

Abstract
Background:
This study aimed to determine the profile of morbidity among elderly registered at home health care service in the Armed Forces Hospital of Southern Region, Kingdom of Saudi Arabia.
Materials and Methods:
A retrospective study was conducted (over a period of 6 months during year 2011) and data was collected by reviewing of medical records of all elderly patients of elderly.
Results:
The total number of elderly ≥ 60 years were 880. The most prevalent morbidity is hypertension (59.1%) followed by diabetes mellitus (57.3%), stroke (34.9%), dementia (28.5%), osteoarthritis (24.2%) and Alzheimer (21.4%). Females are at higher risks of having many types elderly diseases compared to males. The highest risk was for obesity (OR = 9.1; 95% CI = 3.51- 12.8), followed by osteoporosis (OR = 8.7; 95% CI = 15.10 – 9.13) and fracture neck femur (OR = 3.9; 95 CI = 2.11 – 6.91). In addition, females were also at higher risks of having Osteoarthritis and thyroid disorder. On the other hand, males are more susceptible to hypertension (OR = 1.4; 95 % CI = 1.07 – 1.85), stroke (OR = 1.3; 95 % CI = 1.08 – 1.89) and renal diseases (OR = 2.4; 95% CI = 1.25 – 4.54).
Conclusion:
It is concluded that there is a great need for preventive, curative and rehabilitative program in order to introduce high quality of health care services to elderly.
Keywords: Elderly population, morbidity, South of Saudi Arabia
INTRODUCTION
Home care has grown into a vital source of health care, especially for elderly, who represent the highest percent of recipients. In recent years, there has been a dramatic increase in the number of older persons worldwide[1] and more old people are alive nowadays than at any time in history.[2] The proportion of the population aged 60 and over, is also growing each year. By the year 2025, the world will host 1.2 billion people aged 60 and over and rising to 1.9 billion in 2050.[3] In Saudi Arabia, elderly account for 3.5% of the total population.[4]
The risk of having chronic diseases rises as the proportion of elderly people increases. Chronic diseases cause medical, social and psychological problems that limit the activities of elderly people in the community.[5,6]
Assessment of the morbidity profile will help in the application of interventions, to improve the health status and the quality of life of the elderly. Yet there is little or no baseline information on the prevalence of chronic disease in this population.[7] The lack of such information on health trends can inhibit accurate predictions for future health care needs in this age group. Therefore it is necessity to obtain correct and up-to-date data to plan health services for the elderly.[8,9]
The importance of early surveillance of the health needs of elderly people has been emphasized.[9]
The objective of this study is to evaluate the morbidity profile among the elderly patients attending home care health services in the Armed Forces Hospital in southern region of Saudi Arabia.
MATERIALS AND METHODS
This is a retrospective descriptive study where data is obtained by reviewing the medical records of all patients registered at the home care health service in the Armed Forces Hospital in southern region of Saudi Arabia.
The present study included the geriatric population of 60 years and above who are indicated for home health care services as the target population. These indications were: any elderly who are home bound due to a major operation or chronic illness or severely physically disabled or had recent car accidents.
The data were collected by physicians in the department of home health care service during a study period of 6 months of the year 2011.
The clinical diagnoses of individual patients were taken according to the referring physician reports. The written diagnoses were reviewed. All investigations for each patient were also reviewed. The total numbers of co morbidities were calculated according to the written diagnoses.
Data entry and analysis were performed using Statistical Package for the Social Sciences Program (SPSS) - 16th Edition.
The appropriate statistical tests were used accordingly. A P value of < 0.05 was considered to be significant
RESULTS
Demographic characteristics
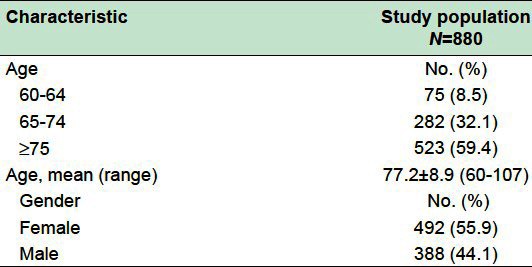
Table 1 portrays demographic characteristics of elderly group (≥60 years). The age of elderly ranges from 60-104 years with a mean of 77.2 ± 8.9. More than half (59.4%) of them with age ≥75 years. Most of the elderly (55.9%) are females.
Table 1.
Demographic characteristics of study elderly group
Morbidity profiles
There is a high level of co-morbidity, of the total elderly group 11% had one morbidity and 89% had two or more morbidity distributed as following: Two chronic diseases experienced by 16.5%, three conditions by 21.8% and four or more conditions by 50.7% of the elderly population. The number of elderly morbid conditions ranged from 1-7 diseases with a mean of 3.7 ± 1.7 [Figure 1].
Figure 1.
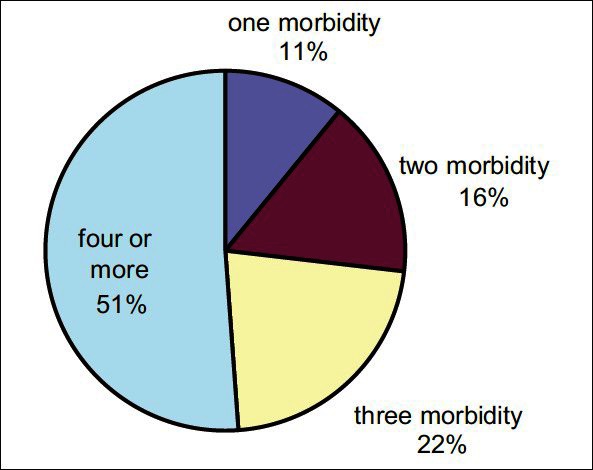
Percentage of co-morbidity among the elderly group
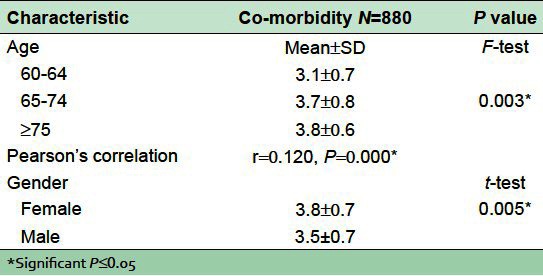
Table 2 illustrates the relationship between the numbers of co-morbidities and the demographic variables. Higher number of co-morbidities is observed among females compared to males with a statistical significant difference (t = 2.8, P = 0.005). Regarding the effect of age, higher mean co-morbidities is noticed with advancing age and a statistical significant difference is present (F = 5.7, P = 0.003) also there is a highly significant direct correlation between number of co-morbidity and advance age (r = 0.120, P = 0.000).
Table 2.
Association between demographic variables and morbidities among elderly
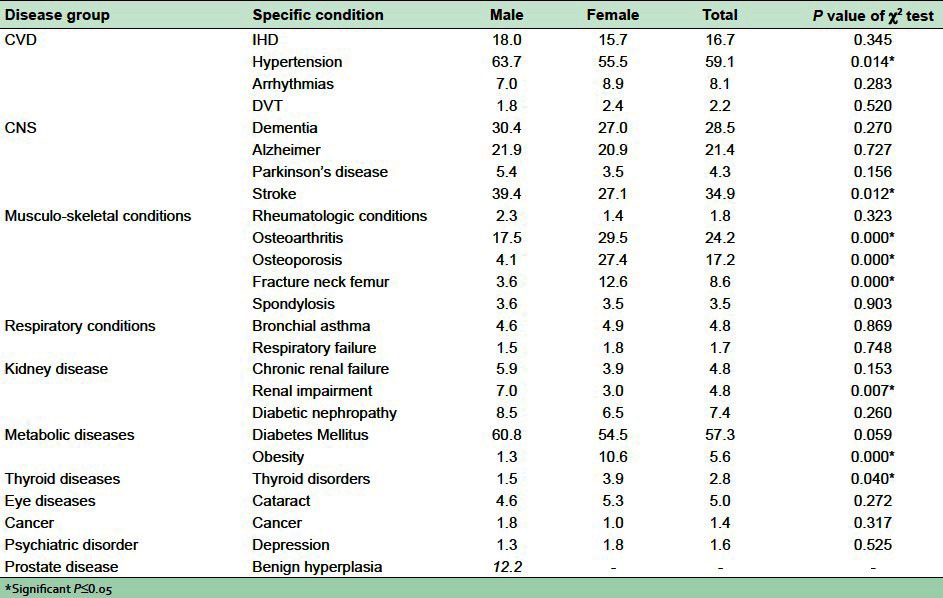
A total of 25 morbidities were reported in this study; the most prevalent is hypertension (59.1%) followed by diabetes mellitus (57.3%), stroke (34.9%), dementia (28.5%), osteoarthritis (24.2%), alzheimer (21.4%), osteoporosis (17.2%) and ischemic heart diseases (16.7%). Other diseases occurred among 4-8% of study population as arrhythmias, fracture neck femur, diabetic nephropathy, obesity, bronchial asthma, chronic renal failure and Parkinson's disease occurred in.
Most of the morbidities have the same percent in both genders. Some diseases show significant (P < 0.005) high prevalence among males such as hypertension, stroke and renal impairment. Their prevalence among males 63.7%, 39.4% and 7.0% respectively compared to females 55.5%, 34.9% and 3.0% respectively. Diseases of the musculoskeletal system, such as arthritis, osteoporosis and fracture neck femur are more significantly prevalent among females; also obesity and thyroid disorder are more significantly prevalent in females (10.6% and 3.9% respectively). Whereas diseases of the prostate are only present among men, it account for 12.2% of elderly males. Depression and cancer were reported among less than 2% of patients [Table 3].
Table 3.
Gender-wise distribution of morbidity conditions among elderly people attending home health service, southwest, Saudi Arabia
Regarding the complications of the most prevalent two morbidities among the elderly group, the most prevalent complication of hypertension is stroke (41.9%). and the most prevalent complication is diabetic nephropathy (12.5%).
The relationship between the most prevalent significant morbidities and the gender is tested. Females are at higher risks of having many types elderly diseases compared to males. The highest risk was for obesity (OR = 9.1; 95% CI = 3.51-12.8), followed by osteoporosis (OR = 8.7; 95% CI = 15.10 – 9.13) and fracture neck femur (OR = 3.9; 95% CI = 2.11 – 6.91). In addition, females were also at higher risks of having Osteoarthritis and thyroid disorder. On the other hand, males are more susceptible to hypertension (OR = 1.4; 95 % CI = 1.07 – 1.85), stroke (OR = 1.3; 95 % CI = 1.08 – 1.89) and renal diseases (OR = 2.4; 95 % CI = 1.25 – 4.54).
DISCUSSION
Co-morbidity is common in elderly persons and is associated with more rapid declines in health status and a greater likelihood of disability. Also; high rates of co-morbidity present a challenge in providing care to elderly.[10,11]
This study demonstrated that the majority of the elderly people in South of Saudi Arabia had a high numbers of co morbidity. It was observed that average number of diseases per person was 3.7 ± 1.7, this average is a slightly less in a study conducted in Jeddah (2.1 ± 1.2).[12] Other studies among elderly in North and South India reported the number of co morbidity as 2.6 ± 1.4.[13] Our study revealed that 89% of elderly had 2 or more co morbidity. This number is much less in other studies (ranges from 56 to 65%).[12,14,15]
Over the last twenty years, Saudi Arabia has witnessed major socioeconomic development leading to significant changes in its standard of living and lifestyle. The transformation of the society has also resulted in changes in dietary habits and related social practices. This has been compounded by a lack of exercise among large segments of the society. These factors and others have contributed to the emergence of life style-related diseases, including hypertension, diabetes mellitus, arthritis and osteoporosis.[16]
In this study hypertension was the most common among these morbidities and is also found to be more prevalent among males than females this is in agreement with findings from other studies (73.6% and 67.9% among males)[16,17] Reported gender differences may result from biological differences, but they may be due to other sociodemographic, comorbidity, obesity confounding effect. A systematic review showed that overall worldwide prevalence of hypertension, however, showed no significant gender difference.[18]
Diabetes is one of the growing health problems in the elderly population in the world and in the Middle East region in general and Saudi Arabia in particular.[19–22] Results of the present study revealed that diabetes mellitus was the second common chronic disease (57.3%) diagnosed among elderly patients. Al-Nozha et al., 2004,[23] in a National Community Based Survey in the Saudi Arabia found that the prevalence of diabetes among elderly population aged 60-70 years was 36.5 % and other 14.9 % showed impaired glucose tolerance. The higher figures obtained from the present study may be because the age of elderly in present study ranged from 60-107 years and not just elderly 60-70 and as it is known there is an increase in the rates of diabetes with advanced age, or the difference could be due to that the present study conducted among elderly patients not among the general elderly population.
The diabetic foot is still a common health problem which affects the patient's quality of life, especially after amputation. The prevalence of diabetic foot among attending diabetic patients in this study was 6.2%. Other studies showed that the prevalence ranges from 4% to 10% in different countries.[24–27]
Among Saudi diabetic patients, the prevalence of retinopathy is 31% after a mean duration of diabetes greater than 10 years.[28] our study shows so much less prevalence among diabetic elderly (1.7%). This low prevalence may be attributed to that not all diabetic patient were undergone fundscopy. However, to date no study has examined screening strategies for diabetic retinopathy in Saudi patients.
Diseases of the musculoskeletal system, arthritis and osteoporosis, ranked as the fourth (29.5%) and the fifth (27.4%) most prevalent diseases among elderly females, and this difference is found to be statistically highly significant. This might be due to the post-menopausal osteoporotic changes among females. A study by Jain[29] and Padda[13] had reported higher percent of arthritis among females 54.2% and 60.1% respectively. A study by Moharana found that, 37.0% of females were having osteoarthritis.[30]
Results of the current study showed that IHD was more encountered among males compared to females and 16.7% of elderly had these diseases. Results from the National Community Based Survey in the Saudi Arabia revealed that male gender was a risk factor of IHD and the prevalence among elderly aged 60-70 years was lower (9.3 %).[31] This difference may be due to differences in the age group or the type of the target population.
Present results showed that 28.5% of elderly had dementia and 21.4 of them had Al Zheimer disease which coincides with the percentage reported among elderly in Jeddah (25.6%).[12] Other international studies[32,33] showed less prevalence (10.3% and 13% respectively). These results suggest that Alzheimer's disease is a common condition and that its public health impact will continue to increase with increasing longevity of the population.
Several studies of the dementia and Alzheimer's disease have found no significant difference by gender.[34–36] Our study also supports this finding.
Several studies of obesity in Saudi Arabia have indicated a significantly higher prevalence of obesity among females than among males.[37–39] Our study showed similar results.
The prevalence of depression among elderly in our study was 1.6%. Other study showed a higher prevalence (4.6%).[40] However, both prevalence cannot be directly compared due to the difference of the study design and target population. Furthermore, our data were collected largely based on medical records, whereas the previous study employed ‘Diagnostic Manual of Mental Disorders, fourth edition (DSM-IV)’ for assessing depression. So, further studies are necessary to clarify this issue.
CONCLUSION
This study revealed that elderly attending home care facilities in southern region were suffering from many chronic disorders. Such common co-morbidities need preventive, curative and rehabilitative program in improving the quality of life among elderly patients in home care setting.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Hafez G, Bagchi K, Mahaini R. Caring for the elderly: A report on the status of care for the elderly in the Eastern Mediterranean Region. East Mediterr Health J. 2000;6:636–43. [PubMed] [Google Scholar]
- 2.McMurdo ME. A healthy old age: Realistic or futile goal? BMJ. 2000;321:1149–51. doi: 10.1136/bmj.321.7269.1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.New York: United Nations Population Division; 2003. World Population Prospects: The 2002 Revision, Highlights. ESA/P/WP 180. [Google Scholar]
- 4.Saudi Arabian population census. 2004 [Google Scholar]
- 5.Resnick NM. Appleton and Lange. 39th ed. USA: 1999. Geriatric Medicine, Current Medicine and Treatment; pp. 47–70. [Google Scholar]
- 6.Mobbs C. The Merck Manual of Geriatrics. [Last accessed on 2011 Feb 16]. Available from: http://www.merck.com/pubs/mm_geriatrics/sec2/ch2.htm .
- 7.Allain TJ, Wilson AO, Gomo ZA, Mushangi E, Senzanje B, Adamchak DJ, et al. Morbidity and disability in elderly Zimbabweans. Age Ageing. 1997;26:115–21. doi: 10.1093/ageing/26.2.115. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organisation. Life in the 21st Century. A Vision of Everyone, WHO. 1998 [Google Scholar]
- 9.World Health Organisation. The World Health Report 2000, Health Systems: Improving Performance. WHO. 2000 [Google Scholar]
- 10.Fillenbaum GG. Comorbidity of five chronic health conditions in elderly community residents: determinants and impact on mortality. J Gerontol A Biol Sci Med Sci. 2000;55:84–9. doi: 10.1093/gerona/55.2.m84. [DOI] [PubMed] [Google Scholar]
- 11.Grau L, Kovner C. Comorbidity, Age, and Hospital Use among Elderly Medicare Patients. J Aging Health August. 1991;3:352–67. doi: 10.1177/089826439100300303. [DOI] [PubMed] [Google Scholar]
- 12.Ibrahim NK, Ghabrah TM, Qadi M. Morbidity profile of elderly attended/admitted in Jeddah health facilities, Saudi Arabia. Bull High Inst Public Health. 2005;35:173–90. [Google Scholar]
- 13.Padda AS. Health profile of aged persons in urban and rural field practice areas of Medical College, Amritsar. Indian J Community Med. 1998;13:72–6. [Google Scholar]
- 14.AL-Doghether MH, AL-Megbil TI. Determinants of prescribing for the elderly in primary health care. Middle East J Fam Med. 2004;2:1–5. [Google Scholar]
- 15.Jennifer L, Wolff MH, Starfield B. Prevalence, Expenditures, and Complications of Multiple Chronic Conditions in the Elderly. Arch Intern Med. 2002;162:2269–76. doi: 10.1001/archinte.162.20.2269. [DOI] [PubMed] [Google Scholar]
- 16.Bani IA. Prevalence and related risk factors of Essential Hypertension in Jazan region, Saudi Arabia. Sudanese J Public Health. 2011;6:45–50. [Google Scholar]
- 17.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou YY, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28:77–84. [PubMed] [Google Scholar]
- 18.Kearney P, Whelton M, Reynolds K, Muntner P. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–23. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- 19.Ahmed A. Review on the prevalence of Diabetic Foot and its Risk Factors in Saudi Arabia. Middle East J Fam Med. 2009;7:29–34. [Google Scholar]
- 20.Hossain P, Kawar B, El Nahas M. Obesity and Diabetes in the Developing World- A Growing Challenge. N Engl J Med. 2007;356:213–5. doi: 10.1056/NEJMp068177. [DOI] [PubMed] [Google Scholar]
- 21.Chang J, Malik V, Jia W, Kadowaki T, Yajnik C, Hoyoor K, et al. Diabetes in Asia, Epidemilology, Risk factors, and pathophysiology. JAMA. 2009;301:2129–40. doi: 10.1001/jama.2009.726. [DOI] [PubMed] [Google Scholar]
- 22.Mokdad A, Ford E, Bowman B, Dietz W, Vinicor F, Bales V, et al. Prevalence of obesity, Diabeters, and obesity related health risk factors. JAMA. 2003;289:76–9. doi: 10.1001/jama.289.1.76. [DOI] [PubMed] [Google Scholar]
- 23.Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25:1603–10. [PubMed] [Google Scholar]
- 24.Singh N, Armstrong D, Lipsky B. Preventing Foot ulcers in patients with Diabetes. JAMA. 2005;293:217–28. doi: 10.1001/jama.293.2.217. [DOI] [PubMed] [Google Scholar]
- 25.Malgrange D, Richard JL, Leymarie F. French Working Group on the Diabetic Foot. Screening Diabetic patients at risk for foot ulceration. A multi-centre hospital based study in France. Diabetes Metab. 2003;29:261–8. doi: 10.1016/s1262-3636(07)70035-6. [DOI] [PubMed] [Google Scholar]
- 26.Desonnaville J, Colly L, Wijkel D, Heine R. The Prevalence and determinant of foot ulceration in type 2 diabetic patients in a primary health care setting. Diabetes Res Clin Pract. 1997;35:149–56. doi: 10.1016/s0168-8227(97)01380-6. [DOI] [PubMed] [Google Scholar]
- 27.Ribe L, Rustoen T, Birelard R, Honestard R, Paul S, Miaskowski C. The Prevalence and occurrence of diabetic foot ulcer pain and its impact on health related quality of life. J Pain. 2006;7:290–99. doi: 10.1016/j.jpain.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 28.Abu El Asrar AM, Al-Rubean KA, Al-Amro SA, Kangave D. Risk factors for diabetic retinopathy among Saudi diabetics. Int Ophthalmol. 1999;22:155–61. doi: 10.1023/a:1006240928938. [DOI] [PubMed] [Google Scholar]
- 29.Jain NC, Pawar AB, Hadiya Ravjibhai, Bansal RK. Morbidity profile of elderly people in slums of surat city. Natl J Community Med. 2010;1:52–4. [Google Scholar]
- 30.Moharana PR, Sahani NC, Sahu T. Health status of geriatric population attending the preventive geriatrics clinic of a tertiary health facility. J Community Med. 2008;4:22–6. [Google Scholar]
- 31.Al-Nozha MM, Arafah MR, Al-Mazrou YY, Al-Maatouq MA, Khan NB, Khalil MZ, et al. Coronary artery disease in Saudi Arabia. Saudi Med J. 2004;25:1165–71. [PubMed] [Google Scholar]
- 32.Evans DA, Funkenstein HH, Albert MS, Scherr PA, Cook NR, Chown MJ, et al. Prevalence of Alzheimer's disease in a community population of older persons. Higher than previously reported. JAMA. 1989;262:2551–6. [PubMed] [Google Scholar]
- 33.Alzheimer's Association, 2010 Alzheimer's Disease Facts and Figures, Alzheimer's and Dementia. [Last accessed on 2011 Apr 18];6 Available from: http://www.alz.org . [Google Scholar]
- 34.Fratigilioni L, forsellio Y. Prevalence of Alzheimer's disease and other dementias in an elderly urban population: Relationship with age, sex, and education. Neurology. 1991;41:188–96. doi: 10.1212/wnl.41.12.1886. [DOI] [PubMed] [Google Scholar]
- 35.Barnes LL, Wilson RS, Schneider JA, Bienias JL, Evans DA, Bennett DA. Gender, cognitive decline and risk of AD in older persons. Neurology. 2003;60:1777–81. doi: 10.1212/01.wnl.0000065892.67099.2a. [DOI] [PubMed] [Google Scholar]
- 36.Hebert LE, Scherr PA, McCann JJ, Becket LA, Evans DA. “Is the risk of developing Alzheimer's disease greater for women than for men?”. Am J Epidemiol. 2001;153:132–13. doi: 10.1093/aje/153.2.132. [DOI] [PubMed] [Google Scholar]
- 37.Al-Shammari SA. High prevalence of clinical obesity among Saudi females: a prospective, cross-sectional study in the Riyadh region. J Trop Med Hyg. 1993;97:183–8. [PubMed] [Google Scholar]
- 38.Al-Abbad FA, Al-Sowielem S. Prevalence of obesity. Saudi Med J. 1998;19:608–13. [Google Scholar]
- 39.Ogbeide DO. The prevalence of overweight and obesity and its correlation with chronic diseases in Al-Kharj adult outpatients, Saudi Arabia. Saudi Med J. 1996;17:327–32. [Google Scholar]
- 40.Abolfotouh MA, Daffallah AA, Khan MY, Khattab MS, Abdulmoneim I. Psychosocial assessment of geriatric subjects in Abha City, Saudi Arabia. East Mediterr Health J. 2001;3:481–91. [PubMed] [Google Scholar]