

Abstract
Background:
Cutaneous horns usually develop on a keratinocytic base with the histopathology on a spectrum ranging from benign keratosis through to invasive squamous cell carcinoma (SCC). Some features of horns are easily identified using dermatoscopy.
Objective:
To investigate if specific clinical or dermatoscopy features of horns correlate with the histopathology in the base of the horn.
Methods:
Consecutive horn cases (n=163) were assessed prospectively in vivo for horn height, terrace morphology and base erythema using a Heine Delta 20 dermatoscope. Cases with potentially confounding influences were excluded. A history of horn pain or pain on palpation was also recorded.
Results:
Benign keratosis (n = 49), actinic keratosis (n = 21), SCC in situ (n = 37) and invasive SCC (n = 56) were recorded. An invasive SCC presenting as a horn as most likely to have a height less than the base diameter, 66% (37/56). Compared to the other study entities, invasive SCC tends to have less terrace morphology (P<0.05), a higher incidence of base erythema (P<0.05) and more pain (P<0.01).
Limitations:
Data categories did not include anatomic site or horn growth rates. Excision selection bias favored the incidence of invasive SCC.
Conclusions:
Horns presenting on an invasive SCC base are more likely to have a height less than the diameter of the base, not to have terrace morphology, to have an erythematous base and to be painful.
Keywords: squamous cell carcinoma, cutaneous horn, pain
Introduction
Cutaneous horns are usually found on chronic sun damaged skin. Horns are conical shaped, circumscribed and composed of dead keratin usually derived from base keratinocytes. Anatomic sites for horn predilection include the exposed areas on the head, the dorsa of the hands and forearms. A horn base may display benign or malignant histopathology. Horns with a benign histopathological base have a reported incidence ranging from 41% [1] to 60% [2, 3] and up to 77% on the eyelid [4]. Horn formation can occur in keratoacanthoma [5]. Squamous cell carcinoma has been reported in 94% of horns with a malignant base [1]. Factors previously reported to be associated with premalignant and malignant horns are male sex, increased age, anatomic site and lesion geometry [2]. Wide base or low height-to-base ratio horns are more likely to display a malignant base [2]. Multiple horns may occur on some patients. Actinic keratoses have been reported as the most common horn base entity (37.4%) in a study of 230 horns [6]. Horns associated with likely invasive SCC at the base should be identified and receive priority intervention. This study investigates four clinical and or dermoscopic features of horns to assess if these features indicate an increased chance that invasive SCC is present in the base of the horn. These features were: (a) the ratio of the height of the horn to the diameter of the base, (b) horizontal terrace morphology on the horn (suggesting compact orthohyperkeratosis), (c) presence of erythema at the base of the horn (suggesting increased blood perfusion) and (d) a history of previous horn pain and/or horn pain on palpation.
Methods
Prospective in vivo data collection occurred from July 2009 to April 2011 in a private practice in Sydney, Australia. All 163 cases were submitted for routine histopathology then allocated into one of the following four categories: benign keratosis; actinic keratosis; SCC in situ or invasive SCC. Horns with a seborrheic keratotic base were included in the benign keratosis category. Data was recorded in vivo using a Delta Heine 20 dermatoscope (Heine, Optotechnic GmbH, Herrsching, Germany). Photographs were recorded using a Canon EOS 550D camera (Canon, Tokyo, Japan) coupled to a DermLite FOTO dermatoscope (3Gen). To avoid diagnostic error due to inadequate tissue that is too superficial, all excisions were taken down to subcutaneous fat. In a previous horn study [6], some cases under investigation were unable to be confidently diagnosed due to insufficient excision depth.
Inclusion criteria
All consecutive horns that were excised within the study window were assessed for inclusion. All horns had to have a height greater than half the diameter of the base. All horns remaining after the application of the exclusion criteria were accepted into the study.
Exclusion criteria
Any horn with a known history of prior intervention was excluded, this included previous ablative therapies, topical medication either clinician or patient initiated, previous surgery and horns in a field of previous photodynamic therapy or radiotherapy. Horns in contact with tattoos or scars and collision situations where non-horn entities were identified together with a horn either during clinical examination, dermatoscopy or on histopathological section were also excluded. Horns on a non-keratinocytic base were not encountered during the study window.
Definitions of the horn features assessed
(1) Horn heights were compared to the diameter of the base of the horn. The height was recorded as either less than the base diameter or greater or equal to the base diameter, or up to a height twice the base diameter or greater than twice the base diameter. Such horn height assessment is very quick to perform and easy to do in practice.
(2) Terrace morphology is a feature characterized by structural horizontal contours on the side of the horn, as demonstrated by Figure 1A and B. An example of a horn without terrace morphology is shown in Figure 2A and Figure 2B.
Figure 1.

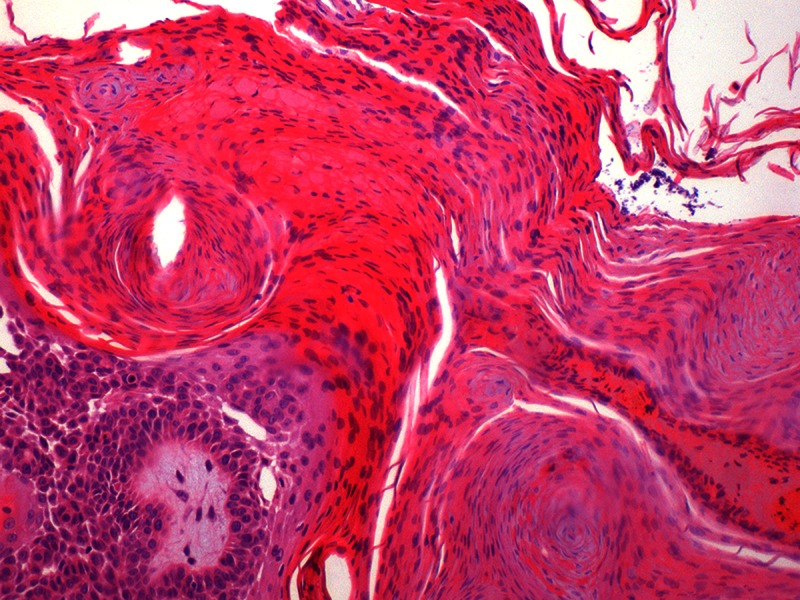
(A) Dermatoscopy demonstrating terrace morphology on a horn over benign keratosis. The horn height is greater than the base diameter, terrace morphology is present, no base erythema is present, and this horn was not painful. (B) Histopathology of the same horn as Figure 1A, hematoxylin and eosin stain. Orderly orthohyperkeratosis is present (arrow). [Copyright: ©2013 Pyne et al.]
Figure 2.

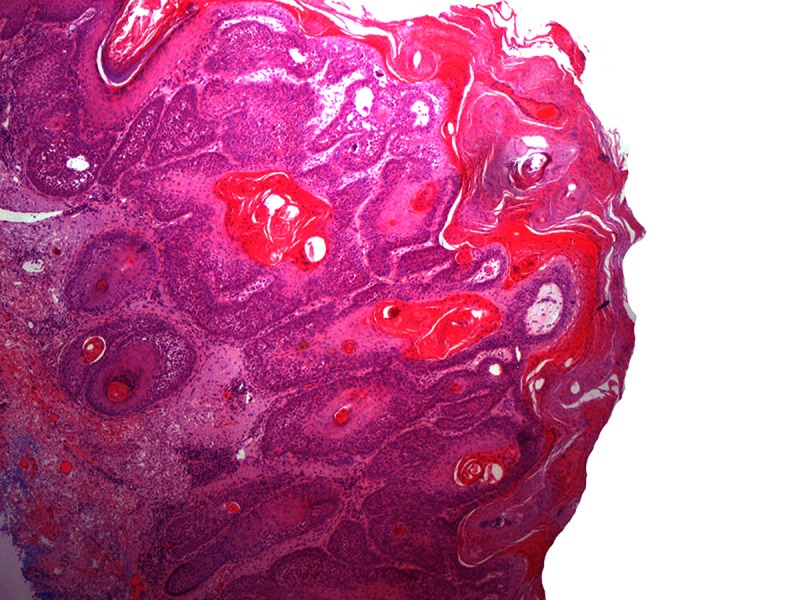
(A) Dermatoscopy of a horn with an invasive SCC base on the ear. The horn height is less than the base diameter, no terrace morphology is present, base erythema is present and this horn was painful. (B) Histopathology, same lesion as Figure 2A, hematoxylin and eosin stain. [Copyright: ©2013 Pyne et al.]
(3) Base erythema is present when the base of the horn displays red areas compared to the background skin assessed within 5 mm from the horn base boundary.
(4) Pain associated with the horn required careful interview technique to avoid prompting the patient to state the horn was painful when pain was not actually perceived. Pain was recorded as present if stated by the patient during history taking or reported on palpation during clinical examination.
Data categories
Following histopathological confirmation, all cases were allocated into one of the four diagnostic categories: benign keratosis, actinic keratosis, SCC in situ or invasive SCC. These four diagnostic categories were then collated with the previously in vivo recorded four features of: (a) ratio of horn height to base diameter, (b) the presence of terrace morphology, (c) the presence of red in the base and (d) a history of horn pain and or pain on palpation.
Data validation
To assess interobserver agreement between two observers (JP and DS), 20 consecutive horns were each assessed in vivo for the presence or absence of each of the four features under investigation. Each observer was blinded to the recording of the other observer. There was complete agreement with all four features of all 20 horns examined.
Formal Ethics Committee approval was granted by The University of Queensland prior to starting the study data collection.
Results
Invasive SCC 34.4% (56/163) was the most common histopathology at the horn base in this study with benign keratosis 30.1% (49/163) and SCC in situ 22.7% (37/163) less represented. Actinic keratosis occupied only 12.9% (21/163) of cases. Cases were dominated by Fitzpatrick 1 and 2 skin types with extensive sun damaged skin.
Relative horn height
Examination of Figure 3 finds 66% (37/56) of invasive SCC being represented by horn heights less than the base diameter. Invasive SCC has the highest incidence of all diagnostic entities in horns with a height less than the base diameter. Horns with a height between one and two times the base diameter show a progressive decline in incidence from benign keratosis 41% (20/41) to invasive SCC 27% (15/56). Compared to the other three diagnostic entities together, the horn height differences relative to invasive SCC are not significant (p = 0.31).
Figure 3.
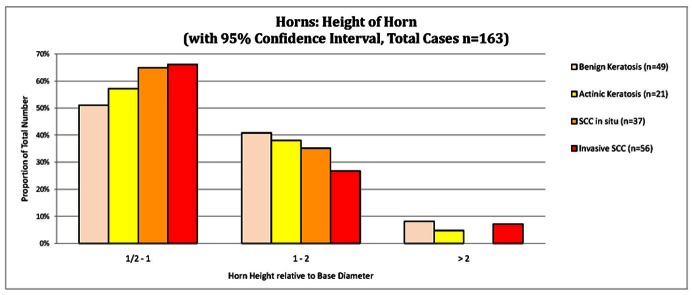
Height of the horn. The relative height of the horn compared to the base diameter. [Copyright: ©2013 Pyne et al.]
Terrace morphology
Terrace morphology was recorded in 38%, CI: 26.0—50.6% (21/56), of invasive SCC; see Figure 4. Invasive SCC had the lowest significant incidence of terrace morphology compared to the other entities combined, P = 0.02.
Figure 4.
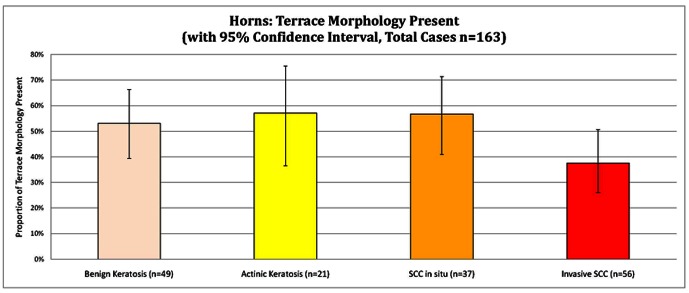
Presence of terrace morphology. [Copyright: ©2013 Pyne et al.]
Horn base erythema
Basal erythema occurred in over 55%, CI: 45.7—64.2%, of all four diagnostic categories, as shown in Figure 5. Invasive SCC displayed the greatest incidence of 77%, CI: 64.2—85.9% (43/56), erythema at the base, compared to the other entities combined P = 0.04.
Figure 5.
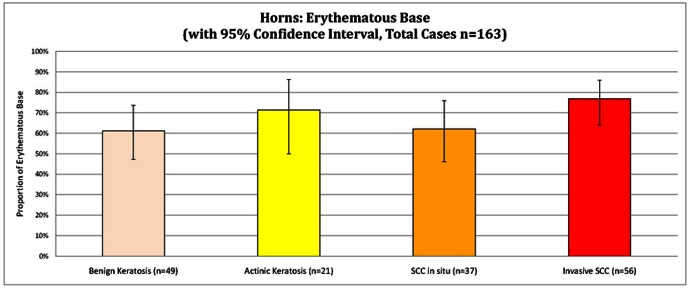
Presence of erythema in the horn base. [Copyright: ©2013 Pyne et al.]
Horn pain
A history of horn pain or pain on palpation was recorded in 48%, CI: 35.7—61.0%, (27/56) of invasive SCC; see Figure 6. Invasive SCC had the highest recorded incidence of pain compared to the other diagnostic categories, P = 0.007.
Figure 6.
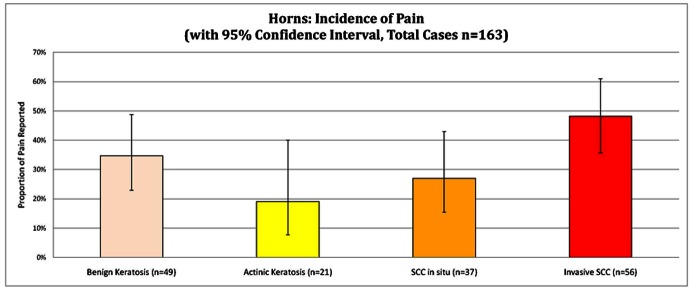
History of horn pain and or pain on palpation. [Copyright: ©2013 Pyne et al.]
Discussion
The overall incidence of the study of diagnostic entities does not reflect the presenting incidence of these entities in practice. Case selection was biased and based on actively seeking either in situ or invasive SCC. Although all the excised tissue in this study was submitted for histopathology, there may be some diagnostic under diagnosis due to sampling errors inherent in the histopathological processing. The intention of this study was to determine how significant the selected features were to confidently confirm or exclude invasive SCC in practice.
Terrace morphology is an orderly structural dermatoscopic feature with the histopathology of orthohyperkeratosis consisting of horizontal parallel lamellae of dead keratin. Examination of the data on Figure 4 shows that all entities, other than invasive SCC, have an incidence of terrace morphology of between 50 and 60% with overlapping confidence intervals. Given the more delinquent behavior and aggressive growth of invasive SCC, it was not surprising that invasive SCC had the lowest incidence of terrace morphology.
Erythema associated with the horn base was presumed to represent increased perfusion. It is unknown how much such erythema may be attributed to host generated inflammation or factors intrinsic to the neoplastic process in the horns concerned.
Study data in Figure 6 indicates that pain was most frequent in horns with invasive SCC. This has some practical value, as this symptom may prompt medical attention and should alert the clinician to consider invasive SCC as a likely diagnosis.
Horn base erythema, absent terrace morphology and the presence of horn pain were found to be statistically significant features in the discrimination of invasive SCC compared to the other study entities. However, due to the similar incidences of the features in the other entities, these features serve more as diagnostic indicators rather than for precise diagnostic confirmation.
Findings from this study indicate that when presenting as a horn, invasive SCC most likely has a height less than the diameter of the base; does not have terrace formation; displays base erythema; and may possibly be painful.
Whether present or absent, there was no feature in this study that alone confidently confirms or excludes the pre-histopathological diagnosis of invasive SCC at a horn base.
Acknowledgments
Dr. Devendra Sapkota is a Master of Medicine (Skin Cancer) degree student at The University of Queensland. His main role was to assist in data collection and data validation. Mr. Jian Cheng Wong is a Master of Statistics graduate from The University of New South Wales, Sydney. Mr. Wong was involved in the statistical planning, data processing and statistical analysis of this study.
Footnotes
Funding: None.
Competing interests: The authors have no conflicts of interest to disclose.
All authors have contributed significantly to this publication.
References
- 1.Mantese SA, Diogo PM, Rocha A, Berbert AL, Ferreira AK, Ferreira TC. Cutaneous horn: a retrospective histopathological study of 222 cases. An Bras Dermatol. 2010;85(2):157–63. doi: 10.1590/s0365-05962010000200005. [DOI] [PubMed] [Google Scholar]
- 2.Yu RC, Pryce DW, Macfarlane AW, Stewart TW. A histopathological study of 643 cutaneous horns. Br J Dermatol. 1991;124(5):449–52. doi: 10.1111/j.1365-2133.1991.tb00624.x. [DOI] [PubMed] [Google Scholar]
- 3.Copcu E, Sivrioglu N, Culhaci N. Cutaneous horns: are these lesions as innocent as they seem to be? World J Surg Oncol. 2004;3(2):18. doi: 10.1186/1477-7819-2-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mencia-Gutierrez, Gutierrez-Diaz E, Redondo-Marcos I, Ricoy JR, Garcia-Torre JP. Cutaneous horns of the eyelid: a clinicopathological study of 48 cases. J Cutan Pathol. 2004;31(8):539–43. doi: 10.1111/j.0303-6987.2004.00226.x. [DOI] [PubMed] [Google Scholar]
- 5.Yang JH, Kim DH, Lee JS, et al. A case of cutaneous horn originating from keratoacanthoma. Ann Dermatol. 2011;23(1):89–91. doi: 10.5021/ad.2011.23.1.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schosser RH, Hodge SJ, Gaba CR, Owen LG. Cutaneous horns: a histopathologic study. South Med J. 1979;72(9):1129–31. doi: 10.1097/00007611-197909000-00014. [DOI] [PubMed] [Google Scholar]