

Abstract
Purpose
The main objective of this study was to evaluate the association between polymorphisms of the target genes of pemetrexed and clinical outcomes in non-small cell lung cancer (NSCLC) patients treated with pemetrexed.
Materials and Methods
We assessed polymorphisms at 8 sites in 4 genes [thymidylate synthase (TS), dihydrofolate reductase (DHFR; 1610, 680, 317, intron 1), methylenetetrahydrofolate reductase (MTHFR; 677, 1298), glycinamide ribonucleotide formyl transferase (GARFT; 2255)] associated with pemetrexed metabolism using polymerase chain reaction, gene scanning, and restriction fragment length polymorphism analysis in 90 patients with adenocarcinoma of the lung.
Results
Survival was significantly longer with pemetrexed in patients with TS 3RGCC/3RGCC or 3RGGC/3RGGC compared with the other groups (PFS; 5.2 months vs. 3.7 months, p=0.03: OS; 31.8 months vs. 18.5 months, p=0.001). Patients with DHFR 680CC experienced fatigue more frequently (50% vs. 8.6%, p=0.008). Polymorphisms of MTHFR and GARFT were not significantly associated with clinical outcomes of pemetrexed.
Conclusion
The TS genotype was associated with survival and one DHFR polymorphism was associated with fatigue in NSCLC patients treated with pemetrexed. Further large prospective studies are required to identify other biomarkers that affect patients being treated with pemetrexed for adenocarcinoma of the lung.
Keywords: Polymorphism, lung neoplasms, pemetrexed
INTRODUCTION
Pemetrexed is an important component in the treatment of advanced non-small cell lung cancer (NSCLC).1 Pemetrexed acts as a multi-targeted antifolate compound by interrupting purine biosynthesis via thymidylate synthase (TS) and dihydrofolate reductase (DHFR) inhibition and pyrimidine biosynthesis via glycinamide ribonucleotide formyl transferase (GARFT) and aminoimidazole carboxamide formyl transferase inhibition, all of which are key enzymes involved in folic acid metabolism.2
Because TS activity is high in rapidly proliferating cells,3 it is considered an ideal target for cancer chemotherapeutics. The variable number of tandem repeats (VNTR) and single nucleotide polymorphisms (SNPs) in the 5'-untranslated region (UTR) in the TS promoter have repeatedly been shown to be correlated with treatment outcomes in patients with gastrointestinal malignancies who receive fluorouracil.4 Furthermore, functional gene polymorphisms of DHFR, methylenetetrahydrofolate reductase (MTHFR), and GARFT have been shown to be correlated with outcomes in patients with rheumatoid arthritis who are treated with methotrexate.5,6
In NSCLC, TS and DHFR expressions have been associated with sensitivity to pemetrexed.7,8 Moreover, Smit, et al.9 reported that, among NSCLC patients who were treated with pemetrexed, those with MTHFR C677T had longer survival compared with patients with other genotypes. However, the prevalence of polymorphisms of key proteins in folate metabolism has been shown to differ among various ethnic populations,10 and more research is needed in Asian patients.
We hypothesized that certain SNPs of TS, DHFR, and GARFT, the key enzyme targets of pemetrexed, might be predictive markers for the efficacy and toxicity of this agent. Thus, we examined the association between TS, DHFR, and GARFT SNPs and the clinical outcomes of NSCLC patients treated with pemetrexed.
MATERIALS AND METHODS
Eligible patients and treatment
Ninety patients with advanced NSCLC were enrolled in this study. Eligible patients were those diagnosed with cytologically- or histologically-proven lung adenocarcinoma, who had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0-2, and who had previous treatment with more than one prior chemotherapy regimens for advanced NSCLC at Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Korea, from January 2007 to December 2010. Baseline characteristics were age, gender, clinical stage, ECOG PS, histological type, smoking history, and number of prior chemotherapy regimens. Histological analysis of tumors was based on the WHO classification of cell types.11 Patients received 500 mg/m2 of pemetrexed every 3 weeks until disease progression, intolerable toxicity, or patient refusal. All patients received supplementation with folic acid and vitamin B12.
Patients were evaluated every 6 weeks by computed tomography and clinical response was defined according to the response evaluation criteria of Response Evaluation Criteria In Solid Tumor (RECIST) 1.1 for patients with measurable disease.12 Toxicity was scored every 3 weeks according to the Common Toxicity Criteria-Adverse Events version 4.0. All patients had provided written informed consent and the study protocol was approved by the Institutional Review Board of Yonsei University College of Medicine (No 4- 2008-0647).
Genetic analysis
Genetic analyses were blinded to patient characteristics and clinical outcomes. Genomic DNA for analysis of polymorphisms was isolated as described previously13 from each patient's peripheral blood. DNA sequencing was performed according to the manufacturer's instructions (Applied Biosystems, Foster City, CA, USA) for all genes. Genotyping was performed for four DHFR sites (1610, 680, and 317 in the promoter, and a 19bp deletion), two sites in MTHFR (677 and 1298), one site in GARFT (2255), and the TS 5'UTR VNTR and C/G polymorphism within the third VNTR in the TS promoter. DNA amplification was performed using a PTC-200 thermocycler (MJ Research, Waltham, MA, USA). DNA sequencing was performed using a BigDye Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems, Foster City, CA, USA) on an ABI Prism 3100 DNA analyzer (Applied Biosystems, Foster City, CA, USA) for all genes. The primers used for amplification and sequencing were as follows: DHFR C1610T (sense: 5'-GCCCCCGCCGACAAAAGGGACCCTTTCTCCA-3'; antisense: 5'-GTTCACCCATAGGGTTTCC-3'), DHFR C680A (sense: 5'-CCCCCGCCGTTCATTGCAATTTAAGTGTTTCC-3'; antisense: 5'-ATACTGCCACAGGAAAAGCC-3'), DHFR A317G (sense: '-GCAGCTTTCTTCTAGTCACCC-3'; antisense: 5'-GTAGGTTCTGTCTGGGACTGG-3'), DHFR intron 19bp (sense: 5'-ATGGGACCCAAACGGGCGCA-3': antisense: 5'-AAAAGGGGAATCCAGTCGG-3'), MTHFR C677T (sense: 5'-AAGGAGGAGCTGCTGAAGATG-3'; antisense: 5'-CTTTGCCATGTCCACAGCATG-3'), MTHFR A1298C (sense: 5'-AGGACG GTGCGG TGA GAGTG-3'; antisense: 5'-CAC TTT GTG ACCATT CCG GTT TG-3'), and GARFTA2255G (sense: 5'-TTTTTCAGATGCCCAG ACCT-3'; antisense: 5'-GAGTAAGGAGCAAGTACCTTCAGC-3'). TS 5'UTR VNTR and C/G polymorphism within the third tandem repeat (sense: 5'-AAAAGGCGCGCGGAAGGGGTCCT-3'; antisense: '-TCCGAGCCGGCCACAGGCAT-3').
Statistical methods
The associations between each genotype and other categorical clinical variables were compared using the χ2 test or Fisher's exact test. Progression-free survival (PFS) was defined as the time from the start day of pemetrexed treatment until the date of tumor progression or death. Overall survival (OS) was measured from the start date of pemetrexed therapy to the date of death or final follow-up. In the absence of death, OS was defined using the time of the last visit. Survival data were estimated using a Kaplan-Meier curve and compared using the log-rank test. A p-value of less than 0.05 was considered statistically significant. SPSS software version 15.0 was used for statistical analyses (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
The demographic characteristics of the subjects are shown in Table 1. The median age of the patients was 59 years (range, 34-85), 36.7% were female, and 42.2% had never smoked. Forty-nine patients (54.4%) received pemetrexed as a second-line chemotherapy agent. The majority of patients (86.7%) had good PS (ECOG PS 0 or 1).
Table 1.
Patient Baseline Characteristics
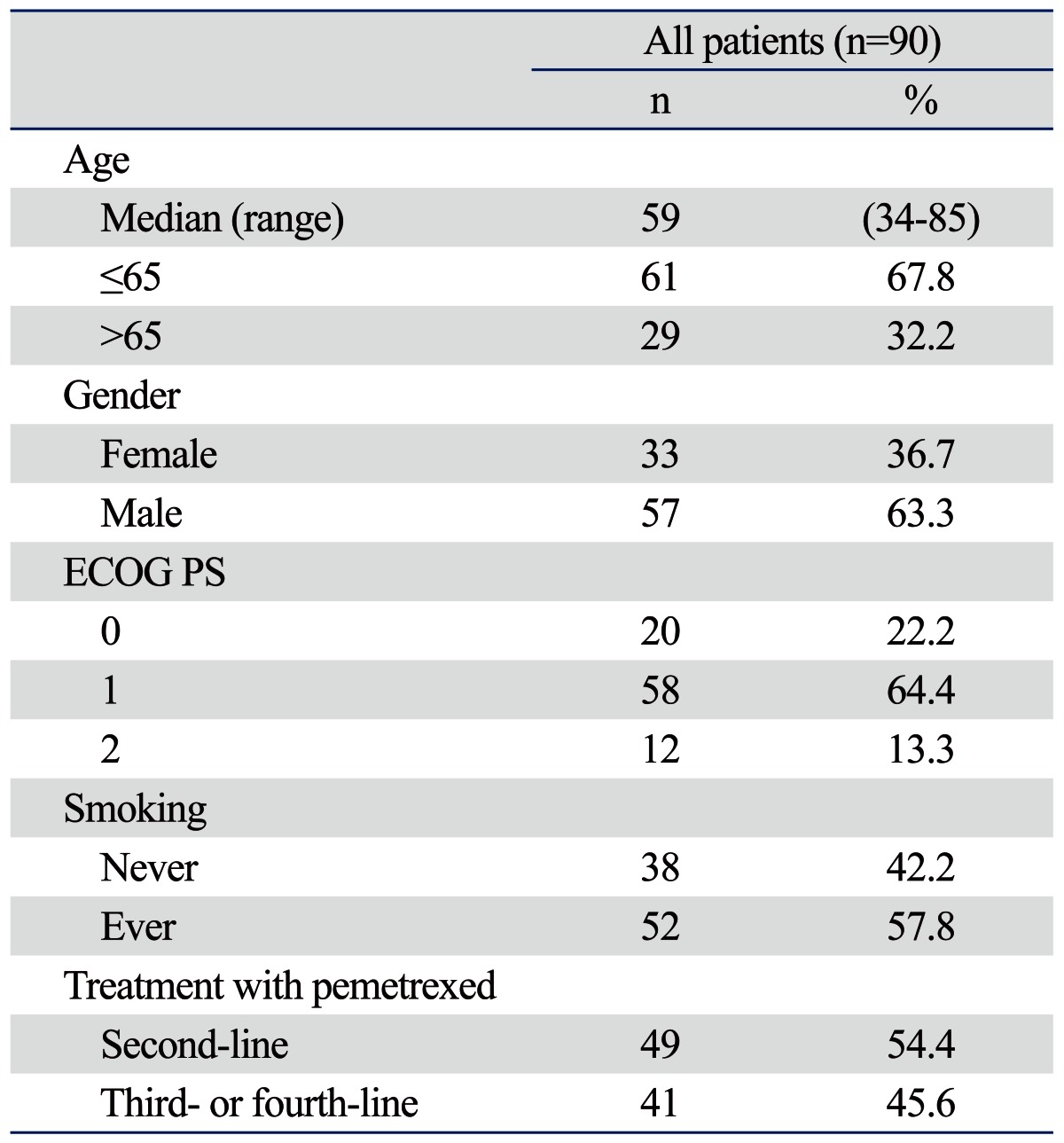
ECOG PS, Eastern Cooperative Oncology Group performance status.
Association of baseline characteristics and genotypes with response to pemetrexed therapy
Response was evaluated in 88 of 90 patients. Two patients were lost to follow-up before response evaluation. One patient achieved complete remission and 13 patients had a partial response, giving a response rate of 15.9%, and 41 patients (46.6%) had the best response, which was stability of disease. No association was found between response rate (RR) and age, gender, and smoking. However, patients with an ECOG PS 0-1 or those who were treated with pemetrexed as a second-line agent had a higher RR than patients with an ECOG PS 2 or those who were treated with pemetrexed as a third- or fourth-line agent (Table 2). On the other hand, male patients, patients with a good PS, and those who were treated with pemetrexed as a second-line agent had a higher disease control rate. Table 3 shows a comparison between the genotypes and response to pemetrexed. No significant association was found between response and any of the genotypes of DHFR, MTHFR, GARFT, or TS 5' UTR (Table 3).
Table 2.
Correlation of Baseline Characteristics with Response to Pemetrexed
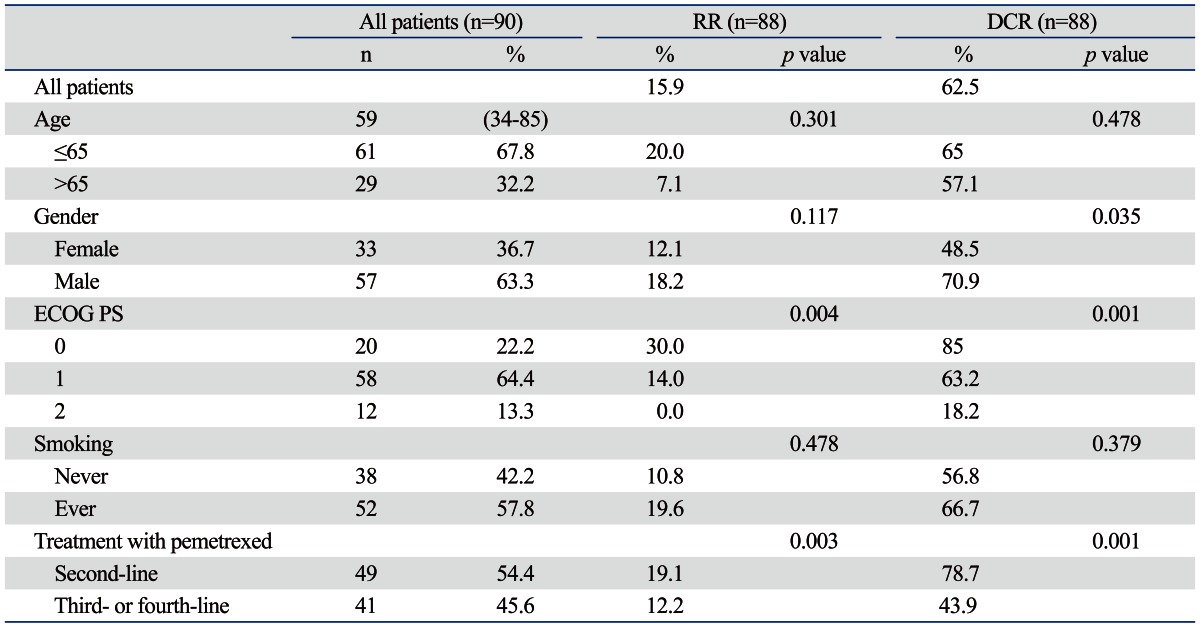
ECOG PS, Eastern Cooperative Oncology Group performance status; RR, response rate; DCR, disease control rate.
Table 3.
Correlation of Baseline Characteristics and Genetic Polymorphisms with Response to Pemetrexed
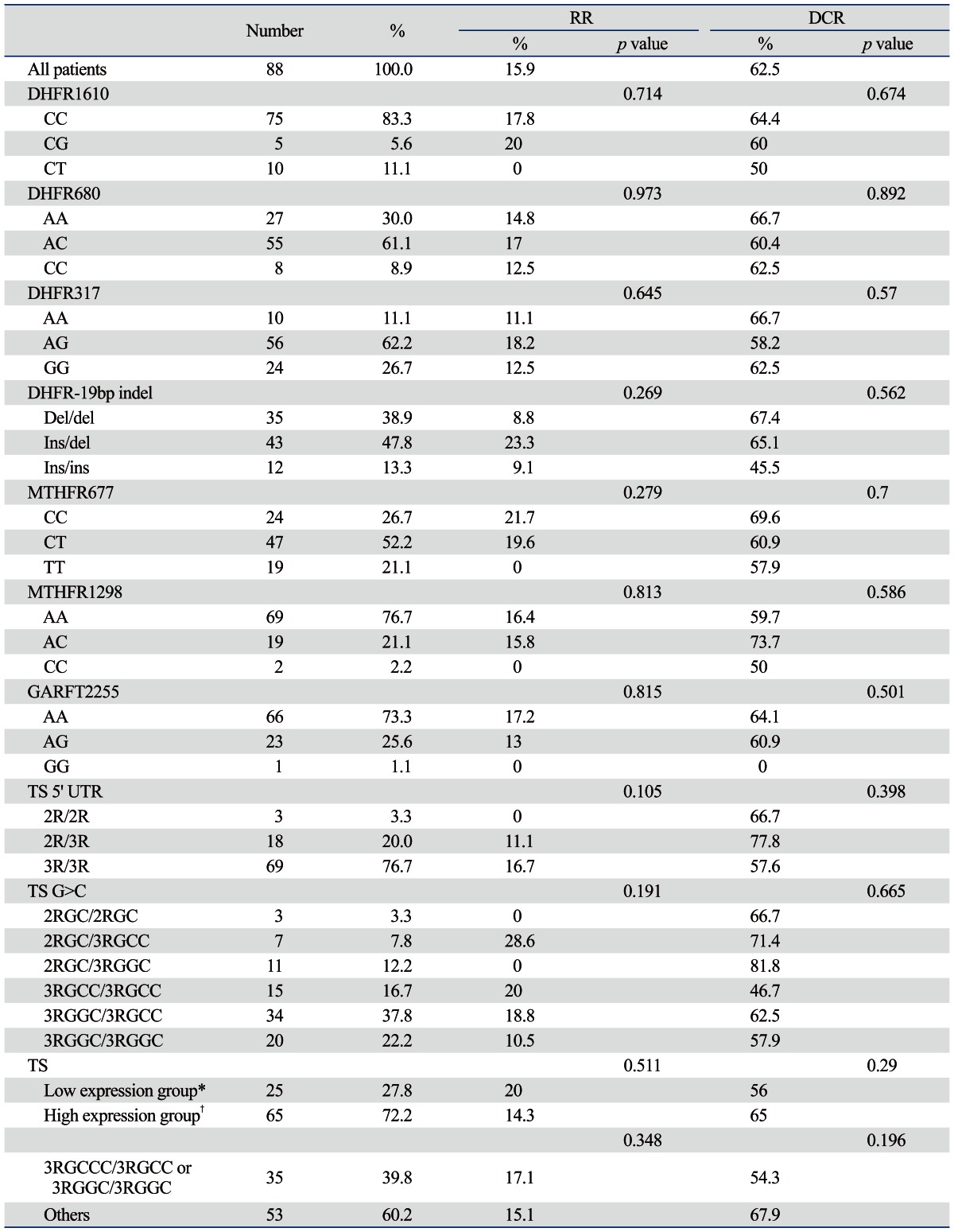
DHFR, dihydrofolate reductase; MTHFR, methylenetetrahydrofolate reductase; GARFT, glycinamide ribonucleotide formyl transferase; TS, thymidylate synthase; UTR, untranslational region; RR, response rate; DCR, disease control rate.
*2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC.
†2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC.
Association of baseline characteristics and genotypes with survival with pemetrexed therapy
In all 90 patients, the median follow-up duration was 13.4 months (range, 0.5-52.2 months). The median PFS was 4.4 months (95% CI, 0.4-13.6 months), and the median OS was 23.1 months (95% CI, 16.8-29.4 months). Patients with good PS had longer PFS and OS than the patients with an ECOG PS 2. In addition, patients treated with pemetrexed as a second-line agent had a longer PFS than those who were treated with pemetrexed as a third- or fourth-line drug. However, no significant differences were found between any each genotype itself and survival. The TS genotype was categorized into two groups: a high-expression genotype (2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC) and a low-expression genotype (2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC) as based on a previous report.14 Patients with a high expression genotype had a longer OS than those with a low-expression genotype (31.8 months vs. 21.1 months, p=0.04) (Fig. 1). In addition, 3RGCC/3RGCC or 3RGGC/3RGGC was associated with a longer PFS and OS as compared with other genotypes (PFS, 5.2 months vs. 3.7 months, p=0.03; OS, 31.8 months vs. 18.5 months, p=0.001) (Table 4 and 5, Fig. 2). Good PS and treatment with pemetrexed as a second-line agent were independent predictive markers for PFS by multivariate analysis; however, neither TS 3RGCC/3RGCC nor 3RGGC/3RGGC were independent predictive markers. In addition, good PS was significantly associated with OS by multivariate analysis; however, neither TS 3RGCC/3RGCC nor 3RGGC/3RGGC were independent predictive markers for OS.
Fig. 1.

Kaplan-Meier curve estimates for patients treated with pemetrexed. Progression-free survival (PFS) and overall survival (OS) were plotted against the expression of thymidylate synthase. Low expression group: 2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC; high expression group: 2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC. (A) PFS. (B) OS. TS, thymidylate synthase.
Table 4.
Univariate and Multivariate Analysis of Progression Free Survival
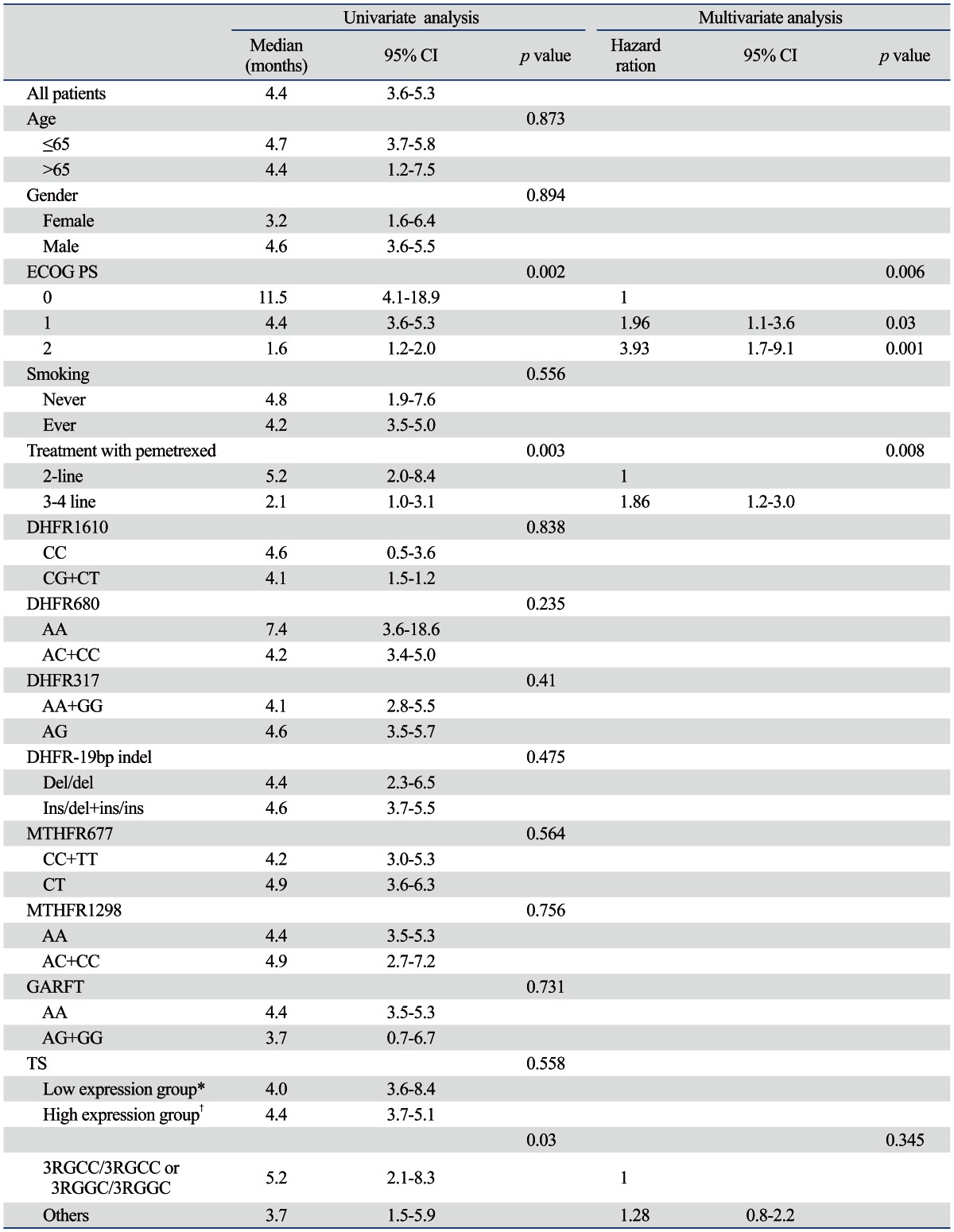
ECOG PS, Eastern Cooperative Oncology Group performance status; DHFR, dihydrofolate reductase; MTHFR, methylenetetrahydrofolate reductase; GARFT, glycinamide ribonucleotide formyl transferase; TS, thymidylate synthase; CI, confidence interval.
*2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC.
†2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC.
Table 5.
Univariate and Multivariate Analysis of Overall Survival
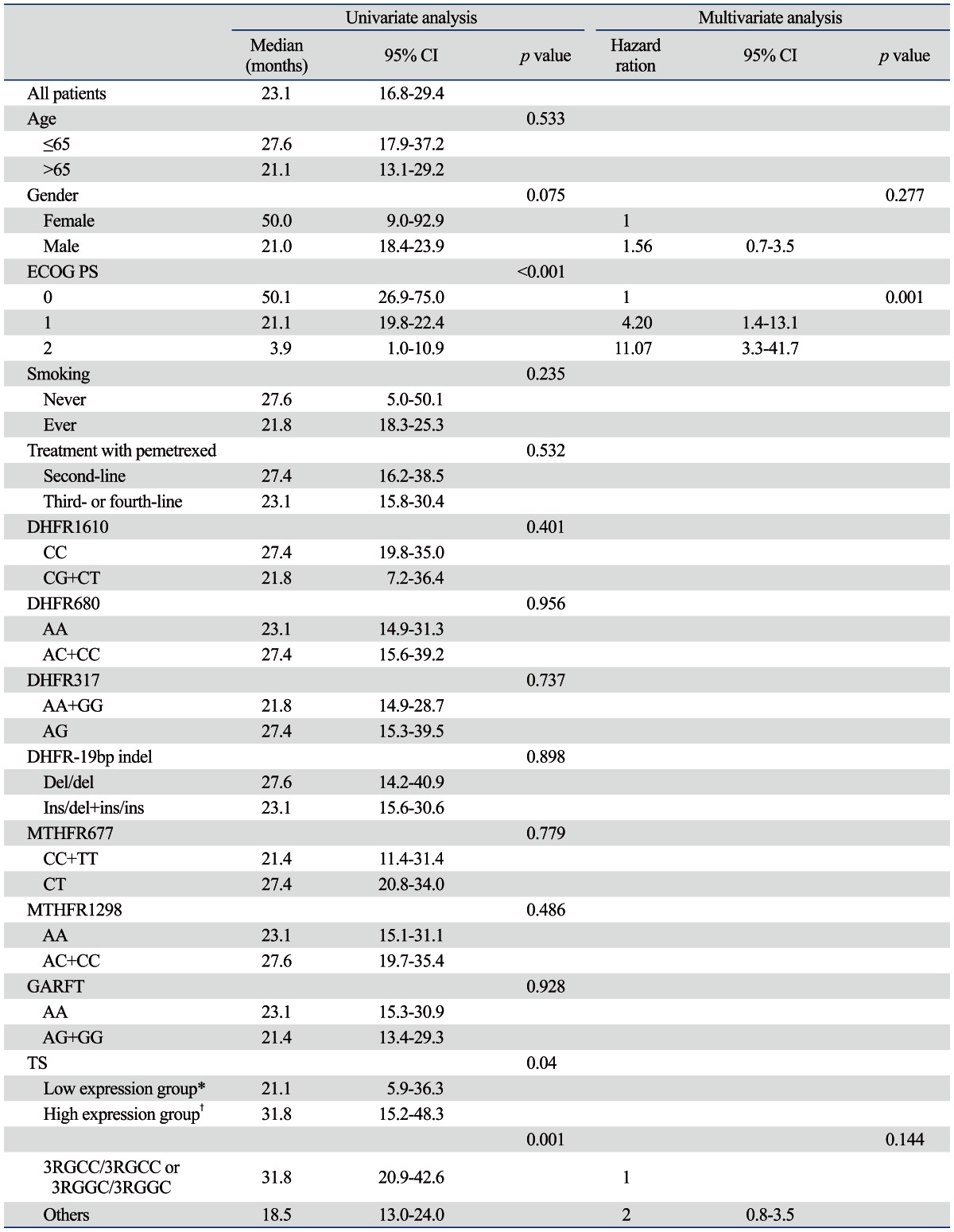
ECOG PS, Eastern Cooperative Oncology Group performance status; DHFR, dihydrofolate reductase; MTHFR, methylenetetrahydrofolate reductas; GARFT, glycinamide ribonucleotide formyl transferase; TS, thymidylate synthase; CI, confidence interval.
*2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC.
†2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC.
Fig. 2.

Kaplan-Meier curve estimates for patients treated with pemetrexed. Progression-free survival (PFS) and overall survival (OS) were plotted by genotype. Dotted line-2RCC/2RGC, 2RGC/3RGCC, 2RGC/3RGGC, 3RGCC/3RGGC; straight line-3RGCC/3RGCC and 3RGGC/3RGGC. (A) PFS. (B) OS. TS, thymidylate synthase.
Association of genotype and toxicity from pemetrexed
The frequency of pemetrexed-related toxicity was less than 5% for all categories except hematologic toxicity and fatigue. There was no grade 4 hematologic toxicity and grade 3 neutropenia, anemia, and thrombocytopenia were experienced by one patient each (Table 5). Overall, 11 patients (12.1%) experienced grade 1 or 2 fatigue. Patients with DHFR C680C experienced fatigue more commonly than those with other genotypes (50% vs. 8.6%, p=0.008) (Table 5). With the exception of fatigue, no association was found between hematologic toxicity and other genotypes.
DISCUSSION
We tested the hypothesis that genetic polymorphisms of the target enzymes of pemetrexed might be associated with its effects in the treatment of advanced lung adenocarcinoma, and found that the genotype of TS was significantly associated with survival and one DHFR polymorphism was associated with fatigue in patients treated with pemetrexed for NSCLC.
Preclinical data have previously shown that the RNA level of TS in tumors is usually lower in non-squamous NSCLC, as compared with squamous NSCLC, which may be responsible for the different activity of pemetrexed.15,16 In addition, TS is the main cellular target of pemetrexed, and the variable number of tandem repeat polymorphisms within the TS promoter has been shown to be correlated with treatment outcomes in colorectal cancer patients treated with 5-fluorouracil.4 Nief, et al.14 studied the association of TS G>C genotype with TS catalytic activity and found that the TS genotype can be classified into low expression (2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC) and high expression genotypes (2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC). They also found that both mRNA expression and protein activity were higher in cells with the high-expression genotype. In the current study, when genotypes were grouped according to VNTR (2R/2R, 2R/3R, 3R/3R) without considering the G>C polymorphisms, no significant differences could be detected in clinical outcomes for pemetrexed. However, patients with high expression genotypes by Nief's classification had longer OS than those with low expression genotypes (21.1 months vs. 31.8 months, p=0.04). Nevertheless, there was no difference of PFS according to TS genotypes by Nief's classification. Interestingly, TS 3RGCC/3RGCC and 3RGGC/3RGGC were significantly associated with both PFS and OS (Table 4 and 5, Fig. 2). According to Nief's classification, 3RGCC/3RGCC was classified into low expression genotypes and 3RGGC/3RGGC into high expression genotypes. Also, there is no report about the association between the efficacy of pemetrexed and TS genotypes by Nief's classification, except the current study. Therefore, further validation and investigation of the efficacy of pemetrexed according to the classification of TS genotypes are needed.
DHFR is the primary target of methotrexate (MTX) and pemetrexed, and any polymorphism could be related to clinical outcomes for MTX. Dulucq, et al.17 reported that DHFR promoter polymorphisms were associated with worse outcomes in acute lymphocytic leukemia. A recent study reported that DHFR gene downregulation was seen in pemetrexed-sensitive lung cancer cell lines.18 However, Uramoto, et al.19 reported no association between DHFR mRNA and protein expression and clinical response in NSCLC treated with pemetrexed. In the current study, no significant difference was observed in RR and survival according to the different polymorphisms of DHFR. Interestingly, the patients with DHFR 680CC experienced fatigue more frequently than the others (p=0.008). To our knowledge, our result is the first report of an association between DHFR polymorphisms and fatigue in pemetrexed treatment.
MTHFR is an enzyme that plays an essential role in the metabolism of folate and is also the target of pemetrexed. Two common polymorphisms associated with lower enzyme activity are 677CT and 1298AC, and the variant genotype MTHFR was found to be associated with an increased risk of various cancers.20-22 In addition, Smit, et al.9 reported that patients with MTHFR 677TT had a longer PFS than patients with other genotypes in NSCLC treated with pemetrexed. However, the current study showed no association between MTHFR genotypes and clinical outcomes or pemetrexed toxicity (Table 6).
Table 6.
Correlation of Genetic Polymorphisms with Toxicity
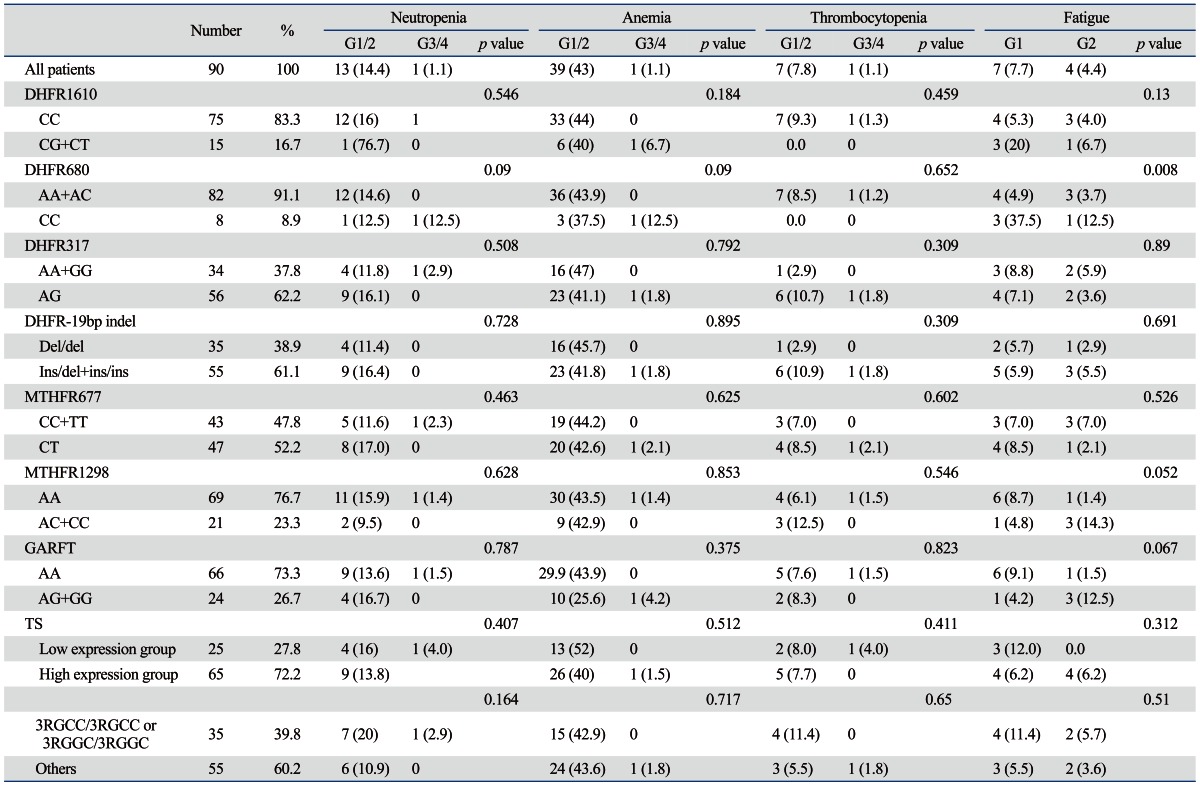
DHFR, dihydrofolate reductase; MTHFR, methylenetetrahydrofolate reductase; GARFT, glycinamide ribonucleotide formyl transferase; TS, thymidylate synthase.
Low expression group, 2RCC/2RGC, 2RGC/3RGCC, 3RGCC/3RGCC; high expression group, 2RGC/3RGGC, 3RGCC/3RGGC, 3RGGC/3RGGC.
Expression of the target enzymes of chemotherapeutic agents is expected to modulate the cytoxic effects in tumor and host cells and to affect clinical outcomes and drug toxicity. Direct quantification of target enzyme levels in tumor tissue has some methodological limitation, while genotypes of the target enzyme in peripheral blood are more easily studied. However, several clinical studies, including the current study, have failed to find a consistent correlation between target enzyme genotype and clinical outcomes in terms of therapeutic response or toxicity. Discrepancies between results might partly be due to differences in study design, tumor types, stage, ethnic differences, drug treatment, and the multifactorial nature of drug response.
In conclusion, TS 3RGG/3RGCC and 3RGGC/3RGGC are associated with survival, and DHFR 680CC is associated with fatigue in NSCLC treated with pemetrexed. However, further prospective studies will be needed to find a genetic marker that can be used in clinical practice to individualized drug therapy in NSCLC patients.
ACKNOWLEDGEMENTS
This study was supported by a faculty research grant (6-2010-0061) of Yonsei University College of Medicine.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Curtin NJ, Hughes AN. Pemetrexed disodium, a novel antifolate with multiple targets. Lancet Oncol. 2001;2:298–306. doi: 10.1016/s1470-2045(00)00325-9. [DOI] [PubMed] [Google Scholar]
- 2.Adjei AA. Pemetrexed (ALIMTA), a novel multitargeted antineoplastic agent. Clin Cancer Res. 2004;10(12 Pt 2):4276s–4280s. doi: 10.1158/1078-0432.CCR-040010. [DOI] [PubMed] [Google Scholar]
- 3.Kaneda S, Nalbantoglu J, Takeishi K, Shimizu K, Gotoh O, Seno T, et al. Structural and functional analysis of the human thymidylate synthase gene. J Biol Chem. 1990;265:20277–20284. [PubMed] [Google Scholar]
- 4.Jakobsen A, Nielsen JN, Gyldenkerne N, Lindeberg J. Thymidylate synthase and methylenetetrahydrofolate reductase gene polymorphism in normal tissue as predictors of fluorouracil sensitivity. J Clin Oncol. 2005;23:1365–1369. doi: 10.1200/JCO.2005.06.219. [DOI] [PubMed] [Google Scholar]
- 5.Dervieux T, Furst D, Lein DO, Capps R, Smith K, Walsh M, et al. Polyglutamation of methotrexate with common polymorphisms in reduced folate carrier, aminoimidazole carboxamide ribonucleotide transformylase, and thymidylate synthase are associated with methotrexate effects in rheumatoid arthritis. Arthritis Rheum. 2004;50:2766–2774. doi: 10.1002/art.20460. [DOI] [PubMed] [Google Scholar]
- 6.Berkun Y, Levartovsky D, Rubinow A, Orbach H, Aamar S, Grenader T, et al. Methotrexate related adverse effects in patients with rheumatoid arthritis are associated with the A1298C polymorphism of the MTHFR gene. Ann Rheum Dis. 2004;63:1227–1231. doi: 10.1136/ard.2003.016337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schultz RM, Chen VJ, Bewley JR, Roberts EF, Shih C, Dempsey JA. Biological activity of the multitargeted antifolate, MTA (LY231514), in human cell lines with different resistance mechanisms to antifolate drugs. Semin Oncol. 1999;26(2 Suppl 6):68–73. [PubMed] [Google Scholar]
- 8.Sigmond J, Backus HH, Wouters D, Temmink OH, Jansen G, Peters GJ. Induction of resistance to the multitargeted antifolate Pemetrexed (ALIMTA) in WiDr human colon cancer cells is associated with thymidylate synthase overexpression. Biochem Pharmacol. 2003;66:431–438. doi: 10.1016/s0006-2952(03)00287-9. [DOI] [PubMed] [Google Scholar]
- 9.Smit EF, Burgers SA, Biesma B, Smit HJ, Eppinga P, Dingemans AM, et al. Randomized phase II and pharmacogenetic study of pemetrexed compared with pemetrexed plus carboplatin in pretreated patients with advanced non-small-cell lung cancer. J Clin Oncol. 2009;27:2038–2045. doi: 10.1200/JCO.2008.19.1650. [DOI] [PubMed] [Google Scholar]
- 10.Ulrich CM, Robien K, Sparks R. Pharmacogenetics and folate metabolism--a promising direction. Pharmacogenomics. 2002;3:299–313. doi: 10.1517/14622416.3.3.299. [DOI] [PubMed] [Google Scholar]
- 11.Travis WD, Colby TV, Corrin B, Shimosato Y, Brambilla E. Histological typing of lung and pleural tumours. 3rd ed. Berlin: Springer-Verlag; 1999. [Google Scholar]
- 12.Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000;92:205–216. doi: 10.1093/jnci/92.3.205. [DOI] [PubMed] [Google Scholar]
- 13.Boom R, Sol CJ, Salimans MM, Jansen CL, Wertheim-van Dillen PM, van der Noordaa J. Rapid and simple method for purification of nucleic acids. J Clin Microbiol. 1990;28:495–503. doi: 10.1128/jcm.28.3.495-503.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nief N, Le Morvan V, Robert J. Involvement of gene polymorphisms of thymidylate synthase in gene expression, protein activity and anticancer drug cytotoxicity using the NCI-60 panel. Eur J Cancer. 2007;43:955–962. doi: 10.1016/j.ejca.2006.12.012. [DOI] [PubMed] [Google Scholar]
- 15.Ceppi P, Volante M, Saviozzi S, Rapa I, Novello S, Cambieri A, et al. Squamous cell carcinoma of the lung compared with other histotypes shows higher messenger RNA and protein levels for thymidylate synthase. Cancer. 2006;107:1589–1596. doi: 10.1002/cncr.22208. [DOI] [PubMed] [Google Scholar]
- 16.Scagliotti GV, Parikh P, von Pawel J, Biesma B, Vansteenkiste J, Manegold C, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008;26:3543–3551. doi: 10.1200/JCO.2007.15.0375. [DOI] [PubMed] [Google Scholar]
- 17.Dulucq S, St-Onge G, Gagné V, Ansari M, Sinnett D, Labuda D, et al. DNA variants in the dihydrofolate reductase gene and outcome in childhood ALL. Blood. 2008;111:3692–3700. doi: 10.1182/blood-2007-09-110593. [DOI] [PubMed] [Google Scholar]
- 18.Wu MF, Hsiao YM, Huang CF, Huang YH, Yang WJ, Chan HW, et al. Genetic determinants of pemetrexed responsiveness and nonresponsiveness in non-small cell lung cancer cells. J Thorac Oncol. 2010;5:1143–1151. doi: 10.1097/JTO.0b013e3181e0b954. [DOI] [PubMed] [Google Scholar]
- 19.Uramoto H, Onitsuka T, Shimokawa H, Hanagiri T. TS, DHFR and GARFT expression in non-squamous cell carcinoma of NSCLC and malignant pleural mesothelioma patients treated with pemetrexed. Anticancer Res. 2010;30:4309–4315. [PubMed] [Google Scholar]
- 20.Graziano F, Kawakami K, Ruzzo A, Watanabe G, Santini D, Pizzagalli F, et al. Methylenetetrahydrofolate reductase 677C/T gene polymorphism, gastric cancer susceptibility and genomic DNA hypomethylation in an at-risk Italian population. Int J Cancer. 2006;118:628–632. doi: 10.1002/ijc.21397. [DOI] [PubMed] [Google Scholar]
- 21.Shannon B, Gnanasampanthan S, Beilby J, Iacopetta B. A polymorphism in the methylenetetrahydrofolate reductase gene predisposes to colorectal cancers with microsatellite instability. Gut. 2002;50:520–524. doi: 10.1136/gut.50.4.520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boccia S, Boffetta P, Brennan P, Ricciardi G, Gianfagna F, Matsuo K, et al. Meta-analyses of the methylenetetrahydrofolate reductase C677T and A1298C polymorphisms and risk of head and neck and lung cancer. Cancer Lett. 2009;273:55–61. doi: 10.1016/j.canlet.2008.07.026. [DOI] [PubMed] [Google Scholar]