 60 has the highest per capita healthcare expenditure during the last 18 years. Per capita expenditure for population between age 45 and 60 increased by more than 145% between 1992 and 2010, followed by age 15-44 (137%), under age 15 (45%), and age 60 years and above (36%). The analysis revealed that the per capita healthcare expenditure for the population under age 15 is almost nine times higher ($9,244 vs. $1,048) than healthcare expenditures of otherwise similar age group without diabetes. The analysis also revealed that the per capita healthcare expenditure for the population between age 15 and 44 is two times higher ($1,255 vs. $590) than healthcare expenditures of the otherwise similar age group without diabetes. Per capita healthcare expenditure for male/female population diagnosed with diabetes is equal (to some extent) to the per capita healthcare expenditure of male/female population without diabetes. Similarly, per capita for Saudi citizens diagnosed with diabetes is to some extent equal to per capita for Saudi citizens with undiagnosed diabetes. While, per capita healthcare expenditure for non-Saudi population is eight times higher ($8,589 vs. $1,018) than healthcare expenditures of non-Saudi nationality without diabetes.
Future economic burden of diabetes
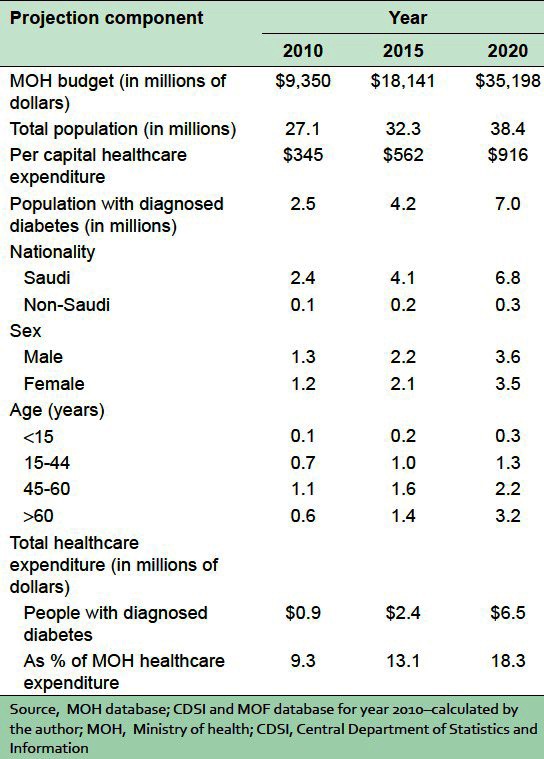
As mentioned earlier, the rapid increase of socio-economic development in Saudi Arabia coupled with improved living standards and technological advancements during the last four decades has resulted in dramatic change of Saudi lifestyle. Over-nutrition, increasing obesity and smoking rate, and less physical activity and many other factors reflecting the substantial increase in the size of Saudi population diagnosed with diabetes.[40–45] These factors are likely to remain, and if diabetes prevalence rates remained constant over time, then the number of people diagnosed with diabetes is expected to rise by 4.2 million in 2015 and by another seven million by 2020.
The economic burden of diabetes on Saudi Arabia is expected to be approximately $2.4 billion in 2015 [Table 3]. This is an increase of $1.5 billion, or nearly three times the level in 2010, this cost is also expected to rise by another $6.5 billion in 2020. Given the expected increase in the number of people diagnosed with diabetes in Saudi Arabia, the proportion of public healthcare spending is expected to escalate from 9.3% in 2010 to 13.1% in 2015 and to 18.3% by 2020.
Table 3.
Projection of population with diagnosed diabetes and their healthcare expenditure – (in USA dollars)
The actual economic burden of diabetes in future years is expected to be higher if the cost of health care outpaces the overall cost of living, or if the growing problem of obesity increases the prevalence rate diabetes. The cost estimate of diabetes documents the extraordinary national economic burden of diabetes. Even so, such estimates do not account for the lost productivity and losses attributable to pain and suffering incurred by people diagnosed with diabetes, as well as to families and friends of those with diabetes.
CONCLUSIONS
Diabetes is a personal crisis for people living with the disease, and for their families. Diabetes is also causing a financial crisis for Saudi healthcare system. Treatment of the disease and its related complications are consuming an ever-larger share of healthcare budgets, and will soon force a tremendous increase in those budgets. Although the population diagnosed with diabetes comprises more than 9% of the Saudi population in 2010, almost 1 in 11 people in Saudi Arabia having diabetes, and if the present prevalence rate remains unchanged over time, the ratio of people with to without diabetes will increase by almost 1 in 5 people having the disease in 2020.
Diabetes cost the nation an estimated $0.9 billion in 2010. People diagnosed with diabetes have medical healthcare expenditures that are ten times higher than what expenditures would be in the absence of diabetes. This cost is estimated to be $6.5 billion by 2020 reflecting an increase of $5.6 billion (or 7 times higher than the cost in 2010) within the next 10 years or so. These figures represent a substantial economic burden to the future system of Saudi healthcares. Although, the diabetes cost estimates presented in this research study might be conservative for several reasons:
Omitted from this analysis due to data limitations is the number of people who reported that they had diabetes in both private and other governmental (e.g. universities hospitals, Armed Forces Medical Services, Security Forces Hospital, National Guard Medical Services, Royal Commission Hospitals, Youth Welfare Hospital, now Saudi ARAMCO) healthcare service providers. At the time of writing in 2012, there are 148 hospitals and about 2,360 health clinics not related to MOH healthcare system. This research study relied only on data obtained directly from the MOH healthcare database on people diagnosed with diabetes and ignored other sources of data due to difficulty in obtaining them. Consequently, diabetes prevalence is probably much higher than figures presented in this study because a significant number of cases are not included in the analysis.
Omitted from the cost estimates is the indirect cost associated with diabetes such as lost productivity due to disease-related absenteeism, unemployment due to disease-related disability, lost productivity due to early mortality by disease as well as the social cost of intangibles such as pain and suffering and care provided by non-paid caregivers. The prevention programs targeted to people with diabetes, research activities, and administration costs associated with diabetes are also omitted for the diabetes cost estimates in this study. If a portion of these costs were attributed to diabetes, the national healthcare cost of diabetes would be billions of dollars higher than what the estimate suggest in this study.
Sensitivity analysis related diabetic mellitus and its related complications were not carried out in this study.
Worldwide, resources allocated to diabetes prevention and treatment, are growing, but prevalence is also growing steadily. Several international reports on preventing DM indicated that people with diabetes are at greater risk of neurological disease, peripheral vascular disease, cardiovascular disease, renal disease, endocrine/metabolic complications, ophthalmic disease, and other chronic complications compared with individuals without diabetes.[1–8] Chronic complications are the main cause of death among diabetic patients and account for the higher costs in hospitalization and drugs, and the costs of drugs for these complications are 2.5 times higher than those for the general population. These international reports suggested that better access to preventive healthcare system, more widespread diagnosis, more intensive disease management, and the advent of new medical technologies could significantly eliminate or reduce the health problems caused by diabetes. These factors could also improve the quality of life for people with diabetes and their families, while at the same time potentially reduce national expenditures for healthcare services and increasing productivity in the national economy.
To sum up, further research studies are needed to improve our understanding of economic costs of diabetes and its substantial burden to Saudi healthcare system. Special attention should also be given to the role of diabetic awareness programs, community-based screening campaigns and different health educational programs in reducing health problems caused by diabetes, which in the long run, helps to reduce the national burden of this disease. SHA should also be adopted by Saudi health providers to deal with these developments of financial health flows related to the consumptions of healthcare goods and services.
ACKNOWLEDGMENT
I would like to extend my sincere gratitude to Dr. Fahd Al-Muhanna for his valuable contribution in revising the manuscript and for his suggestions and comments in preparing this research study.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Hogan P, Dall T, Nikolov P. American Diabetes Association. Economic costs of diabetes in the US in 2002. Diabetes Care. 2003;26:917–32. doi: 10.2337/diacare.26.3.917. [DOI] [PubMed] [Google Scholar]
- 2.American Diabetes Association. Economic costs of Diabetes in the US in 2007. Diabetes Care. 2008;31:1–20. doi: 10.2337/dc08-9017. [DOI] [PubMed] [Google Scholar]
- 3.Canadian diabetes Association. An economic tsunami: the cost of diabetes in Canada. 2009. [Last accessed on 2012 Feb 22]. Available from: http://www.diabetes.ca/documents/get-involved/FINAL_Economic_Report.pdf .
- 4.Ray N, Thamer M, Chan J. American Diabetes Association. Economic consequences of diabetes mellitus in the U.S. in 1997. Diabetes Care. 1998;21:296–309. doi: 10.2337/diacare.21.2.296. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Fact sheet: Diabetes. 2010. [Last accessed on 2012 Jan 12]. Available from: http://www.who.int/mediacentre/factsheets/fs312/en/index.html .
- 6.International Diabetes Federation. Diabetes Atlas. 5th ed. Brussels, Belgium: IDF Publications; 2011. [Last accessed on 2012 Feb 03]. The Global Burden of Diabetes; pp. 7–13. Available from: http://www.idf.org/diabetesatlas/news/fifth-edition-release . [Google Scholar]
- 7.World Health Organization. Global Burden of Disease (GBD) estimates Death and DALY estimates for 2002 by cause for WHO Member States. 2004. [Last accessed on 2012 Jan 12]. Available from: http://www.who.int/healthinfo/global_burden_disease/en/index.html .
- 8.World Health Organization. Preventing Chronic Diseases: A Vital Investment. Geneva: World Health Organization; 2005. Chapter 1- Chronic diseases: causes and health impacts; pp. 34–58. [Google Scholar]
- 9.El-Hazmi M, Warsy A, Al-Swailem A.R, Al-Swailem A.M, Sulaimani R. Diabetes mellitus as a health problem in Saudi Arabia. East Mediterr Health J. 1998;4:58–67. [Google Scholar]
- 10.El-Hazmi M, Warsy A. Prevalence of Obesity in the Saudi Population. Ann Saudi Med. 1997;17:302–6. doi: 10.5144/0256-4947.1997.302. [DOI] [PubMed] [Google Scholar]
- 11.Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS, Arafah MR, Khalil MZ, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25:1603–10. [PubMed] [Google Scholar]
- 12.Famuyiwa OO, Sulimani RA, Laajam MA, Al-Jasser SJ, Mekki MO. Diabetes mellitus in Saudi Arabia: The clinical pattern and complications in 1,000 patients. Ann Saudi Med. 1992;12:140–51. doi: 10.5144/0256-4947.1992.140. [DOI] [PubMed] [Google Scholar]
- 13.Al-Shehri ST. Al-Khobar: King Faisal University; 1995. Direct costs of diabetes mellitus: Estimation of direct cost of health services offered to adult diabetic patients in Ministry of Health Centers in Al-Khobar Area [dissertation] [Google Scholar]
- 14.Al-Hamdan NA, Al-Zalabani AH, Saeed AA. Comparative study of physical activity of hypertensives and normotensives: A cross-sectional study of adults in Saudi Arabia. J Family Community Med. 2012;19:162–6. doi: 10.4103/2230-8229.102315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fatani HH, Mira SA, el-Zubier AG. Prevalence of diabetes mellitus in rural Saudi Arabia. Diabetes Care. 1987;10:180–3. doi: 10.2337/diacare.10.2.180. [DOI] [PubMed] [Google Scholar]
- 16.Fatani HH, Mira SA, El-Zubier AG. The prevalence of diabetes mellitus in Urban Saudi Arabia. In: Niliyanant W, Vichyanarat A, Vannasseng S, editors. Diabetes Mellitus. Bangkok: Crystal House; 1985. pp. 8–16. [Google Scholar]
- 17.Martin AB, Whittle LS, Levit KR. Trends in state health care expenditures and funding: 1980-1998. Health Care Financ Rev. 2001;22:111–40. [PMC free article] [PubMed] [Google Scholar]
- 18.Cost-effective approaches to diabetes care and prevention. Brussels, Belgium: IDF Task Force on Diabetes Health Economics, IDF Publication; 2003. [Last accessed on 2012 Feb 22]. International Diabetes Federation. Available from: http://da3.diabetesatlas.org/indexc1f0.html . [Google Scholar]
- 19.Chapter I: Review of Health Situation. Annual Health Report, 1992. Saudi Arabia, Riyadh: Department of Statistics; 1992. Ministry of Health; pp. 27–80. [Google Scholar]
- 20.Chapter II: Health Indicators: Health Statistical Year Book, 2006. Saudi Arabia, Riyadh: Department of Statistics; 2006. [Last accessed on 2012 Jan 22]. Ministry of Health; p. 27. Available from: http://www.moh.gov.sa/statistics . [Google Scholar]
- 21.1992 and 2010 Statistical Year Book. Saudi Arabia, Riyadh: Ministry of Finance; 1992. Ministry of Finance. Chapter 11: Health Budget; pp. 106–133. [Google Scholar]
- 22.Statistical Yearbook. Riyadh, Saudi Arabia: Ministry of Planning; 1992. Central Department of Statistics and Information. Chapter 3: Population Indicators; pp. 27–35. [Google Scholar]
- 23.Statistical Yearbook. Riyadh, Saudi Arabia: Ministry of Planning; 2010. [Last accessed on 2011 Dec 21]. Central Department of Statistics and Information. Chapter 3: Population and Housing Indicators; pp. 33–63. Available from: http://www.cdsi.gov.sa . [Google Scholar]
- 24.Bagust A, Hopkinson PK, Maier W, Currie CJ. An economic model of the long-term health care burden of Type II diabetes. Diabetologia. 2001;44:2140–55. doi: 10.1007/s001250100023. [DOI] [PubMed] [Google Scholar]
- 25.King H, Aubert RE, Herman WH. Global burden of diabetes, 1995-2025: Prevalence, numerical estimates, and projections. Diabetes Care. 1998;21:1414–31. doi: 10.2337/diacare.21.9.1414. [DOI] [PubMed] [Google Scholar]
- 26.Brandle M, Zhou H, Smith BR, Marriott D, Burke R, Tabaei BP, et al. The direct medical cost of type 2 diabetes. Diabetes Care. 2003;26:2300–4. doi: 10.2337/diacare.26.8.2300. [DOI] [PubMed] [Google Scholar]
- 27.Oliva J, Lobo F, Molina B, Monereo S. Direct health care costs of diabetic patients in Spain. Diabetes Care. 2004;27:2616–21. doi: 10.2337/diacare.27.11.2616. [DOI] [PubMed] [Google Scholar]
- 28.OECD, Eurostat, WHO. A System of Health Accounts. Paris, France: OECD Publishing; 2011. Part I: Concepts and Methods for health Account; pp. 23–107. [Google Scholar]
- 29.Al-Ghamdi AJ, Al-Turki KA, Al-Baghli NA, El-Zubaier AG. A community-based screening campaign for the detection of diabetes mellitus and hypertension in the Eastern province, Saudi Arabia: Methods and participation rates. J Family Community Med. 2007;14:91–7. [PMC free article] [PubMed] [Google Scholar]
- 30.Al-Baghli NA, Al-Turki KA, Al-Ghamdi AJ, El-Zubaier AG, Al-Baghli FA, Bohlaiqa NH. Control of hypertension in Eastern Saudi Arabia: Results of screening campaign. J Family Community Med. 2009;16:19–25. [PMC free article] [PubMed] [Google Scholar]
- 31.Karim A, Ogbeide DO, Siddiqui S, Al-Khalifa IM. Prevalence of diabetes mellitus in a Saudi community. Saudi Med J. 2000;21:438–42. [PubMed] [Google Scholar]
- 32.Kalantan KA, Mohamed AG, Al-Taweel AA, Abdul Ghani HM. Hypertension among attendants of primary health care centers in Al-Qassim region, Saudi Arabia. Saudi Med J. 2001;22:960–3. [PubMed] [Google Scholar]
- 33.Abahussain NA, El-Zubier AG. Diabetes knowledge among self reported diabetic female teachers: Al-khobar, Saudi arabia. J Family Community Med. 2005;12:43–8. [PMC free article] [PubMed] [Google Scholar]
- 34.Shorr RI, Franse LV, Resnick HE, Di Bari M, Johnson KC, Pahor M. Glycemic control of older adults with type 2 diabetes: Findings from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Geriatr Soc. 2000;48:264–7. doi: 10.1111/j.1532-5415.2000.tb02644.x. [DOI] [PubMed] [Google Scholar]
- 35.World Health Organization. Geneva: World Health Organization; 1997. Chapter 3: Charting the Future, The World Health Report 1997 Conquering Suffering, Enriching Humanity; pp. 121–136. [PubMed] [Google Scholar]
- 36.Al-Mahroos F. Diabetes mellitus in the Arabian Peninsula. Ann Saudi Med. 2000;20:111–2. doi: 10.5144/0256-4947.2000.111. [DOI] [PubMed] [Google Scholar]
- 37.Kamel NM, Badawy YA, el-Zeiny NA, Merdan IA. Sociodemographic determinants of management behaviour of diabetic patients. Part II. Diabetics’ knowledge of the disease and their management behaviour. East Mediterr Health J. 1999;5:974–83. [PubMed] [Google Scholar]
- 38.Chin MH, Zhang JX, Merrell K. Diabetes in the African-American Medicare population. Morbidity, quality of care, and resource utilization. Diabetes Care. 1998;21:1090–5. doi: 10.2337/diacare.21.7.1090. [DOI] [PubMed] [Google Scholar]
- 39.Gilmer TP, O’Connor PJ, Rush WA, Crain AL, Whitebird RR, Hanson AM, et al. Predictors of health care costs in adults with diabetes. Diabetes Care. 2005;28:59–64. doi: 10.2337/diacare.28.1.59. [DOI] [PubMed] [Google Scholar]
- 40.Al-Nuaim AR, Al-Rubeaan K, Al-Mazrou Y, Al-Attas O, Al-Daghari N, Khoja T. High prevalence of overweight and obesity in Saudi Arabia. Int J Obes Relat Metab Disord. 1996;20:547–52. [PubMed] [Google Scholar]
- 41.Warsy AS, el-Hazmi MA. Diabetes mellitus, hypertension and obesity – Common multifactorial disorders in Saudis. East Mediterr Health J. 1999;5:1236–42. [PubMed] [Google Scholar]
- 42.Abalkhail B. Overweight and obesity among Saudi Arabian children and adolescents between 1994 and 2000. East Mediterr Health J. 2002;8:470–9. [PubMed] [Google Scholar]
- 43.Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: A brief review. East Mediterr Health J. 2004;10:663–70. [PubMed] [Google Scholar]
- 44.Al-Hazzaa HM. Obesity and physical inactivity among Saudi children and youth: Challenges to future public health. J Family Community Med. 2006;13:53–4. [PMC free article] [PubMed] [Google Scholar]
- 45.Al-Baghli NA, Al-Ghamdi AJ, Al-Turki KA, El-Zubaier AG, Al-Ameer MM, Al-Baghli FA. Overweight and obesity in the Eastern Province of Saudi Arabia. Saudi Med J. 2008;29:1319–25. [PubMed] [Google Scholar]