

Abstract
Purpose
There is no report about psychopathological effect causing by disc herniation. The disease could impose psychopathological influence on the social life, the treatment period, and response to the treatment. This study was to evaluate retrospectively the psychopathological influence of lumbar disc herniation (LDH) among Korean 19-year-old males.
Materials and Methods
We compared the Korean military multiphasic personality inventory (KMPI) profiles of 74 LDH cases with the KMPI profiles of 150 controls. The LDH groups were categorized to 2 groups according to the presence of thecal sac compression by disc materials, and evaluated the relation between the KMPI and LDH.
Results
The decrease of the faking-good response scale and increase of the faking-bad response scale were observed more in the LDH group than in the normal volunteer group (p<0.05). The neurosis set such as anxiety, depression and somatization was markedly increased in the LDH group compared to the normal volunteers group (p<0.05). The scale of personality disorder was also increased more in the LDH group (p=0.002). The differences of KMPI scales were not correlated with the severe pathology of LDH.
Conclusion
Young male with LDH may tend to have more abnormal results of multiphasic personality inventory test compared to the normal volunteers, suggesting that LDH may be related to the psychopathology in young males in Korea. Therefore, clinicians are recommended to evaluate and treat the psychopathological aspects in patients with LDH.
Keywords: Lumbar disc herniation, multiphasic personal inventory, psychopathology, lumbar disc herniation, conscription
INTRODUCTION
Lumbar disc herniation (LDH) is a disabling and painful disease that affects all ages causing untold suffering, diminished quality of life, and enormous economic limitation. The influence of psychological variables in spinal disease has been extensively researched for long times.1-6 Many studies have reported that depression and other abnormal psychological attitude are an inadequate predictor of defective outcome of spinal surgery or rehabilitation. However, to our best knowledge, there are no published series documenting the personality effect caused by LDH. We, therefore, reviewed the result of multiphasic personal inventory test to check psychological influence of LDH in Korean male adolescent.
MATERIALS AND METHODS
Since Korea has adopted the conscription system, all men are examined for the conscription at the Military Manpower Administration (MMA) at 19 years of age. In the examination of conscription, all examinees are evaluated with Korean military multiphasic personality inventory (KMPI). We were able to collect the data of normal volunteers with no spinal diseases and examinees with LDH. All examinees for this study were 19-year-old males who were admitted to the department of neurosurgery at Seoul Regional MMA from April 2011 to December 2011. All participants consented that this data could be used for the study. This study was conducted with the approval of the committee in the MMA in Seoul and it was approved by ethical committee of MMA.
The volunteers (150 cases) were interviewed by a neurosurgeon who confirmed that they had neither psychological problem, nor medical visit for spinal problems. Also, lumbar magnetic resolution images were checked to confirm any spinal disease such as LDH, spondylolisthesis, spondylolysis, and etc. The examinees with LDH (74 cases) had already been diagnosed by magnetic resolution images in the area of lumbar spine, and LDH was confirmed by the lumbar computed tomography. According to these imaging data, LDH group was categorized into two groups: the absence and the presence of the thecal sac compressing disc. We classified adolescent LDH into four groups of herniation severity as it is required by the guideline issued by the Korean military directorate, as shown in Table 1.7 Severity of lumbar disc herniation was categorized according to the Korean military guideline, and this guideline categorized all medical conditions into 7 physical grades (MMA physical grade). This directorate categorize status of lumbar disc herniation as normal (MMA physical grade 1), mild disc bulging without compression of the thecal sac (MMA physical grade 2), disc protrusion or extrusion without compression of the thecal sac (MMA physical grade 3), disc protrusion or extrusion with compression of thecal sac (MMA physical grade 4), disc protrusion or extrusion with spinal canal compromise of more than 50% (MMA physical grade 4), and disc protrusion or extrusion with a positive cut-off sign (MMA physical grade 5).7 In the present study, severities of lumbar disc herniation were categorized as mild or severe according to the presence of thecal sac compression. In this study, to avoid psychopathological effect by the operation, the cases with post-operated LDH were excluded from this study.
Table 1.
Classification of Adolescent Herniated Lumbar Disks as Required by Guideline Issued by the Korean Military Medical Directorate
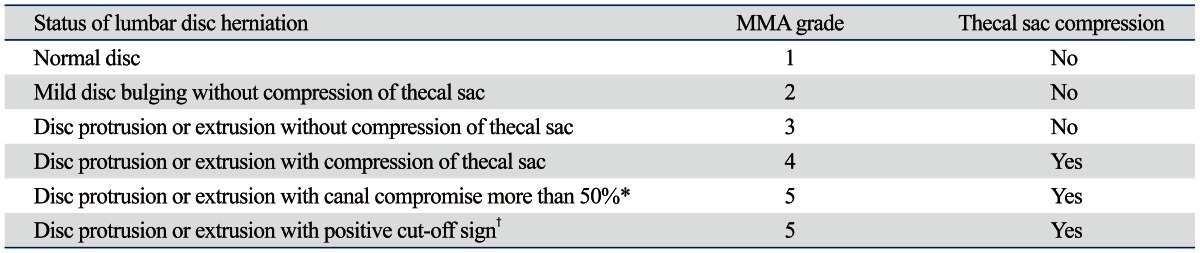
MMA, Military Manpower Administration.
*Spinal canal stenosis was defined as the narrowing of the spinal canal by >50% of the mid-sagittal diameter (front to back) in the same plane.
†Cut-off was defined as the loss of neuromuscular signal at the level of interest identified by imaging.
KMPI is a conventional type of Minnesota multiphasic personality inventory test (MMPI) by adjusting for Korean conscription. Several subjects were analyzed in KMPI, including response set, neurosis set, psycopathy set, accident set, prediction set of accident, and special set. If one of any exceeded or lacked any one of the criteria, it was categorized to abnormal results of KMPI by computer. In this study, we divided the category of abnormal results in 3 separate sets: response set (faking-good response, faking-bad response, and infrequency scale), neurosis set (anxiety, depression, and somatization), psychopathy set (schizophrenia, personality disorder, and paranoid). Evaluation of the statistical significance of difference was carried out using Student t-test. Tests were considered significant at p-values less than 0.05. The statistical comparisons were analyzed with SPSS 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
All the examinees (224 cases) were 19-year-old Korean males and none of the examinees had any psychological problems. The agreement rate of KMPI was check in both groups; 51.81±8.51 (95% CI 50.81 to 52.80) was checked in the volunteer group, and 52.32±8.91 (95% CI 51.59 to 53.05) was checked in the LDH group. However, the agreement rate of KMPI was not statistically significantly different (p=0.146). In the normal volunteer group, the spinal diseases such as LDH, spondylolisthesis, and spondylolysis were not observed. In the LDH group, LDH had already been diagnosed and confirmed by image studies. Among them, 57 cases were observed as non compressing thecal sac lesion by LDH, and 17 cases were observed as compressing thecal sac lesion by LDH.
Table 2 summarized the results of KMPI in the normal volunteer group and LDH group. The proportion of abnormal results, the response set, the neurosis set, and the psychopathy set of KMPI was compared between the two groups. There were more abnormal results in the LDH group (18.9%, 95% CI 14.3% to 23.5%) than in the normal volunteers group (9.3%, 95% CI 6.9% to 11.7%, p=0.042). In the results of KMPI, the faking-good response scale and bad response scale, the neurosis set (anxiety, depression, and somatization scale), and the scale of personality disorder were significantly different between the two groups. Whereas the faking-good response scale was decreased in the LDH group (p=0.028), the faking-bad response was increased in the LDH group (p=0.004). The infrequent scale did non differ among the two groups. In the neurosis set, all scales of anxiety, depression, and somatization were markedly increased in the LDH group compared with the normal volunteers group (p=0.017, 0.000, 0.000). In the psychopathy set, only the scale of personality disorder was increased more in the LDH group (p=0.002), while the other scales were not different.
Table 2.
The Results of Korean Military Multiphasic Inventory Test in the Normal Volunteers Group and the Lumbar Disc Herniation Group [Mean±Standard Deviation (95% Confidence Intervals)]
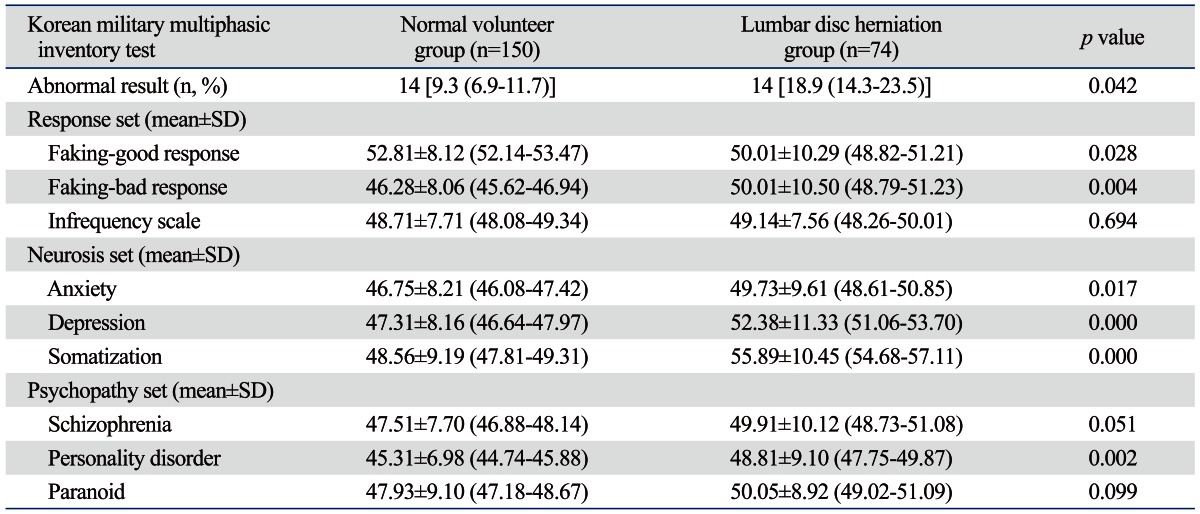
SD, standard deviation.
According to the presence and abscence of the thecal sac compressing disc, the cases in LDH group were divided into two subgroups. There were 57 cases in the group of the presence of the thecal sac compressing disc and 17 cases in the group of the absence of the thecal sac compressing disc. Table 3 shows the results of KMPI in the two subgroups of the LDH group. There were no significant differences in all scales between the two groups.
Table 3.
The Result of Korean Military Multiphasic Inventory Test in the Two Subgroups of Lumbar Disc Herniation Group [Mean±Standard Deviation (95% Confidence Intervals)]
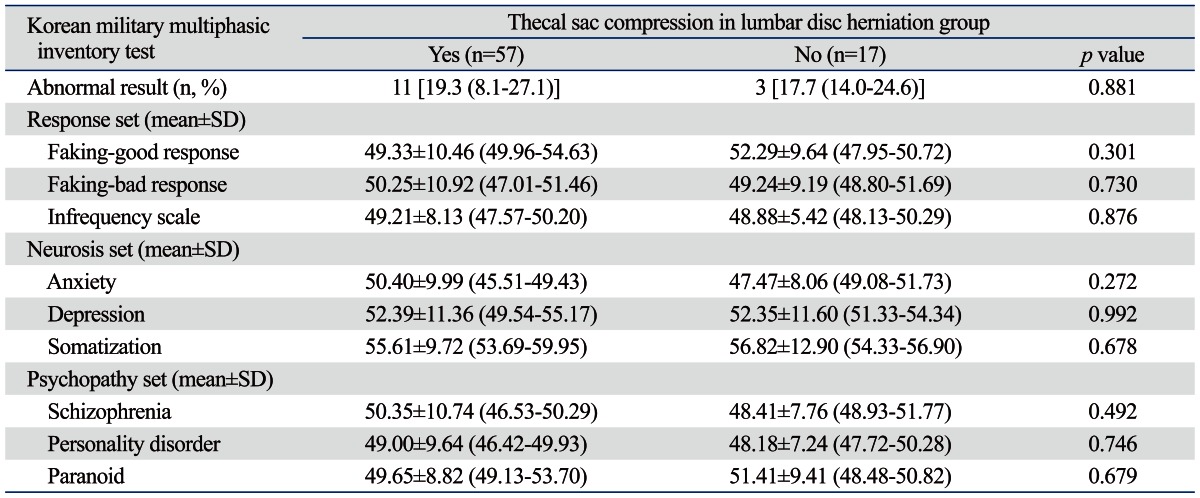
SD, standard deviation.
DISCUSSION
To identify one's personality structure and psychopathology, the multiphasic personality inventory is a useful personality test.8 The MMPI is the most frequently used personality tests in mental health,9,10 and it is widely used to investigate personality structure and psychopathology in various fields; it is even used in law to identify the malingering claims. However, this test is not common in neurosurgical field as there are only a few published literatures about psychopathological abnormality in patients with spinal disease.1-6,11,12
In the MMPI, ten types of clinical scales were described, and it composed as hypochondriasis (concern with bodily symptoms), depression (depressive symptoms), hysteria (awareness of problems and vulnerabilities), psychopathic deviate (conflict, struggle, anger, respect for society's rules), masculinity/femininity (stereotypical masculine or feminine interests/behavior), paranoia (level of trust, suspiciousness, sensitivity), psychasthenia (worry, anxiety, tension, doubts, obsessiveness), schizophrenia (odd thinking and social alienation), hypomania (level of excitability), and social introversion (people orientation), as the authors described in previous studies.13,14 The analysis of the MMPI focuses on relative elevation of profiles. So, these profiles could compared to profiles of various normal groups. Raw scores of the scales were T-scores which presented standardized metric scores.
KMPI is a conventional Korean conscription adjusted type of MMPI.14 It was created via several stages. First, several military-associated questions were added to pre-existing MMPI, and a pre-test with 575 questions was performed to normal soldiers, normal university students, military prisoners, military hospital psychiatric patients and private hospital psychiatric patients. Afterwards, the validity scale, clinical scale and content scale were established and divided into several profiles similar to MMPI, and the scores were standardized and distinct functions were yielded. Thus, KMPI shows overall some aspects similar to MMPI and set scores on each scales which were transformed into standardized metric scores, known as T-scores.15 By comparing T-scores of each group, one can easily measure the tendency of personality structures and psychopathology.15
In this study, we used only 4 sets of KMPI. First, the response set was composed of faking-good response, faking-bad response, and infrequently response scale. People can fake good (faking-good response) when they feel that it would serve their interests. Therefore, the fakeing-good people may be tempted to skew their answers in a way that they feel it will put them in a good light. The opposite is known as the faking-bad. The infrequent response scale is a scale intended to detect infrequent responding among the psychopathological populations. Second, the neurosis set is composed of anxiety, depression, and somatization scale. These scales present the tendency of each neurotic status. Third, the psychopathy set is composed of schizophrenia, personality disorder, and paranoid scale. These scales also present the tendency of each social relation status.
In the literature review, the multiphasic personal inventory test was usually used to predict the outcomes of spinal surgeries. Most of these studies indicated that depression, anxiety, and hostility all predict several surgical outcomes, and recommended presurgical psychological treatment to improves the outcome.1-6 Herron, et al.1 also reported that hypochondriasis, hysteria, psychopathic deviate, paranoia, psychasthenia, schizophrenia, hypomania, and social introversion scales are good predictors of chemonucleolysis outcome and much better predictors of ultimate outcome. On the other hand, however, there are some reports that contradict these hypotheses.12,16 Cashion and Lynch16 prospectively evaluated a battery of psychological tests in patients undergoing a surgery for LDH, and found that the degree of psychological testing does not definitely predict outcome. This substantiates the recommendation for its further use in registry systems, quality management projects, and clinical trials.11
As shown in Table 2, the proportion of abnormal results was markedly increased in the LDH group compared to the normal volunteers group, suggesting that LDH could be a trigger of abnormal personality or psychopathology. Furthermore, the faking-good response was decreased while the faking-bad response was increased in the LDH group. The neurosis set such as anxiety, depression and somatization was markedly increased in the LDH group. Also, the scale of personality disorder was increased more in the LDH group. Similar result was reported by Boos, et al.,17 who followed up 46 asymptomatic individuals with general psychological assessment for about 5 years. They assessed the psychosocial influence with the Psychological General Well-Being questionnaire, and found that it was related to general exhausted state of the individual, similar negative influence of this recent study.
The result of personal inventory test in the LDH group was significantly different from the result of the normal volunteers group, and the severe pathology of LDH could be considered as a trigger to abnormal personality or psychopathology. In the present study, however, these scales were not correlated with the severe pathology of LDH (Table 3), in good agreement with the result of Taylor, et al.12 Among the patients who were considered for cervical disc surgery, the depressed patients did not have any more severe organic pathology, neurological symptoms or sign, or disablement. Depressive disorder is not secondary to severe pathology. The other scales (faking-good and behavioral retardation) were first reported among LDH in this study.
There are some limitations in this study. First of all, KMPI is not documented or analyzed by literatures as widely as it should have been because its purpose was for a unique environment such as military conscription.18 But, this KMPI is officially approved by the Korean government, which does not differ from the MMPI.14 Secondly, this study by using the military conscription data was a cross sectional study and only males were involved. Indeed, this study lacks of comparison data between preoperative and postoperative status, which could indicate strong relation between the psychopathological influence and LDH. Therefore, these results should not be interpreted as a hasty generalization, but considered as a possibility of psychopathogical influence. Despite of its limitations, multiphasic personal inventory test may be a meaningful way to identify the personality changes or psychopathologies in the LDH patients.
In conclusion, young males with LDH may tend to have more abnormal results of multiphasic personal inventory test, including the faking-good response, the depression, and the behavioral retardation, compared to normal volunteers. This suggests that LDH may be related to psychopathology in young males in Korea. Therefore, clinicians may be recommended to evaluate psychopathological aspects in patients with LDH.
ACKNOWLEDGEMENTS
This work was supported by an Inha University Research Grant.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Herron LD, Turner JA, Weiner P. Lumbar disc herniations: the predictive value of the Health Attribution Test (HAT) and the Minnesota Multiphasic Personality Inventory (MMPI) J Spinal Disord. 1988;1:2–8. [PubMed] [Google Scholar]
- 2.Celestin J, Edwards RR, Jamison RN. Pretreatment psychosocial variables as predictors of outcomes following lumbar surgery and spinal cord stimulation: a systematic review and literature synthesis. Pain Med. 2009;10:639–653. doi: 10.1111/j.1526-4637.2009.00632.x. [DOI] [PubMed] [Google Scholar]
- 3.Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine (Phila Pa 1976) 2002;27:E109–E120. doi: 10.1097/00007632-200203010-00017. [DOI] [PubMed] [Google Scholar]
- 4.Trief PM, Grant W, Fredrickson B. A prospective study of psychological predictors of lumbar surgery outcome. Spine (Phila Pa 1976) 2000;25:2616–2621. doi: 10.1097/00007632-200010150-00012. [DOI] [PubMed] [Google Scholar]
- 5.Sinikallio S, Lehto SM, Aalto T, Airaksinen O, Kröger H, Viinamäki H. Depressive symptoms during rehabilitation period predict poor outcome of lumbar spinal stenosis surgery: a two-year perspective. BMC Musculoskelet Disord. 2010;11:152. doi: 10.1186/1471-2474-11-152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aalto TJ, Malmivaara A, Kovacs F, Herno A, Alen M, Salmi L, et al. Preoperative predictors for postoperative clinical outcome in lumbar spinal stenosis: systematic review. Spine (Phila Pa 1976) 2006;31:E648–E663. doi: 10.1097/01.brs.0000231727.88477.da. [DOI] [PubMed] [Google Scholar]
- 7.Kim DK, Oh CH, Lee MS, Yoon SH, Park HC, Park CO. Prevalence of lumbar disc herniation in adolescent males in Seoul, Korea: prevalence of adolescent LDH in Seoul, Korea. Korean J Spine. 2011;8:261–266. doi: 10.14245/kjs.2011.8.4.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wolf EJ, Miller MW, Orazem RJ, Weierich MR, Castillo DT, Milford J, et al. The MMPI-2 restructured clinical scales in the assessment of posttraumatic stress disorder and comorbid disorders. Psychol Assess. 2008;20:327–340. doi: 10.1037/a0012948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.van Balen HG, de Mey HR, van Limbeek J. A neurocorrective approach for MMPI-2 use with brain-damaged patients. Int J Rehabil Res. 1999;22:249–259. doi: 10.1097/00004356-199912000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Wetzel RD, Guze SB, Cloninger CR, Martin RL, Clayton PJ. Briquet's syndrome (hysteria) is both a somatoform and a "psychoform" illness: a Minnesota Multiphasic Personality Inventory study. Psychosom Med. 1994;56:564–569. doi: 10.1097/00006842-199411000-00013. [DOI] [PubMed] [Google Scholar]
- 11.Mannion AF, Elfering A, Staerkle R, Junge A, Grob D, Dvorak J, et al. Predictors of multidimensional outcome after spinal surgery. Eur Spine J. 2007;16:777–786. doi: 10.1007/s00586-006-0255-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Taylor RE, Creed F, Hughes D. Relation between psychiatric disorder and abnormal illness behaviour in patients undergoing operations for cervical discectomy. J Neurol Neurosurg Psychiatry. 1997;63:169–174. doi: 10.1136/jnnp.63.2.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reitan RM, Wolfson D. Emotional disturbances and their interaction with neuropsychological deficits. Neuropsychol Rev. 1997;7:3–19. doi: 10.1007/BF02876970. [DOI] [PubMed] [Google Scholar]
- 14.Paik HK, Oh CH, Choi K, Kim CE, Yoon SH, Chung J. Influence of history of brain disease or brain trauma on psychopathological abnormality in young male in Korea: analysis of multiphasic personal inventory test. J Korean Neurosurg Soc. 2011;50:114–118. doi: 10.3340/jkns.2011.50.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Oh CH, Lim HK, Chung J, Yoon SH, Park HC, Park CO. The psychopathological influence of congenital heart disease in Korean male adolescents: an analysis of multiphasic personal inventory test results. Yonsei Med J. 2012;53:1107–1112. doi: 10.3349/ymj.2012.53.6.1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cashion EL, Lynch WJ. Personality factors and results of lumbar disc surgery. Neurosurgery. 1979;4:141–145. doi: 10.1227/00006123-197902000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Boos N, Semmer N, Elfering A, Schade V, Gal I, Zanetti M, et al. Natural history of individuals with asymptomatic disc abnormalities in magnetic resonance imaging: predictors of low back pain-related medical consultation and work incapacity. Spine (Phila Pa 1976) 2000;25:1484–1492. doi: 10.1097/00007632-200006150-00006. [DOI] [PubMed] [Google Scholar]
- 18.Fiedler ER, Oltmanns TF, Turkheimer E. Traits associated with personality disorders and adjustment to military life: predictive validity of self and peer reports. Mil Med. 2004;169:207–211. doi: 10.7205/milmed.169.3.207. [DOI] [PMC free article] [PubMed] [Google Scholar]