

Abstract
Background:
Effective reduction of malaria morbidity and mortality in Nigerian children under the age of five depends to a large extent on family biosocial factors. Although, the awareness of insecticide treated bed nets (ITNs) is reportedly high and increasing in Nigeria there remain large gaps between awareness, possession and use by families with children under the age of five in Nigeria.
Aim:
To determine the family biosocial variables that influence the use of insecticide treated nets for children in Eastern Nigeria.
Materials and Methods:
A descriptive hospital-based study was carried out from June 2008-June 2011 on a cross-section of 415 mothers with children under the age of five, who were treated for confirmed malaria, and met the selection criteria were interviewed using a pretested, structured researcher-administered questionnaire. The questionnaire tool elicited information on family socio-demographic variables, inter-spousal discussion, communication, concurrence and participation in the use of insecticide treated bed nets; and reasons for non-utilization. The period of usage in the previous 6 months was assessed and graded using a scoring system of 0-4. Scores of 1-4 indicated usage while score of 0 meant non use.
Results:
The rate of ITNs use was 53.0%. The family variables that significantly influenced utilization were secondary education and above of parents (mother: P = 0.009; father: P = 0.001), monogamy (P value = 0.024), family size of 1-4 (P value = 0.016) and parents living together (P = 0.001); others included parents’ occupation (mother: P = 0.003; father: P = 0.04) and inter-spousal discussion (P value = 0.001), communication (P value = 0.001), concurrence (P = 0.000) and participation (P = 0.000). The commonest reason for non- use was inconvenience during sleep (P = 0.04).
Conclusion:
This study shows that the rate of ITN use was marginally good. Specifically, this rate was significantly influenced by some family variables. The families of children under the age of five should, therefore, be the focus of intensive health promotion campaign to influence the use of ITNs to produce ITN family friendly communities.
Keywords: Children, family biosocial variables, hospital, ITNs-use, malaria, Nigeria
INTRODUCTION
The socio-economic and medical burden Malaria imposes on families includes the disruption of family dynamics leading to family dysfunction and staggering economic costs.[1,2] Malaria infection accounts for 7 out of ten outpatient visits in Nigerian hospitals and is responsible for 25% infant mortality and 30% under-five mortality.[3]
The Roll Back Malaria Initiative (RBMI) has identified the use of insecticide treated bed nets (ITNs) as a key strategy for malaria prevention especially for under-five children in sub-Saharan Africa.[4] The benefits of ITNs have been documented particularly with regard to childhood morbidity and mortality and the World Health Organization (WHO) has called for its increased use.[5–8] The effectiveness of ITNs has been demonstrated in the reduction of the number of febrile episodes in children,[5] decreased level of malaria parasitaemia and mosquito density,[5,6] as well as childhood mortality ranging from 14-72% in some African trials.[9] The global prioritization of malaria control in Africa motivated the Federal Government of Nigeria after the Abuja malaria summit in 2000 to commit to the global effort to reduce the burden of malaria by 50% by the end of the year 2010 setting a mid-term target to have 60% of the population at risk such as under-five children in endemic communities use ITNs by the year 2005.[10,11] These global efforts are essential for the achievement of the Millennium Development Goals (MDGs) with regard to malaria disease and child health.
There is overwhelming evidence in the tropics that the use of ITNs for under-five is most advantageous while non use is associated with increased morbidity and mortality from malaria.[5,6] Of great concern, therefore, is that despite the relatively high awareness of ITNs and rates of use reported in Gambia,[12] and Guatemala,[13] the rates of ITNs possession and use reported in Nigeria have been unimpressive.[14–16]
More importantly, malaria control intervention such as possession and utilization of ITNs are aimed at building human and institutional resources to fight the malaria scourge. The families of the under-five children constitute important human and social institutional resources for which the utilization of ITNs should play a significant role in promoting health. The family is the most basic social unit which directs the health status and the socio-medical needs of its members.[17] Furthermore, families are important recipients of health information (message) who motivate the community on practices that promote health such as the use of ITNs. Reliable and comparable analysis of family socio-demographic factors that influence the utilization of ITNs is the cornerstone for effective free distribution and social marketing of ITNs An understanding of these factors is valuable for acquiring ITNs and using them effectively especially for children under the age of five in malaria endemic communities. In addition, utilization of ITNs is integral to key family practices with implications for family health particularly child health.
There has been a marked increase in the social marketing and the current free distribution of ITNs in recent times. As the awareness and possession of ITNs increase in families with under-five children, it is expected that there would be a corresponding increase in their utilization for the group most at risk of malaria morbidity and mortality. The effects of family variables on malaria disease and illness in under-five children as regards the use of ITNs in malaria prevention in Nigeria needs to be explored. However, family variables that influence the use of ITNs for the under-fives are yet to be studied in the region, particularly at secondary healthcare level in a rural area of Imo State, Nigeria. Moreover, the target years 2005 and 2010 of RBMI have passed and 2015, the target year of Millennium Development Goals (MDGs) is fast approaching. It is therefore, necessary to assess the use of ITNs in families with children under the age of five now. It is against this background that the researchers set out to ascertain family socio-demographic and inter-spousal variables that influence the utilization of ITNs for under-five in rural Nigeria. This study was aimed at determining the family biosocial variables influencing the use of insecticide treated nets for children in Eastern Nigeria in order to make a preliminary assessment of the need for family-friendly interventional programmes to establish and promote a culture of ITNs use for malaria control.
MATERIALS AND METHODS
This was a hospital-based descriptive study carried out from June 2008-June 2011, on a cross-section of 415 mothers of under-five children treated for confirmed malaria at St. Vincent De Paul Hospital, Amurie-Omanze, a rural Mission General Hospital in Isu Local Government Area of Imo State, South-Eastern Nigeria. The hospital gives 24 hours of service daily, including public holidays, to the community and its environs.
A minimum sample size of 250 was calculated using the formula,[18] for estimating minimum sample size for descriptive studies when studying proportions with an entire population size <10,000 using an estimated population size of 500 under-five patients based on the previous annual hospital attendance of under-five patients. We assumed that 50% of the respondents would use ITNs for the under-five patients, at 95% confidence level and a 5% margin of error. A total of 415 respondents were used based on the time frame for the study.
After clinical evaluation of the under-five patients, those who had presumptive diagnosis of malaria had the diagnosis confirmed by thick blood film microscopy using standard Giemsa staining technique. The study population were recruited from among mothers whose under-five children were treated for confirmed malaria at the study centre during the study period. Only married women who possessed ITNs and whose husbands were alive and were in communication with them were interviewed in order to evaluate inter-spousal factors. The under-five who were brought to the hospital by care givers other than their mothers, those used to pre-test the questionnaire in the study centre, and those who used untreated nets were excluded from the study. Moreover, under-five who needed specialized diagnostic investigations and care were referred out and excluded from the study. The mothers were interviewed using researcher administered pretested structured questionnaire after obtaining a verbal informed consent on a one to one basis, and assured of confidentiality. In order to ensure that no mother was interviewed more than once, those interviewed were properly documented at the time of the interview and the records were subsequently cross-checked prior to every interview session. Detailed enquiries were made about:
Family socio-demographic variables such as parental age, occupation and educational status. Social classification of the parents was based on a five-point occupational classification described in a previous study.[19] However, this was reclassified into a lower class (social classes V and IV), middle class (social class III) and upper class (social class I and II) to suit the Nigerian environment.
Family structure and dynamics such as type of marital union, family size, inter-spousal discussion, communication, concurrence and participation in the use of ITNs for children under the age of five.
The use of ITNs was assessed in the previous 6 months before presentation to the hospital and graded using ITNs utilization scoring system of 0-4 developed by the authors from the review of literature,[12–15,20] as follows: Always = 4 points, most times = 3 points, occasionally = 2 points, rarely = 1point and never = 0 point. Those who scored 1 and above were graded as users while 0 score was graded as a non-user. The reasons for non-utilization were also elicited from those who were scored 0.
Clinical symptoms and presenting complaints of the patients were also recorded. A child was defined as having malaria if the mother made a complaint of fever, vomiting and other symptoms suggestive of malaria, had a body temperature exceeding 37.5°C with the asexual forms of Plasmodium falciparum detected on the peripheral blood film.
The questionnaire was pre-tested internally using ten mothers of under-five in the study centre who met the selection criteria and ten other mothers at St. Damian hospital Okporo, a similar Mission General Hospital in Orlu, Imo State. The respondents for the pre-testing were randomly selected and those from the study centre were excluded from the main study. The pretesting was done to find out how the respondents would react to the questionnaire to eliminate any ambiguities. However, no change was necessary after the pre-test as the questions were clearly understood as intended.
The authors operationally defined the family as a couple and their children. Inter-spousal discussion referred to the husband and wife who had a discussion about ITNs in order to decide whether or not to use it for a child under the age of five; inter-spousal communication referred to the exchange of information between husband and wife on the use of ITN for the under-five child either face to face, by telephone, letter or internet; inter-spousal concurrence referred to an agreement between the husband and wife on the use of ITNs for the under-five child, while inter-spousal participation referred to the involvement of the husband and/or wife in putting up the ITN for the under-five child.
Statistics
The results generated were analysed using software Statistical Package for Social Sciences (SPSS) version 13.0, Inc. Chicago, IL, USA for the calculation of frequencies and percentages for categorical variables. Bivariate analysis involved the use of Chi-Square for testing the significance of associations between categorical variables. In circumstances where small expected frequencies were encountered, Chi-Square with appropriate Yates continuity correction was employed. Fisher's exact test was used where appropriate. Furthermore, univariate logistic regression analysis was performed at 95% confidence limit. The level of significance was set at P < 0.05.
RESULTS
Of the 415 respondents who met the selection criteria, 220 respondents said they had used the ITNs for their under-five year children in the previous 6 months before presenting to the study centre, while 195 had not used any, giving ITNs use rate of 53.0%.
Table 1 shows the use of ITNs and associated family variables of the respondents. At bivariate analysis, there were statistically significant associations between the use of ITNs for the under-five and some family variables: Parents who had secondary education and above used ITNs more than those who had primary education and below (mother: 57.3% vs 42.7%, P value = 0.009; father: 65.0% vs 35.0%, P value = 0.001), parents from monogamous families used ITNs more than those from polygamous families (96.8% vs 3.2%, P value = 0.001); parents with a family size of less than four used ITNs more than those who had larger families (68.6% vs 31.4%, P value = 0.001); parents who lived together used ITNs more than parents who lived apart (66.8% vs 33.2%, P value = 0.001); parents who had inter-spousal discussion used ITNs more than those who didn’t (81.8% vs 18.2%, P value = 0.001); parents who had inter-spousal communication used ITNs more than those who didn’t (82.7% vs 17.3%, P value = 0.001); parents between whom there was inter-spousal concurrence used ITNs more than those who had none (86.4% vs 13.6%, P value = 0.000); parents between whom there was inter-spousal participation used ITNs more than those who had none (89.1% vs 10.9%, P value = 0.000). Another statistically significant family variable was parental occupation (mother: P value = 0.003; father: P value = 0.04). The parental age and social classification seemed to influence the use of ITNs, but the association was not found statistically significant.
Table 1.
Family variables as related to ITN utilization among the respondents
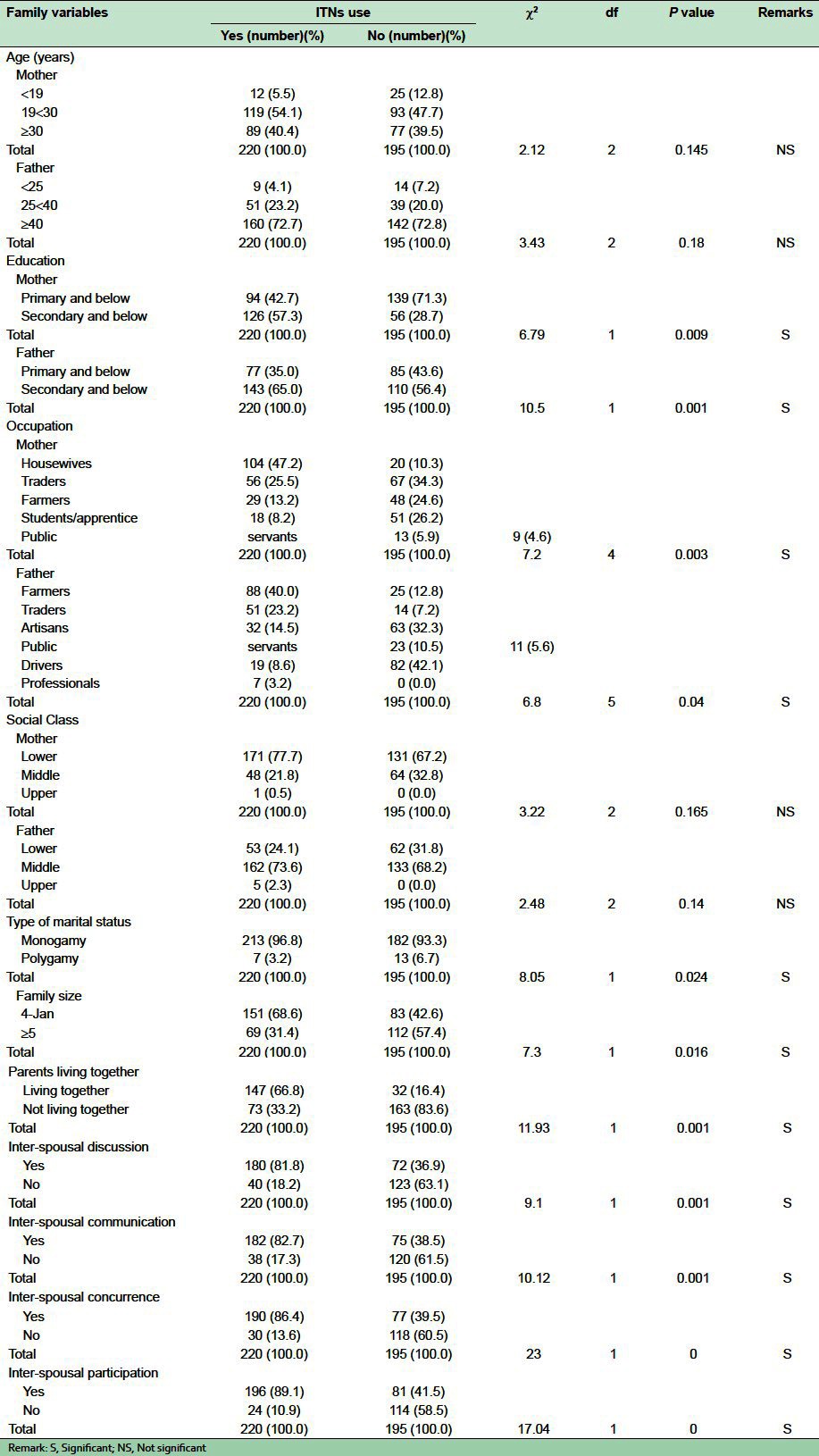
Table 2 shows logistic regression analysis of the family variables. On univariate logistic regression analysis of the family variables in relation to the use of ITNs, family type, size, parents living together, inter-spousal discussion, communication, concurrence and participation were significantly associated while parental education and occupation had no significant influence on the use of ITNs.
Table 2.
Logistic regression coefficient of family variables
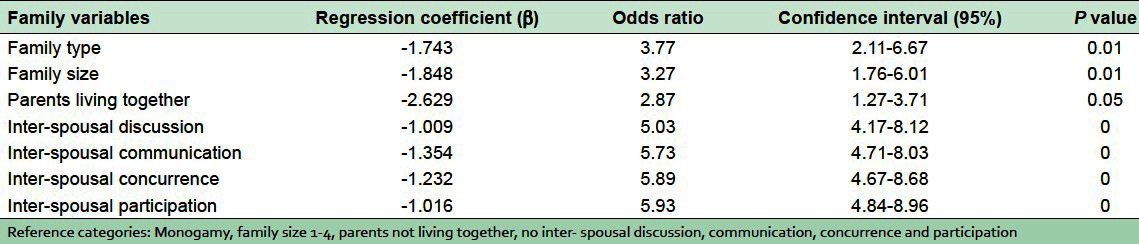
Table 3 shows the reasons for non use of ITNs. The most common reason proffered for non-use was inconvenience during sleep (36.6%). Other reasons included the chore of having to mount and dismantle the net every day, hot night temperatures (heat) and the absence of mosquitoes. The difference was statistically significant (χ2 = 5.04; df = 3; P value = 0.04) [Table 3].
Table 3.
Reasons for non-use of ITNs

DISCUSSION
The 53.0% rate of the use of ITNs in this study is higher than 7% reported in a survey in South-Eastern Nigeria,[20] 2.1% in Ile-Ife,[14] 22.8% in Sagamu,[15] and 20.5% in Malawi.[21] However, higher rates were reported in Gambia (86.0%),[12] and Guatemela (75%),[13] The comparatively average user rate in this study could be attributed to the activities of RBMI in the state which discouraged the sales of ITNs in the health facilities, with the free distribution and the intensification of health talks on its benefits and effectiveness. This is also expected as a consequence of health education on ITNs which the mothers received at the antenatal and infant welfare clinics of health facilities in the study area. Moreover, the distribution of free ITNs to pregnant women who attend antenatal clinics and mothers of under-five who had completed their routine immunization were contributory factors. However, this marginal rate of use in this study has a far reaching implication on the use of ITNs. The focus of health promotion activities on ITNs should be to translate awareness into practice. Although, the rate of use in this study is average, it is still a far cry from the MDGs policy target of 100% by the year 2015. The present rate of use can be improved by focusing family health education on ITNs use. The education of primary care givers in the families particularly mothers, for whom the priority should be the supply of proper adequate information to counter the commonly held erroneous beliefs and misconceptions on ITNs.
This study has shown that parental educational status significantly influenced the use of ITNs for children under the age of five. An majority of the parents had secondary school education and above. This may be attributed to the Federal Government of Nigeria policy on Universal Basic Education and adult literacy classes. Moreover, reports have shown that spousal education generally improves the family health practices and is associated with greater commitment to the care of the child. This includes the awareness, knowledge and use of health promotion materials such as ITNs.[22,23] The reason may be that education tends to influence the acceptance of health-related messages and affords a wider scope for interaction and information exchange on ITNs use, its benefits and effectiveness.
This study also observed that parental occupation significantly influenced ITNs use. This is in keeping with the general belief that occupation plays a major role in shaping family health. Accordingly, occupation increases family access to health resources and strengthens their family health practices such as the use of ITNs and promotes socialization which encourages the exchange of information on health.
Almost all respondents who used ITNs for under-five children in this study were from monogamous family structure. This is probably a function of family communication on ITNs. In addition, monogamous marriages are generally seen as a proximal indicator of family unity and harmony in which the health needs of children under the age of five are guaranteed. Functional family communication especially that between mother and father in a monogamous marriage is viewed as a critical tool in the utilization of such family health promotion materials as ITNs.
This study observed the influence of family size on the use of ITNs for the under-five. The smaller the family size the higher the use of ITNs. This finding is in consonance with the observation that a large family size is more likely to be characterized by a high rate of stress and distress as well as poor family support for the use of ITNs.[24,25] In addition, a large family size usually provides an unhealthy environment for family health promotion practices.
Parents who lived together significantly influenced the use of ITNs for their children under the age of five. Living together had a great impact on the success or failure of medical intervention including the utilization of ITNs.[25] It does appear that couples who lived together were able to influence each other in the use of ITNs to promote the health of an under-five child. In such families, the father maintains the traditional role as the primary bread winner and the mother as the primary home maker.
Although ITNs are distributed free in health facilities, its use is influenced by the decision making process in the family.[25] This study revealed that inter-spousal discussion, communication, concurrence and participation significantly influenced their use for under-five. The decision-making process and actions of the husband and the wife are related to their socio-demographic and family characteristics. Couples communicate verbally and non-verbally with each other, interpret each other's behaviour, and make inferences on the partner's desires and intentions that may result in concurrence and participation in the use of ITNs. This can foster better understanding leading to a decision in favour of the health practice of using ITNs for the under-five. This could be attributed to the family dynamics. This finding is therefore, a clarion call for the review of the current strategies for the free distribution of ITNs to target families in most need as well as those families most likely to fail to use ITNs for children under five, who are at risk.
This study has revealed that the most common reason proffered by respondents for not using ITNs for their children was inconvenience during sleep. This reason is at variance with the most common reason for non-use of ITNs reported in Ile-Ife (non-availability of ITNs),[14] Sagamu (lack of knowledge of ITNs),[15] and Egbema, Rivers state (hot night time temperature).[26] Non-availability of ITNs was not recorded as a reason for non-utilization since they were distributed free of charge by the Federal Government of Nigeria and other international and local non-governmental organizations such as USAID, UNICEF, NETMARK and community- based organizations under the RBMI programme of the World Health Organization.
Study implications
This study has implications for primary care practices and health promotion strategies as regards malaria prevention in children under the age of five by using ITNs. Moreover, it has relevance for key family health promotion practices such as the use of ITNs aimed at reducing morbidity from malaria infection. For poor nations such as Nigeria, the utilization of health care resources for families is mainly driven by the need for curative rather than preventive services. This is probably due to socio-demographic and family variables that adversely affect family health. It is by taking cognizance of these family variables that influence utilization of ITNs that effective interventional planning can be done aimed at increasing ITNs use for this special group of children. It is therefore, envisaged that this study would provide baseline information on the influence of family variables on ITNs utilization by families with children under the age of five in the study area for comparative and promotional purposes.
Study limitations
The limitations of this study are recognized by the researchers. First, since the sample for the study was drawn from hospital attendees in the community, the findings may not be generalized for the influence of family variables on the use of ITNs for the under-five children with malaria disease in the study area. Any generalization of the results of this study to cover the entire community and its environs should be done with caution. Secondly, the study was based on interviews and may thus be prone to information bias on ITNs use by the respondents. Some respondents couldn’t clinically and socially give acceptable and true responses to questions related to health practices. However, their effect was minimized by the structure of the questions as well as an assurance of confidentiality given to the respondents prior to the conduct of the interview. Thirdly, the questionnaire was pre-tested internally in the study centre and externally in a similar rural mission general hospital in another local government area, in Imo state for clarity and acceptability. Furthermore, the scoring system in the report of this study did not adhere to ITN usage because of the biological relevance of occasional or rare use of ITNs, which thus fails to prevent mosquito attack and thereby reduce the incidence of malaria.
CONCLUSION
This study shows that the rate of ITNs was marginally adequate. Specifically, ITN user rate in this study was significantly influenced by some family variables. It is only by inquiring, examining and addressing these family variables that the target 100% ITN utilization by 2015 as recommended by Millennium Development Goals can be achieved. It is recommended that the families of children under the age of five should be the focus of intensive health education and promotion campaign on the use of ITNs. Effective pragmatic intervention strategies to enhance these factors will impact positively on the rate of ITN use leading to ITN family friendly communities.
ACKNOWLEDGMENT
The authors are grateful to Rev. Sister Francisca Eya of St. Vincent de Paul hospital, Amurie-Omanze for permission for the study.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Breman JG, Alilio MS, Mills A. Conquering the intolerable burden of malaria: What's new, what's needed: a summary. Am J Trop Med Hyg. 2004;71:1–15. [PubMed] [Google Scholar]
- 2.Gallop JL, Sachs JD. The economic burden of malaria. Am J Trop Med Hyg. 2001;64:85–96. doi: 10.4269/ajtmh.2001.64.85. [DOI] [PubMed] [Google Scholar]
- 3.FMOH. Abuja, Nigeria: National Malaria and Vector Control Division, FMOH; 2005. National Antimalaria Treatment Policy; pp. 1–66. [Google Scholar]
- 4.Jones C. Overcoming barriers to the use of insecticide treated nets. Afr Health. 2000;22:18–20. [Google Scholar]
- 5.Nwankwo BO, Okafor JO. Effectiveness of insecticide-treated bed nets (ITNs) in malaria prevention among children aged 6 months to 5 years in a rural community in Imo state, Nigeria. Int J Trop Med. 2009;4:41–9. [Google Scholar]
- 6.Gimnig JE, Vulule JM, Lo TQ, Kamau L, Kolczak MS, Phillips-Howard PA, et al. Impact of permethrin-treated bed nets on entomologic indices in an area of intense year round malaria transmission. Am J Trop Med Hyg. 2003;68:16–22. [PubMed] [Google Scholar]
- 7.Lengeler C. Insecticide treated nets for malaria control: real gains. Bull World Health Organ. 2004;82:84. [PMC free article] [PubMed] [Google Scholar]
- 8.Hawley WA, ter kuile FO, Steketee RS, Nahlen BL, Terlouw DJ, Gimnig JE, et al. Implications of the Western Kenya permethrin-treated bed net study for policy, program implementation and future research. Am J Trop Med Hyg. 2003;68:168–73. [PubMed] [Google Scholar]
- 9.Kolaczinski J, Webster J. Malaria control in complex emergencies: The example of East Timor. Trop Med Int Health. 2003;8:48–55. doi: 10.1046/j.1365-3156.2003.00969.x. [DOI] [PubMed] [Google Scholar]
- 10.Yameh G. African Heads of states promise action against malaria. BMJ. 2000;320:1228. [PMC free article] [PubMed] [Google Scholar]
- 11.WHO. Roll Back Malaria-Africa Summit, Abuja, Nigeria. WHO News Letter. 2000;15:1–22. [Google Scholar]
- 12.Aikins MK, Pikering H, Alonso PL, D’Alessandro U, Lindsay SW, Todd J, et al. A malaria control trial using insecticide-treated bed nets and targeted chemoprphylaxis in a rural area of The Gambia, West Africa.4. Perceptions of the causes of malaria and of its treatment and prevention in the study area. Trans R Trop Med Hyg. 1993;87:25–30. doi: 10.1016/0035-9203(93)90172-m. [DOI] [PubMed] [Google Scholar]
- 13.Klein RE, Weller SC, Zeissig R, Richards FO, Ruebush TK., 2nd Knowledge, beliefs and practices in relation to malaria transmission and vector control in Guatemela. Am J Trop Med Hyg. 1995;52:383–8. doi: 10.4269/ajtmh.1995.52.383. [DOI] [PubMed] [Google Scholar]
- 14.Senbanjo IO, Adeodu OO, Ogunlesi TA, Anyabolu CH, Okusanya AA. The use of antimalaria drugs and insecticide treated nets in Ile-Ife, Nigeria. Niger J Med. 2006;15:277–80. doi: 10.4314/njm.v15i3.37228. [DOI] [PubMed] [Google Scholar]
- 15.Iyaniwura CA, Ariba A, Runshewe-Abiodun T. Knowledge, use and promotion of insecticide treated nets by health workers in a suburban town in south-western Nigeria. Niger J Clin Pract. 2008;11:149–54. [PubMed] [Google Scholar]
- 16.Onwujekwe OE, Akpala CO, Ghasi S, Shu EN, Okonkwo PO. How do rural households perceive and prioritize malaria and mosquito nets? A study of five communities of Nigeria. Public Health. 2000;114:407–10. [PubMed] [Google Scholar]
- 17.Park K. Park's Textbook of Preventive and Social Medicine. 20th ed. Jabalpur, India: Banarsidas Bhanot Publishers; 2009. Medicine and Social Science; pp. 595–8. [Google Scholar]
- 18.Araoye MO. Research Methodology with Statistics for Health and Social Sciences. 1st ed. Ilorin: Nathadex Publishers; 2004. Sample size determination; pp. 115–21. [Google Scholar]
- 19.Omoigberale AI, Airauhi LU. Aspects of the epidemiology of intestinal parasitoses (IP) in children: knowledge, practices and perceptions of mothers. Niger J Clin Pract. 2006;9:109–13. [PubMed] [Google Scholar]
- 20.Netmark. Netmark baseline survey on insecticide treated materials (ITMs) in Nigeria. NetMark. 2001 [Google Scholar]
- 21.Holtz TH, Marum LH, Mkandala C, Chizani N, Roberts JM, Macheso A, et al. Insecticide-treated bednet use, anaemia and malaria parasitaemia in Blantyre District, Malawi. Trop Med Int Health. 2002;7:220–30. doi: 10.1046/j.1365-3156.2002.00846.x. [DOI] [PubMed] [Google Scholar]
- 22.Nganda RY, Drakeley C, Reyburn H, Marchant T. Knowledge of malaria influences the use of insecticide treated nets but not intermittent presumptive treatment by pregnant women in Tanzania. Malaria J. 2004;3:42. doi: 10.1186/1475-2875-3-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mbagaya GM, Odhiambo MO, Oniango RR. Mother's health seeking behaviour during child illness in a rural Western Kenya community. Afr Health Sci. 2005;5:322–7. doi: 10.5555/afhs.2005.5.4.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Alaii JA, Hawley WA, Kolczak MS, ter kiule FO, Giming JE, Vulule JM, et al. Factors affecting the use of permethrin-treated bed nets during a randomized controlled trial in western Kenya. Am J Trop Med Hyg. 2003;68:137–41. [PubMed] [Google Scholar]
- 25.Inem AV, Ayankogbe OO, Obazee M, Ladipo MM, Udonwa NE, Odusote K. Conceptual and contextual paradigm of the family as a unit of care. Niger Med Pract. 2004;45:9–13. [Google Scholar]
- 26.Ordinioha B. The use of insecticide-treated bed net in a semi-urban community in South Nigeria. Niger J Med. 2007;16:223–6. [PubMed] [Google Scholar]