

Abstract
Background:
Notalgia paresthetica (NP) is a very common, under-recognized condition characterized by pruritus in a unilateral, dermatomal distribution in the mid-back. Chronic pruritus is sometimes accompanied by pain, paresthesias, or altered sensation to touch.
Objectives:
To review the current literature with regards to the cause of NP and its most appropriate treatment.
Methods:
Comprehensive literature review using PubMed to inspect the available data on NP.
Results:
The most likely cause of NP is cutaneous nerve damage. Many therapies have been tried in the treatment of NP, mostly in small case studies.
Conclusions:
The published cases and studies suggest symptoms of NP are due to a cutaneous sensory neuropathy. Treatments addressing the condition as such are more successful than traditional itch therapies. In many cases, a simple explanation for the persistent pruritus is satisfactory for patients. For very distressing cases, therapy should address the condition as a benign sensory neuropathy. Further studies are needed to evaluate which treatments have the greatest potential for providing symptom relief.
Keywords: notalgia paresthetica, pruritus, cutaneous neuropathy, neuropathic itch, backscratcher
Case report
The 57-year-old woman pictured (Figure 1) has had episodic pruritus of the mid-back for six years. She denied any apparent cause for the pruritus. At times there was an accompanying sensation of “pins and needles.” She also complained of heightened sensitivity in the area, which she noticed when putting on clothes or rubbing her back against the bed. She located the affected area medial to the left scapula. She could not identify anything that improved or worsened the symptoms.
Figure 1.
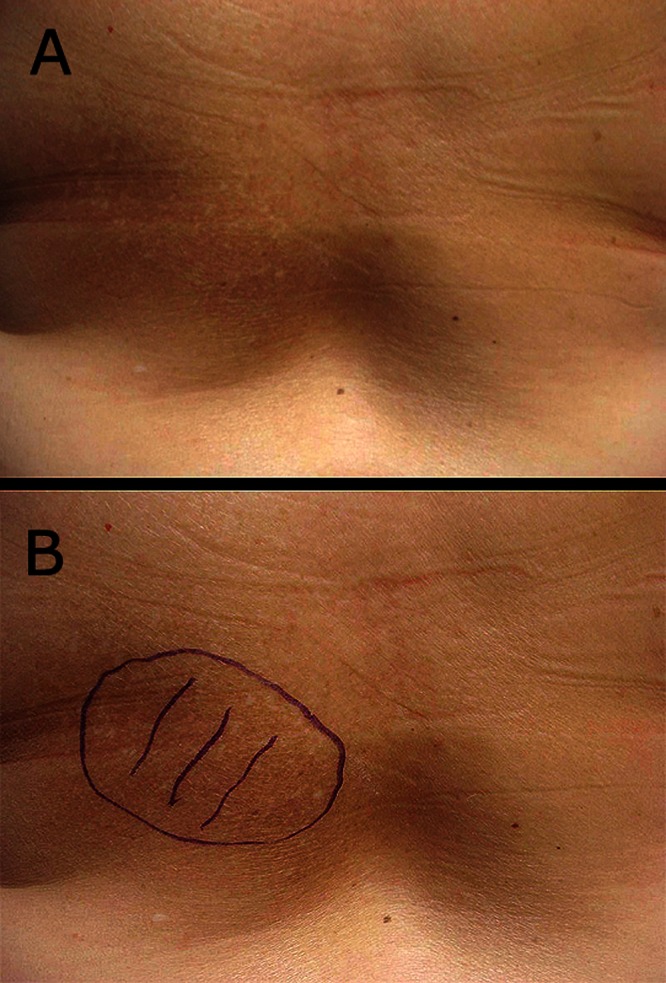
(A) The symptomatic area medial to the patient’s left scapula is visible as a hyperpigmented patch. (B) The hyperpigmented patch is highlighted on the patient’s mid-back. [Copyright: ©2013 Ellis.]
On examination, there was a hyperpigmented patch medial to the left scapula within the dermatomes of T2–T6. The patient had hyperesthesia to light touch in this area. There were no dermatitis, excoriations, or appreciable tissue texture changes, warmth, or edema.
Comment
For centuries people have complained about an itch, just between the shoulder blades, that is out of reach to scratch. For some, the itch can become so persistent, so maddening that finding a way to scratch is all consuming. The back-scratcher is such a primitive tool that even apes have been observed making them from tree branches. Elaborate back-scratchers have been fashioned from everything from whale-bone to tortoiseshell and have been designed by diverse cultures throughout time. We postulate that notalgia paresthetica (NP) was the stimulus leading to the invention of the backscratcher, perhaps by our primate ancestors. Another possible explanation could be that the backscratcher or similar instrument is not the treatment of NP but its cause. Itch can lead to scratching and rubbing either with an instrument or against a wall, which leads to post-inflammatory hyper-pigmentation and the findings that we call NP.
NP is a common dermatologic complaint characterized by unilateral pruritus medial or inferior to the scapula. The condition was first described in 1934 by Astwazaturow, though the complaint of a chronically itchy back has likely plagued people since the beginning of time. NP is typically confined to the dermatomes of T2–T6 and may have accompanying pain, paresthesia, numbness, or hyperesthesia. A patch of lichenification or post-inflammatory hyperpigmentation is the result of chronic scratching [1–3]. It may be more prevalent in middle-age women and often lasts for years [4].
The cause of NP is unclear. Several possible etiologies have been proposed, but it is generally believed that NP is a sensory neuropathy. A small study by Springall and colleagues suggested a proliferation of cutaneous nerves in NP lesions [5]. This finding was not confirmed in any of the 14 patients Savk et al biopsied; none of the tissue samples showed an increase in dermal innervation compared with controls [6]. Most evidence suggests NP is the result of damage to the cutaneous branches of the posterior divisions of the spinal nerves. This can occur either by impingement from degenerative changes in the spine or spasms in the paraspinal musculature. Pain, paresthesia, and numbness are more commonly thought of as neurological findings, but pruritus is an often-unrecognized symptom of nerve damage.
Muscle spasms or fibrous bands may compress cutaneous nerves and cause symptoms. Massey and Pleet used electromyography to detect paraspinal denervation at T2–T6, corresponding to symptoms of NP in 7 out of 9 patients. They suggest the sensory nerve branches at T2–T6 are susceptible to minor trauma because of how they pierce the multifidus spinae muscle [7]. The dorsal nerve roots exit the fascia of the multifidus spinae at a right angle en route to the epidermis; as a result they may be more exposed and prone to injury than in other areas of the back [7, 8].
These nerves can also be entrapped as they exit the spine through the vertebral foramen. A study by Savk and Savk of 43 patients with NP showed over 60% had radiographic findings of degenerative vertebral changes or herniated discs in areas that corresponded to the dermatomal distribution of their symptoms [4]. Several other studies have similarly shown an association between NP and significant spinal pathology [2,3,9].
The diagnosis is made clinically on the basis of history. Often, there are few if any signs of the disease; in some cases there may be localized hyperpigmentation or sensory findings in the infrascapular area. Spinal imaging is not necessary unless the patient has other neurological or musculoskeletal symptoms. Differential diagnosis should include tinea versicolor, contact dermatitis, parapsoriasis, neurodermatitis, and macular amyloidosis. Biopsy of NP may show signs of post-inflammatory hyperpigmentation, mild hyperkeratosis, and mild inflammatory infiltrate of the papillary dermis with dermal melanophages [2,3,6]. Some studies show no evidence of amyloid deposition in NP [2,6], while others do report sparse amyloid detected in dermal papillae [3,10]. This type of cutaneous amyloid is the result of damage to keratinocytes from chronic friction (scratching). It is therefore not surprising to see amyloid deposits in pruritic NP lesions that have been present for years. However, the presence of amyloid can make the distinction from macular amyloidosis difficult, as there is considerable overlap of these two entities [10].
Typical itch treatments such as antihistamines or topical steroids do not address the neuropathic itch of NP [3]. Other treatments that have been tried include topical capsaicin [11], cutaneous botulinum toxin type A injections [12], local nerve block [13], gabapentin [14], oxcarbazepine [15], and surgical decompression of the nerve [8]. These therapies have shown varied improvement of symptoms, may be expensive, invasive or require continued long-term use, and in some cases have undesirable side effects (Table 1).
TABLE 1.
Treatment options for notalgia paresthetica
| Treatments | Description | Efficacy |
|---|---|---|
| Capsaicin [11] | 0.025% cream to affected areas 5 × day for 1 week, then 3 × day for 5 weeks | 70% had improvement, but symptoms returned within a month of stopping treatment |
| Botulism toxin type A [12] | 4 units per superficial injection, spaced 2 cm apart throughout affected area | Resolution of symptoms for over 18 months observed in one patient |
| Nerve block [13] | 5 mL bupivacaine 0.75% with 40 mg methylprednisolone acetate | Resolution of symptoms for at least 12 months in one patient |
| Gabapentin [14] | Initial dose of 300 mg at bedtime, increased to 600 mg | Resolution in one patient while on medication. Symptoms returned fully when medication stopped |
| Oxcarbazepine [15] | Initial dose of 300 mg twice daily. Increased to 600 or 900 mg to achieve adequate relief | Improvement, no resolution, in four patients |
| Surgery [8] | Surgical decompression of cutaneous nerve | Resolution of symptoms observed in one patient |
| Transcutaneous Electrical Nerve Stimulation [9] | 5 20-minute sessions/week × 2 weeks, 50–100 Hz with a 40–75 μs pulse width | Improvement of symptoms, no resolution, in 15 patients |
| Exercise [16] | Strengthening of rhomboid and latissimus dorsi muscles, stretching of pectoral muscles daily for one week | Resolution of symptoms in two patients |
| Acupuncture [17] | Deep intramuscular stimulation to paraspinal muscles in affected area every 1–2 weeks until relief | Partial to complete resolution after 2–6 treatments, but relapse of symptoms in 1–12 months, observed in 16 patients |
| Osteopathic Manipulative Treatment [18] | Muscle energy, soft tissue, inhibition, fascia release | Improvement of symptoms observed in one patient |
Recent studies have looked at several non-pharmacological, non-surgical therapies to address the neuro-musculoskeletal pathology presumed to cause NP (Table 1).
Savk and Savk showed that transcutaneous electrical nerve stimulation yielded statistically significant improvement in the symptoms of 15 NP patients with corresponding radiographic findings. From an initial pruritus of 10/10, there was a decrease in pruritus to a mean 6.8/10 after ten sessions over two weeks [9].
A case study using exercises to strengthen postural muscles and extend the spine, thereby reducing the angle of the cutaneous nerves as they pass through the muscles and the transverse processes, completely eliminated pruritus in two women with NP [16].
Acupuncture also appears promising for relief of NP. A study of 16 patients with neurogenic pruritus, seven of which had presentations consistent with NP, illustrated complete relief of pruritus in 75% after 2–6 treatments with deep intramuscular stimulation acupuncture. Recurrence of symptoms did occur after 1–12 months without therapy in 37%, necessitating further treatment [17].
Osteopathic manipulative treatment (OMT) relieved pruritus in a middle-aged woman who developed NP following a motor vehicle accident. Soft tissue techniques applied to the affected upper thoracic and scapular regions improved the patient’s pain and itching [18]. This was only a single case study, but if proven effective it may be an easy way for osteopathic dermatologists comfortable with OMT to treat these patients.
All of these modalities warrant further investigation of their usefulness for the treatment of NP and other types of neurogenic pruritus. Patients often get some relief simply by learning the pruritus they are experiencing has a biological cause and a name. In persistent cases that interfere with quality of life, say if your patient owns multiple, strategically located back scratchers, some of these therapies may be worth trying. And while scratching to excess with a large salad fork is not recommended, for more mild symptoms, the timeless phrase, “I’ll scratch your back if you’ll scratch mine” is fitting. And the market for back scratchers is as strong as ever.
Conclusion
Take home messages about notalgia paresthetica:
NP is a unilateral pruritus located medial or inferior to the scapula in the T2–T6 dermatomal region.
NP is most often seen in middle-aged women and can last for months or years.
It may be accompanied by pain, paresthesias, numbness, or hypersensitivity.
Symptoms are most likely caused by impingement of nerves as they exit the spinal column or traverse through muscles of the back. It is sometimes seen in association with herniated discs or degenerative disc disease.
Traditional itch treatments (antihistamines, topical steroids) fail because they do not address the neuropathy.
Many modalities have been used to treat NP with varying success. The most important point to keep in mind is this is a harmless condition, which often does not warrant the potential side effects or risks of many treatments.
Educating patients about the cause and course of the condition can be the most important aspect of treatment.
Acknowledgments
The author would like to acknowledge the invaluable contributions of David Elpern, M.D. This paper was written during a dermatology clerkship in his office. His input and help with editing is greatly appreciated.
Footnotes
Funding: None.
Competing interests: The author has no conflicts of interest to report. No sources of funding were used to assist in the preparation of this review. This literature review is an original contribution.
References
- 1.Massey EW, Pleet AB. Localized pruritus–notalgia paresthetica. Arch Dermatol. 1979;115(8):982–3. [PubMed] [Google Scholar]
- 2.Savk E, Savk SO, Bolukbasi O, et al. Notalgia paresthetica: a study on pathogenesis. Int J Dermatol. 2000;39(10):754–9. doi: 10.1046/j.1365-4362.2000.00080.x. [DOI] [PubMed] [Google Scholar]
- 3.Raison-Peyron N, Meunier L, Acevedo M, Meynadier J. Notalgia paresthetica: clinical, physiopathological and therapeutic aspects. A study of 12 cases. J Eur Acad Dermatol Venereol. 1999;12(3):215–21. [PubMed] [Google Scholar]
- 4.Savk O, Savk E. Investigation of spinal pathology in notalgia paresthetica. J Am Acad Dermatol. 2005;52(6):1085–7. doi: 10.1016/j.jaad.2005.01.138. [DOI] [PubMed] [Google Scholar]
- 5.Springall DR, Karanth SS, Kirkham N, Darley CR, Polak JM. Symptoms of notalgia paresthetica may be explained by increased dermal innervation. J Invest Dermatol. 1991;97(3):555–61. doi: 10.1111/1523-1747.ep12481889. [DOI] [PubMed] [Google Scholar]
- 6.Savk E, Dikicioglu E, Culhaci N, Karaman G, Sendur N. Immunohistochemical findings in notalgia paresthetica. Dermatology. 2002;204(2):88–93. doi: 10.1159/000051823. [DOI] [PubMed] [Google Scholar]
- 7.Massey EW, Pleet AB. Electromyographic evaluation of notalgia paresthetica. Neurology. 1981;31(5):642. doi: 10.1212/wnl.31.5.642. [DOI] [PubMed] [Google Scholar]
- 8.Williams EH, Rosson GD, Elsamanoudi I, Dellon AL. Surgical decompression for notalgia paresthetica: a case report. Microsurgery. 2010;30(1):70–2. doi: 10.1002/micr.20702. [DOI] [PubMed] [Google Scholar]
- 9.Savk E, Savk O, Sendur F. Transcutaneous electric nerve stimulation offers partial relief in notalgia paresthetica patients with a relevant spinal pathology. J Dermatol. 2007;34(5):315–9. doi: 10.1111/j.1346-8138.2007.00279.x. [DOI] [PubMed] [Google Scholar]
- 10.Goulden V, Highet AS, Shamy HK. Notalgia paraesthetica—report of an association with macular amyloidosis. Clin Exp Dermatol. 1994;19(4):346–9. doi: 10.1111/j.1365-2230.1994.tb01212.x. [DOI] [PubMed] [Google Scholar]
- 11.Wallengren J, Klinker M. Successful treatment of notalgia paresthetica with topical capsaicin: vehicle-controlled, double-blind crossover study. J Am Acad Dermatol. 1995;32(2):287–9. doi: 10.1016/0190-9622(95)90152-3. [DOI] [PubMed] [Google Scholar]
- 12.Weinfeld PK. Successful treatment of notalgia paresthetica with botulinum toxin type A. Arch Dermatol. 2007;143(8):980–2. doi: 10.1001/archderm.143.8.980. [DOI] [PubMed] [Google Scholar]
- 13.Goulden V, Toomey PJ, Highet AS. Successful treatment of notalgia paresthetica with a paravertebral local anesthetic block. J Am Acad Dermatol. 1998;38(1):114–6. doi: 10.1016/s0190-9622(98)70552-3. [DOI] [PubMed] [Google Scholar]
- 14.Loosemore MP, Bordeaux JS, Bernhard JD. Gabapentin treatment for notalgia paresthetica, a common isolated peripheral sensory neuropathy [letter] J Eur Acad Dermatol Venereol. 2007;21(10):1440–1. doi: 10.1111/j.1468-3083.2007.02256.x. [DOI] [PubMed] [Google Scholar]
- 15.Savk E, Bolukbasi O, Akyol A, Karaman G. Open pilot study on oxcarbazepine for the treatment of notalgia paresthetica. J Am Acad Dermatol. 2001;45(4):630–2. doi: 10.1067/mjd.2001.116228. [DOI] [PubMed] [Google Scholar]
- 16.Fleischer AB, Meade TJ, Fleischer AB. Notalgia paresthetica: successful treatment with exercises. Acta Derm Venereol. 2011;91(1):356–7. doi: 10.2340/00015555-1039. [DOI] [PubMed] [Google Scholar]
- 17.Stellon A. Neurogenic pruritus: an unrecognized problem? A retrospective case series of treatment by acupuncture. Acupunct Med. 2002;20(4):186–190. doi: 10.1136/aim.20.4.186. [DOI] [PubMed] [Google Scholar]
- 18.Richardson BS, Way BV, Speece AJ. Osteopathic manipulative treatment in the management of notalgia paresthetica. J Am Osteopath Assoc. 2009;109(11):605–8. [PubMed] [Google Scholar]