

Abstract
Extramammary Paget's disease is uncommon. Diagnosis has to be confirmed by histopathology. Treatment is a challenge in cases with extended tumors. We present a 70-year-old male patient with extensive genitoanal Paget's disease. Mohs surgery is the gold standard in such cases. Details of the surgical planning are discussed including wound bed preparation. Radiotherapy may be an alternative.
KEYWORDS: Apocrine malignancy, Extramammary Paget's disease, Mohs surgery, transplantation
INTRODUCTION
Invasive extramammary Paget's disease (IEMPD) is uncommon. The predominant area of development is the anogenital region followed by the axillary skin. It affects mainly elderly people.[1]
Basically, this tumor is an adenocarcinoma of apocrine gland origin. Histopathology demonstrates large single cells or cell nests throughout the epidermis in Paget's disease. Tumor cells are positive for periodic-acid-Schiff stain (PAS), cytokeratin 7 (CK7), and carcino-embryonal antigen (CEA) but remain negative for S100 or HMB-45. Immunohistology helps to distinguish IEMPD for pagetoid melanoma (S100 and HMB-45 positive, but CK7, CEA, and PAS negative).[2]
Six different patterns of Paget cell proliferation have been described. Upper nests or a mixture of at least three patterns has been considered as suggestive for IEMPD.[3] IEMPD shows a complete loss of Wnt (wingless-type MMTV integration site)-5α.[4] In addition, several protein kinases involved in the c-Jun amino-terminal kinase pathway are overexpressed in IEMPD: Hematopoietic progenitor kinase-1, mitogen-activated protein/extracellular signal-related protein kinase kinase kinase-1, and phosphomitogen-activated protein kinase kinase-4.[5] The over expression of HER-2/neu (c-erbB-2) is correlated to invasiveness of lymph node metastasis.[6]
European age standardized incidence of EMPD is 0.6 per 1000,000 person years. Five-year relative survival for invasive EMPD is 91.2%. Among European patients 8.6% developed other malignancies.[7] The percentage of secondary tumours is 14.4% in South Korea.[8] The highest increased risk of developing a second primary tumour was found in the first year of follow-up or being female. These findings argue for thorough search for other tumours during follow-up.[7,8]
CASE REPORT
A 70-year-old Causasian male patient of good general health presented with a persistent scaling erythematous lesion on his groins with ill-defined margins. He reported no itching or other subjective symptoms. The lesions were slow growing for more than 5 years. Topical treatment with corticosteroids or anti-mycotics had not improved the cutaneous appearance. His personal and family medical history was unremarkable.
On examination we observed an extensive erythematous lesion of groins, perineum and proximal parts of scrotal skin with peripheral scaling and central oozing [Figure 1]. Inguinal lymph nodes were not palpable.
Figure 1.

Clinical aspect of extensive extramammary invasive Pagetæs disease with involvement of groins scrotum and perineum
Laboratory investigations were unremarkable except a slightly increase level of carcinoembryonal antigen (CEA) of 2.2 μg/L. Microbial swabs were taken for bacterial cultures but remained sterile. We took a diagnostic biopsy from the left groin in the centre of the lesions. It was suggesting Paget's disease.
Diagnostic ultrasound for lymph nodes demonstrated some enlarged nodes. A control was suggested. The ultrasound control 6 weeks later was normal. Screening for second tumour including skin (total body investigation including dermoscopy), lung (computerized tomography), prostate (digital examination, ultrasound and prostate-specific antigen), and GIT (coloscopy) remained negative.
Treatment and course: We performed complete surgical excision with delayed Mohs techniques [Figure 2]. The histopathological work-up revealed a Paget carcinoma (apocrine adenocarcinoma) surrounded by intraepidermal Paget's disease [Figure 3]. The invasive part was completely excised with the 1st surgery. Paget's disease was noticed in minor parts of the surgical margins. Therefore, re-excision of the margins was done twice with delayed Mohs technique, i.e., complete examination of all margins. Controls demonstrated no Paget's residues. The distance between surgical border and anal verge was 2 cm. Wound bed was prepared by repeated topical CO2 application under plastic foil for 20 min. Hereby granulation was improved. The resulting defect was closed by split-skin mesh-graft and the scrotum was partially reconstructed by extension of scrotal skin [Figure 4]. The healing was uneventful and the outcome was functionally and esthetical very good [Figure 5].
Figure 2a.
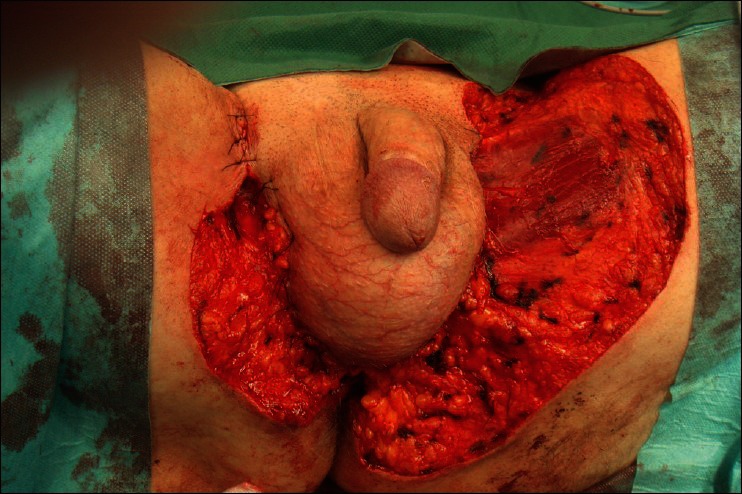
Surgical situs after Mohs surgery
Figure 3.
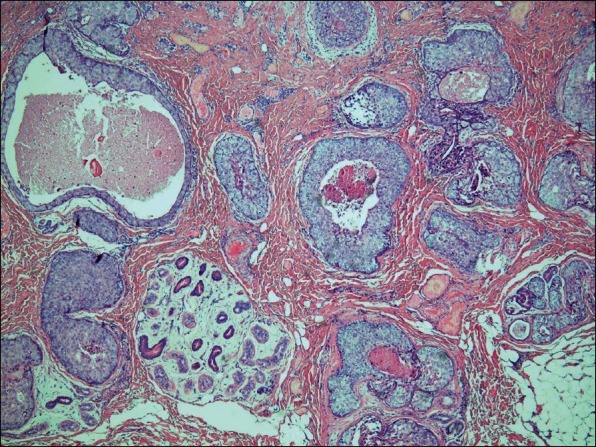
Histopathology of the tumor with pagetoid cell proliferations and invasive growth (H and E, ×4)
Figure 4.
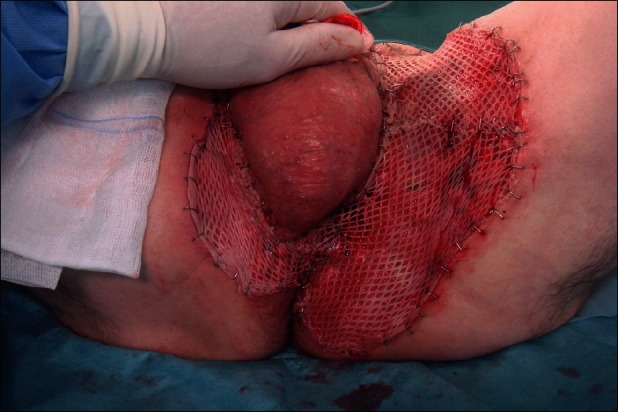
Mesh-graft split skin transplantation after induction of granulation by topical CO2
Figure 5.

Good functional and esthetic outcome
Figure 2b.

The excised tumor
During follow-up of three months the patient was relapse-free. A regular follow-up every 3 months during the first year and twice a year for a total of five years is planned.
DISCUSSION
Extramammary Paget's disease is uncommon. The differential diagnosis includes inverse psoriasis, eczema, intertrigio, tinea and mycosis fungoides. The anogenital region is the most common involved area, but scrotal disease is less common.[1,9]
Standard therapy is complete surgical excision with 2 cm to 5 cm safety margin or Mohs surgery.[10–13] Mohs surgery may be supported by immunostaining for cytokeratin 17 expressed by EMPD.[14] Recurrence rates after standard surgical excision range from 33% to 62.5% versus 16% to 28% after Mohs surgery.[11–13]
Non-surgical treatments have been used either in non-invasive EMPD or recurrent EMPD. Topical imiquimod may produce long-term remissions in smaller tumors but not in all.[14–17] Photodynamic therapy fails to achieve complete remissions especially in larger tumours.[18,19] Other options include topical 5-fluorouracil, topical bleomycin, CO2-laser, docetaxel, and radiotherapy.[1,20]
Whereas surgery remains the golden standard, in extensive disease defect closure may become difficult. Various techniques have been used including split skin mesh graft transplants with or without vacuum-assisted closure, and a number of flaps, especially when deep arteries are exposed.[1,10,21,22] Although flaps allow a rapid closure of defects, the long term outcome of pendiculated flaps often bears the risk of local lymphedema. This can be circumvented by preparation of wound ground and delayed split skin grafting as in our case. We use repeated topical CO2 application to improve granulation of wound bed tissue.[23]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Lam C, Funaro D. Extramammary Paget's disease: Summary of current knowledge. Dermatol Clin. 2010;28:807–26. doi: 10.1016/j.det.2010.08.002. [DOI] [PubMed] [Google Scholar]
- 2.Castelli E, Wollina U, Anzarone A, Morello V, Tomasino RM. Extrammary Paget disease of the axilla associated with comedo-like apocrine carcinoma in situ. Am J Dermatopathol. 2002;24:351–7. doi: 10.1097/00000372-200208000-00013. [DOI] [PubMed] [Google Scholar]
- 3.Shiomi T, Yoshida Y, Shomori K, Yamamoto O, Ito H. Extramammary Paget's disease: Evaluation of the histopathological patterns of Paget cell proliferation in the epidermis. J Dermatol. 2011;38:1054–7. doi: 10.1111/j.1346-8138.2011.01268.x. [DOI] [PubMed] [Google Scholar]
- 4.Xie L, Hayashida S, Furue M. Loss of Wnt-5α is associated with an invasive phenotype of extramammary Paget's disease. J Cutan Pathol. 2011;38:576–80. doi: 10.1111/j.1600-0560.2011.01689.x. [DOI] [PubMed] [Google Scholar]
- 5.Quian Y, Takeuchi S, Dugu L, Tsuji G, Xie L, Nakahara T, et al. Hematopoietic progenitor kinase 1, mitogen-activated protein/extra cellular signal-related protein kinase kinase kinase 1, and phosphomitogen-activated protein kinase kinase 4 are over expressed in extramammary Paget disease. Am J Dermatopathol. 2011;33:681–6. doi: 10.1097/DAD.0b013e318215c3fb. [DOI] [PubMed] [Google Scholar]
- 6.Masuguchi S, Jinnin M, Fukushima S, Makino T, Sakai K, Inoue Y, et al. The expression of HER-2 in extramammary Paget's disease. Biosci Trends. 2011;5:151–5. doi: 10.5582/bst.2011.v5.4.151. [DOI] [PubMed] [Google Scholar]
- 7.van der Zwan JM, Siesling S, Blokx WA, Pierie JP, Capocaccia R. Invasive extramammary Paget's disease and the risk for secondary tumours in Europe. Eur J Surg Oncol. 2012;38:214–21. doi: 10.1016/j.ejso.2011.12.008. [DOI] [PubMed] [Google Scholar]
- 8.Lee SJ, Choe YS, Jung HD, Ahn SK, Cha YC, Cho KH, et al. A multicenter study on extramammary Paget's disease in Korea. Int J Dermatol. 2011;50:508–15. doi: 10.1111/j.1365-4632.2010.04661.x. [DOI] [PubMed] [Google Scholar]
- 9.Zhang N, Gong K, Zhang X, Yang Y, Na Y. Extramammary Paget's disease of scrotum--report of 25 cases and literature review. Urol Oncol. 2010;28:28–33. doi: 10.1016/j.urolonc.2008.07.002. [DOI] [PubMed] [Google Scholar]
- 10.Kyriazanos ID, Stamos NP, Miliadis L, Noussis G, Stoidis CN. Extra-mammary Paget's disease of the perianal region: A review of the literature emphasizing the operative management technique. Surg Oncol. 2011;20:e61–71. doi: 10.1016/j.suronc.2010.09.005. [DOI] [PubMed] [Google Scholar]
- 11.Boehringer A, Leiter U, Metzler G, Moehrle M, Garbe C, Breuninger H. Extramammary Paget's disease: Extended subclinical growth detected using three-dimensional histology in routine paraffin procedure and course of the disease. Dermatol Surg. 2011;37:1417–26. doi: 10.1111/j.1524-4725.2011.02091.x. [DOI] [PubMed] [Google Scholar]
- 12.Hendi A, Brodland DG, Zitelli JA. Extramammary Paget's disease: Surgical treatment with mohs micrographic surgery. J Am Acad Dermatol. 2004;51:767–73. doi: 10.1016/j.jaad.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 13.Coldiron BM, Goldsmith BA, Robinson JK. Surgical treatment of extramammary Paget's disease. A report of six cases and a re-examination of Mohs micrographic surgery compared with conventional surgical excision. Cancer. 1991;67:933–8. doi: 10.1002/1097-0142(19910215)67:4<933::aid-cncr2820670413>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 14.Petrie MS, Hess S, Benedetto AV. Automated 15-minute cytokeratin 7 immunostaining protocol for extramammary Paget's disease in Mohs micrographic surgery. Dermatol Surg. 2011;37:1811–5. doi: 10.1111/j.1524-4725.2011.02181.x. [DOI] [PubMed] [Google Scholar]
- 15.Feldmeyer L, Kerl K, Kamarashev J, de Viragh P, French LE. Treatment of vulvar Paget disease with topical imiquimod: A case report and review of the literature. J Dermatol Case Rep. 2011;5:42–6. doi: 10.3315/jdcr.2011.1073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jim On SC, Izumi AK. Extramammary Paget disease: Failure to respond to topical imiquimod 5% J Am Acad Dermatol. 2011;65:656–7. doi: 10.1016/j.jaad.2010.04.035. [DOI] [PubMed] [Google Scholar]
- 17.Green JS, Burkemper NM, Fosko SW. Failure of extensive extramammary Paget disease of the inguinal area to clear with imiquimod cream, 5%: Possible progression to invasive disease during therapy. Arch Dermatol. 2011;147:704–8. doi: 10.1001/archdermatol.2011.121. [DOI] [PubMed] [Google Scholar]
- 18.Nardelli AA, Stafinski T, Menon D. Effectiveness of photodynamic therapy for mammary and extra-mammary Paget's disease: A state of the science review. BMC Dermatol. 2011;11:13. doi: 10.1186/1471-5945-11-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Al Yousef A, Boccara O, Moyal-Barracco M, Zimmermann U, Saiag P. Incomplete efficacy of 5-aminolevulinic acid (5 ALA) photodynamic therapy in the treatment of widespread extramammary Paget's disease. Photodermatol Photoimmunol Photomed. 2012;28:53–5. doi: 10.1111/j.1600-0781.2011.00635.x. [DOI] [PubMed] [Google Scholar]
- 20.Nakamori R, Omoto Y, Yamanaka K, Habe K, Korokawa I, Mizutani H. Complete remission of advanced extramammary Paget's disease treated with docetaxel: A case report. Clin Exp Dermatol. 2012;37:194–5. doi: 10.1111/j.1365-2230.2011.04204.x. [DOI] [PubMed] [Google Scholar]
- 21.Fang BR, Ameet H, Li XF, Lu Q, Wang XC, Zeng A, et al. Pedicled thinned deep inferior epigastric artery perforator flap for perineal reconstruction: A preliminary report. J Plast Reconstr Aesthet Surg. 2011;64:1627–34. doi: 10.1016/j.bjps.2011.04.013. [DOI] [PubMed] [Google Scholar]
- 22.Nakamura Y, Ishitsuka Y, Nakamura Y, Xu X, Hori-Yamada E, Ito M, et al. Modified gluteal-fold flap for the reconstruction of vulvovaginal defects. Int J Dermatol. 2010;49:1182–7. doi: 10.1111/j.1365-4632.2010.04578.x. [DOI] [PubMed] [Google Scholar]
- 23.Wollina U, Heinig B, Uhlemann C. Transdermal CO2 applications in chronic wounds. Int J Low Extrem Wounds. 2004;3:103–6. doi: 10.1177/1534734604265142. [DOI] [PubMed] [Google Scholar]