

Abstract
To detect vascular variability anomalies (VVAs), a blood pressure and heart rate profile around the clock for at least 7 days is a start. As a minimum, measurement every 60 or preferably 30 minutes for a week is needed, to be continued if abnormality is found, to assess the about 24-hour (circadian) variability that exists in all individuals. As a first dividend, one then also obtains a glimpse of 2 of the very many longer-than-circadian periodicities, the biological half-week and week. Certainly if we can have sensors and computer chips in our cars that continuously monitor the pressure over a tire's life, we should be able to do the same job for ourselves for diagnostic and therapeutic decisions. Healthcare today emphasizes wellness with recommendations for exercise and a proper diet, yet these evaluations may not be adequate. BP may be measured at a visit to the doctor or before an exercise session, along with measuring body weight and performing a physical exam. The seeds of disease are planted long before they are visible, and what appears to be normal from a conventional point of view may in fact be abnormal. Hidden alterations of physiological function, masked by the body's remarkable adaptive capabilities, may become visible through a new diagnostic and therapeutic realm—chronobiology—that reveals hitherto unseen abnormalities. The tools of chronobiology may yield additional dividends, such as the detection of physiological “loads” related to stress and stress relief and the undesirable effects of space weather upon personal events such as sudden cardiac death, societal events like terrorism and war, and natural disasters. Chronobiologically interpreted automatic ambulatory BP and heart rate (HR) monitoring (C-ABPM) may detect the antecedents of these types of events. C-ABPM is of interest in preventive cardiology, since it reveals new diagnoses as vascular variability anomalies (VVAs) and renders previous conventional diagnoses more reliable, such as that of an elevated BP. These VVAs include MESOR (midline-estimating statistic of rhythm)-hypertension, an elevation of the MESOR, which is diagnosed, like all other VVAs, only after 1 or preferably several replications of 7-day around-the-clock BP monitoring with available, affordable, and unobtrusive instrumentation. The recommendation for continuous C-ABPM recognizes several principles that constitute inseparably intertwined contributors to severe cardio-, cerebro- and renovascular diesase. C-ABPM gauges wear and tear of genetics, physical loads, and in particular mental stress placed upon individuals from “womb to tomb” by daily life, including weather in extraterrestrial space as well as that on earth, as a continuous surveillance paradigm preventing us from flying blind to a change from less than 5% to near 100% in the risk of a stroke within 6 years.
Key Words: Chronobiology, ambulatory blood pressure, hypertension, circadian, coherence, C-ABPM, stress, vascular variability anomaly, disorder, syndrome
摘要
对于血压等看似简单的问题,仅 仅衡量药物乃至饮食和运动的影 响是不够的:而需要至少 7 天昼 夜不停地仔细衡量,以准确描述 众多个体身上出现的 24 小时( 全天)变化。由此带来的首要好 处是,可以简要了解很多超过一 个昼夜时长的两个时段(即生物 半周和生物周)的情况。当然, 既然我们的汽车可以装传感器和 电脑芯片,在轮胎寿命期内对轮 胎压力进行持续监测,那么我们 自己应该也能采取相同的做法, 以作出诊断和治疗决定。如今的 医疗注重建议运动和合理饮食以 保持健康,但仅有这些要素或许 不够。可在就医时或在运动课程 之前测量血压,同时称体重并进 行体检。疾病在显现之前很久便 已埋下种子,而传统观点所认为 的正常情况实际上可能并不正 常。生理机能的隐性变化被身体 强大的适应能力掩盖,但可由新 的时间生物学诊断和治疗方法揭 示,从而展现可能隐藏的异常情 况。时间生物学工具还可能带来 其他好处,例如检测与压力和压 力释放有关的生理“负荷”,及 太空天气对个人事件(如心脏猝 死)、社会事件(如恐怖主义和 战争)以及自然灾害的不利影 响。从时间生物学角度解释的动 态血压 (BP) 和心率 (heart rate, HR) 监测 (C-ABPM) 可能会查出 这些事件的前因。C-ABPM 有助于 预防心脏病,因为其可显示血管 变异异常 (vascular variability anomalies, VVA) 等新诊断,并使 先前的传统诊断(如血压 (BP) 升高)更加可靠。VVA 包括高血 压 MESOR(midline-estimating statistic of rhythm,即调整中值), 即 MESOR 升高,如同其他所有 VVA 一样,其仅可通过使用价格 合理且普通可用的测量仪器进行 7 天昼夜不停的血压 (BP) 测, 得到一次或(最好是)几次证实 后作出诊断。关于持续 C-ABPM 的建议确认了几项要素,这些要 素紧密结合并互相作用,促成心 脏、大脑和肾血管疾病。包括日 常生活在个体的整个一生中对个 体基因、身体负荷和精神压力的 损耗,其中包括地球以外空间及 地球上的天气。
SINOPSIS
La mejor medición de los efectos de los fármacos e incluso de la dieta y del ejercicio físico en algo aparentemente tan simple como la presión arterial no es suficiente: necesita medirse prestando atención detenida al tiempo, durante las 24 horas al menos 7 días, para caracterizar de forma precisa la variabilidad durante 24 horas (circadiana), que existe en muchas personas. Como primer resultado, se vislumbran también dos de los muchos periodos largos circadianos, el biológico de media semana y el de una semana. Ciertamente, si nuestros coches pueden tener sensores y chips informáticos, que monitorizan continuamente la presión de los neumáticos, deberíamos ser capaces de conseguir lo mismo con respecto a las decisiones diagnósticas y terapéuticas. La atención médica actual enfatiza el bienestar con recomendaciones de practicar ejercicio físico y llevar una dieta apropiada, aunque estas valoraciones puede que no sean las adecuadas. La presión arterial puede medirse cuando se visita al médico o antes de una sesión de ejercicio, conjuntamente con el peso corporal y un examen físico. Las semillas de las enfermedades se plantan mucho antes del momento en que las enfermedades se hacen visibles y lo que parece normal desde un punto de vista convencional puede que sea, en realidad, anormal. Las alteraciones ocultas de la función fisiológica, enmascaradas por la notable capacidad adaptativa del cuerpo, pueden hacerse visibles mediante un nuevo entorno diagnóstico y terapéutico (de modo cronobiológico), lo que puede revelar anomalías que podrían estar ocultas. Los instrumentos de cronobiología podrían reportar beneficios adicionales, tales como la detección de “cargas” fisiológicas relacionadas con el estrés y la liberación de estrés, así como los efectos indeseables asociados al tiempo espacial en los acontecimientos personales, como la muerte súbita cardiaca, los acontecimientos sociales, como el terrorismo y la guerra, y los desastres naturales. El control (chronobiologically interpreted automatic ambulatory blood pressure monitoring, C-ABPM) automático y ambulatorio de la presión arterial (PA) y la frecuencia cardiaca (FC) interpretados de forma cronobiológica podría detectar los antecedentes de este tipo de acontecimientos. El C-ABPM es interesante en la cardiología preventiva, ya que revela nuevos diagnósticos, como las anomalías de la variabilidad vascular (vascular variability anomalies, VVA), y convierte los diagnósticos convencionales anteriores en más fiables, tales como los que muestran una PA elevada. Estas VVA incluyen la hipertensión de estimación de línea media estadística del ritmo (midline-estimating statistic of rhythm, MESOR), una elevación de MESOR, que se diagnostica, como el resto de las VVA, solamente después de una o preferiblemente varias réplicas del control constante de la PA las 24 horas del día durante 7 días mediante instrumentos que estén disponibles, sean asequibles y no causen molestias. La recomendación para un continuo C-ABPM reconoce varios principios, los cuales constituyen factores entrelazados e inseparables que contribuyen a las enfermedades graves cardiovasculares, cerebrovasculares y renovasculares. Estos incluyen el desgaste genético, las cargas físicas y el estrés mental, que soportan las personas continuamente en la vida diaria, incluido el tiempo en el espacio extraterrestre, así como en la tierra.
Chronobiologically interpreted automatic ambulatory blood pressure monitoring (C-ABPM) yields marker rhythms for vascular and/or other aspects of physiology, including mental functions and thus provides a quantifiable measure of stress, as a vascular variability anomaly (VVA). When a VVA persists in successive 7-day records, it becomes a vascular variability disorder (VVD) as an index of strain. When several VVDs persist and accumulate, they become a vascular variability syndrome (VVS). The risk of an adverse outcome within 6 years increased from less than 5% to nearly 100% in a study on 297 patients with hard outcomes by Kuniaki Otsuka. These adverse outcomes had a confirmatory follow-up on a much larger number of subjects with a proxy outcome of the left ventricular mass index (LVMI) and were further in keeping with a study followed up for over 4 decades. C-ABPM further reveals a new transdisciplinary spectrum with novel infradian (longer than 28-h) components that contribute to other personal and societal health risks, including sudden cardiac death, suicide, and homicide.
Those who regard the proposition of lifelong ABPM as utopian may reconsider when they realize that we can attach to our health, the same attention as we do for security on the road when we continuously measure tire pressure in our cars. This technological opportunity can be made available to our bodies as well as to our automobiles and laboratory animals used for research. Those interested in measurement and self-tracking have innumerable tools for measurement. By lifelong monitoring, we also gain new objective quantifiable perspectives of how seemingly unconnected events such as space weather affect us and arrive at new diagnoses in a personalized, societal, and environmental sense that in turn leads to a unified science based on “big data” (continuous time series, each covering years, eventually decades and even lifetimes). Beyond healthcare, we can start to think globally and act locally in space and can also be “glocal” in time, both with a view of the historical cycles that mold us and in the practice of automatically analyzing time series for continued surveillance.
Big data from C-ABPM serve us with repeated passes over time as they accumulate both as a whole at a given time (globally) and further in sections systematically varied in length (locally) with a view of the cycles that characterize them. This requirement of “glocality” in concept and as an analytical method can be demonstrated, among others, by the fruits of analyzed C-ABPM data, yielding a marker for the human mind as well as for the circulation. In so doing, it reveals our intimate associations with our cosmos. In the language of frequencies, the odds ratio for the number of periods shared by human mental function and geomagnetics more than matches that between the magnetisms of the interplanetary field and the earth.
SELF-SURVEILLANCE
Healthcare stakeholders are slowly beginning to realize that the current costly, disease-oriented health service provided to an individual after the onset of disease can be complemented by programs for “wellness” with self help–based care utilizing ongoing surveillance and early actions whenever warranted. A cost-effective C-ABPM system (around the clock at 30-min intervals for all ages) is immediately available, worldwide, on a small scale. It is provided with free analyses for all from a project on The BIOsphere and the COSmos, BIOCOS. This project constitutes a validation test for an international website (www.2011.geocataclysm.org) recommended by a World Forum on “Natural Cataclysms and Global Problems of the Modern Civilization,” held September 19-21, 2011, in Istanbul, Turkey, that extended the scope of prior consensus conferences. Thus, responses to Sir William Osler's “wear and tear,” putative harbingers of severe disease,1–4 are detected as gauges of loads,4–8 prompting preventive action. Eventually, this task can be implemented on a large scale by an international multilingual analytical and educative website (Figure 1)1,4 on a larger than the currently ongoing small-scale endeavor. The emphasis on wellness can be augmented when prevention is desired. We need no longer fly blind, ignorant to the circadian and the many other variabilities within us and around us, as soon as we have in this generation a system instituted where such a service can be offered freely, such as in community libraries or pharmacies. In the next generation, everyone can be trained in self-monitoring in earliest schooling.9 Today, we have a Zeo Sleep Coach that monitors the brain's electrical waves, the Fitbit that tracks the number of steps you take each day (you need 10 000 steps a day), body scales that measure your weight and body-fat readings and send them to your computer, blood pressure (BP) monitor jacks into your smart phones, and motion sensors that allow you to track how often you brush your teeth or how many times a day you use the bathroom or open the refrigerator door. C-ABPM is no longer out of the ordinary.
Figure 1.

Preventive and curative healthcare can yield the dividend of biomecial monitoring of space weather by time-structural analyses of ambulatory blood pressure and heart rate series.* Physiological, other biological, notably epidemiological, and sociological as well as physical and environmental data collection and analyses in the project on The BIOsphere and the COSmos, BIOCOS, are ongoing worldwide on a very small scale, yielding the data of this paper and some of those cited from our team. They constitute a validation test underlying a proposal by a World Forum on “Natural Cataclysms and Global Problems of the Modern Civilization,” held September 19-21, 2011, in Istanbul, Turkey (www.2011.geocataclysm.org), for a manned international multilingual website, providing analyses for all comers, and saving the data, beyond both the medical community (bottom right) and physical environmental science concerned about space weather effects (upper right), also for the self-surveilling public at large, notably for those interested in science and art, a unified transdisciplinary chronousphere. The Phoenix Project of volunteering members of the Twin Cities chapter of the Institute of Electrical and Electronics Engineers (http://www.phoenix.tcieee.org) is planning to develop an inexpensive, cuffless automatic monitor of blood pressure and to implement the concept of a website for a service providing automatic analyses in exchange for the data that in turn are to be used for refining methods for monitoring psychophysiological effects of space weather.
What Can Be Done Today
In a forthcoming book for the lay public advising patients found to have a BP that is too high or too low, a colleague asked the authors whether he could reproduce Figure 2, published in 198410 as an example of interindividual differences among 24-hour profiles. At the time of the original publication, we had not yet formulated VVAs or VVDs (Figure 3, pp 70-71) that are not generally known, a long series of consensus meetings notwithstanding1–4 and of course had no reference values for them. Mostly not implemented as yet is the detection of circadian and approximately 7-day (circa-septan) BP periodicities documented over a century ago that is immediately available for diagnostic and therapeutic use in 2012. As to diagnosis, let us start by asking this question: Who in Figure 2 is at the greater risk of a cerebral stroke or other severe cardiovascular disease? The important answer, contrary to current worldwide practice, is this: We can't tell; the record is too short. We need a 7-day record as a start and must continue to monitor if it shows abnormality (Figure 4, p 71).
Figure 2.

Different circadian patterns of systolic blood pressure (SBP) in 2 clinically healthy men. Twenty-four–hour profiles of blood pressure (BP) variation in 2 clinically healthy men were described in 198410 as revealing interindividual differences. In the interim, reference values from clinically healthy subjects with outcomes have demonstrated that a double amplitude of 60 mmHg in CH, 60 years of age, is compatible with a diagnosis of 24-hour CHAT (circadian hyper-amplitude-tension, a circadian overswing; see Figure 3) found on occasion in certain individuals as a physiological event (response) under routine conditions. If CHAT persists (is not smoothed out) in the 24-hour cosine fit to a 7-day around-the-clock record, the diagnosis of “7-day CHAT,” like that of “1-day CHAT,” is no more than an indication for further chronobiologically interpreted automatic ambulatory blood pressure (BP) and heart rate (HR) monitoring (C-ABPM). Two patients whose BP averages (here the MESORs, midline-estimating statistics of rhythm) are practically identical differ in terms of their psychophysiology, here gauged by the circadian amplitude of BP. Longer monitoring is indicated to arrive at an assessment of stress or load by a vascular variability anomaly (VVA), or a gauge of strain, a vascular variability disorder (VVD), and thus to assess the risk of developing, among other severe diseases, a stroke within 6 years. As compared to the risk associated with high BP, a risk of systolic CHAT doubled that risk.
Figure 3.

- MESOR (M)-hypertension (MH), an elevation of the M above RL, can be S-MH, D-MH, MA-MH or a combination thereof, demonstrated by M, from curve-fitting complemented by stacking along the 24-hour scale by a measure of load, the hyperbaric index and by percentages and times of abnormal values.4
- Circadian hyper-amplitude (A)-tension (CHAT), an elevation of the 24-hour A above RL, which can also be systolic (S-CHAT), diastolic (D-CHAT), mean arterial (MA-CHAT), or a combination of the foregoing. D-CHAT represents a 720% increase in risk of ischemic stroke.
- SBP-, DBP- or MAP-ecphasia (when persisting and associated with illness, circadian dysphasia), an odd timing outside RL of the circadian rhythm of BP but often not of that in HR.
- Circadian ecfrequentia (when persisting and associated with illness, circadian dysfrequentia), 1 or several circadian periods, τ, with a CI not overlapping RL.
- Excessive pulse pressure (EPP) when the difference in the MESORs of SBP and DBP for adults exceeds 60 mmHg.
- A deficient HR variability (DHRV), defined as a standard deviation of HR <7.5 beats/minute.
Threshold values remain to be replaced by RL. All RLs remain to be improved by restriction to those of disease-free long-lived peers specified by gender, age, ethnicity, and geography.
Figure 4.

Infradian systolic blood pressure (SBP) variability associated with psychophysiologic responses.* At the start of monitoring, CHF, a woman in presumably good health, was 60 years of age. She monitored her blood pressure (BP) and heart rate (HR) around the clock with a TM-2421 monitor from A&D (Tokyo, Japan). The reliability of the TM-2421 monitor had been documented. This monitor measures BP and HR according to the oscillometric and the auscultatory method. As a rule, with the instrument used, oscillometric readings are more reliable than auscultatory measurements. The monitor gives a beep as a warning to stand still (eg, if the user is walking or engaged in some other activity) or remain seated or recumbent, as the case may be. After the beep, the cuff inflates automatically, taking and storing a measurement of systolic and diastolic BP and HR. If so set at half-hourly intervals, automatic measurements are taken and stored for up to 2.5 weeks if the instrument is recharged at 3-day intervals, by being plugged into an electrical outlet for several minutes.
Monitoring sessions were repeated at intervals of weeks or months during 6 years. CHF kept a thorough diary at the time of monitoring, which allowed the association of spans when her BP was found to be deviant with the presence of strong emotions such as grief, conflict, and concern, albeit not in association with annoyance by particular measurements. Irrespective of the duration of a given monitoring session, analyses were carried out in repeated scans of the same data for separate subspans of (1) at least 24 h, (2) a week, (3) longer spans, sections of the data such as (4) only nightly readings or (5) readings without those accompanied by a note indicating annoyance by measurement; (6) in particular, interest such as concern for several weeks about a diagnosis of ovarian cancer in her daughter (showing gross abnormality) and (7) including analyses on all her data accumulated at certain times during the 6 years.
Each data series was analyzed using a curve-fitting and a stacking approach, with analyses of the long series confirming that CHF was 24-h synchronized; the CI (95% confidence interval) of her period, τ, overlapped 24 h. A model was fitted by least squares, which consisted of cosine curves with periods of 24 and 12 h. This model for most people accurately approximates the circadian waveform in BP and HR. The parameters are the MESOR, M, a rhythm-adjusted mean; the amplitude, A (of each of the 2 components), which is a measure of half the predictable extent of change within a cycle; and the acrophase, φ (also of each of the 2 components), a measure of the timing of overall high values recurring in each cycle, were computed. The circadian amplitude and acrophase, together with the MESOR, are interpreted in the light of reference values obtained from databases on clinically healthy subjects matched by gender and age. These reference intervals are calculated as 90% prediction limits. When the MESOR exceeds the upper 95% prediction limit, MESOR-hypertension is diagnosed; when the circadian amplitude exceeds the upper 95% prediction limit, the condition of CHAT is diagnosed; and when the φ or period lies outside the 90% prediction interval, ecphasia or ecfrequentia, respectively, is diagnosed, as apparent from Figure 3.
In the stacking approach, the data as a whole, averaged over an idealized 24-h cycle, are compared by computer with the time-specified reference limits (derived from databases obtained independently on clinically healthy subjects). These reference standards are again calculated as 90% prediction limits over 1-h intervals that are displaced by half an hour throughout the 24-h day. The reference values are thus specified as a function of clock-hour, gender and age (for 24-h synchronized subjects only, not for JF in Figure 28D during episodes of depression). CHF's data are compared with the upper limit of standards, called chronodesms. Whenever the subject's data exceed the upper limit of the chronodesm, BP deviation is diagnosed. The amount of time when the data are above the reference limit represents the percent time elevation. The area delineated between the subject's curve when the data are excessive and the upper limit of acceptability delineates the hyperbaric index in the case of BP and the tachycardic index in the case of HR. As an area under the curve, this index has the units of mmHg × h during 24 h for BP and of beats/min × h during 24 h for the case of HR.
The center of gravity of the area of excess is also calculated to represent the time of overall excess, which usually is informative for specifying the timing of treatment administration when it is needed. Cosine fit- and stacking-derived indices were computed for each profile as a whole as well as for spans of about 24 hours so as to determine the extent of day-to-day variability in the circadian variation and any deviation in relation to chronobiologic norms. The limitation of a profile of 24 hours is seen as intermittent black excesses above the upper limit of the chronodesm in daily summaries in the first record yet missing (with one initial exception) in the second record, each record covering weeks.
MESOR-hypertension was then detected for the first 5 days but not for the next 16 days in February (top left). The circadian amplitude was acceptable for the first 3 days in February but was intermittently excessive in February (top middle) but not in April (bottom middle). The circadian acrophase was deviant only at the beginning of the record in February (top right) and is invariably acceptable in April (bottom right). These results suggest the desirability to monitor for much longer than 24 hours to obtain a reliable diagnosis. Abnormality can occur while most or all measurements lie within acceptable limits insofar as they are neither too high nor too low on the average.
In looking at Figure 2 in 2012, some readers who rely on current official guidelines11 may infer that CH, the 60-year-old man, had a larger swing in BP and may be the healthier of the 2. Many more may recognize CH, the subject whose data are shown on the left of Figure 2, as an excessive “dipper,” a very common diagnosis based on a single 24-hour profile associated with undesirable outcomes, on a population basis.12–15 This majority in turn should not only question a record length of 24 hours as a basis of a diagnosis (Figure 2)5,16–18 but can compare the utility of a classification of dipping with the chronobio-logic diagnosis: eg, of a circadian overswing, CHAT (short for circadian hyper-amplitude-tension; Figure 3)4,19 associated with a high risk of stroke (Figures 5A–5C, pp 72-73).4 It must be realized that a diagnosis based on the single measurement of BP (Figures 6A–6C, pp 74-75), like that relying on a single 24-hour record, as in the case of Figure 2 and others, is a spotcheck rather than a platinum standard (Figure 7, p 75).2
Figure 5A.

An excessive circadian amplitude of diastolic blood pressure raises the risk of ischemic stroke by 720% (see last column on right). Original data of Kuniaki Otsuka.
Figure 5C.

An excessive circadian blood pressure (BP) amplitude (A)* is a risk factor for ischemic stroke and nephropathy independent from the 24-hour mean (MESOR)** Note high relative risk at lowest average blood pressure. Original data of Kuniaki Otsuka.
Figure 6A.

Hypertension and normotension at same clock-hour or even in 24-hour average on same day of week.* Need for systematic long-term surveillance by C-ABPM for subject JCM, a clinically healthy neurosurgery resident who had a systolic value of 160 mmHg on each of 2 occasions while giving blood.
Figure 6C.

Flipping a coin: Of 230 ambulatory blood pressures (BP) measured automatically during 23 days, about half are acceptable (56%) and half unacceptable (44%).*
Figure 7.

There is an alternative to flipping a coin and finding 0% or 100% acceptable values, namely a systematic chronobiologic blood pressure self-surveillance, notably in “borderline” hypertension. The current gold standard must go, just like the single blood pressure at the provider's office.
Figure 5B.

Excessive circadian amplitude of diastolic blood pressure raises the risk of nephropathy by 590% (see last column on right). Original data of Kuniaki Otsuka.
Figure 6B.

A single 24-hour blood pressure profile: fool's gold, not gold standard.* Sometimes, as in JCM, 23 days of monitoring are not enough for a diagnosis.
Urgency and Feasibility of Lifelong Monitoring, Starting at the Diagnosis of Blood Pressure Abnormalitya
In 1904, Theodore C. Janeway of Johns Hopkins University,20 then the opinion leader, did not wish to see a patient before collecting sufficient data to assess periodicities. (The plural was justified since by 1880 and 1881, Ignaz Zadek in Berlin had collected sufficiently long time series to document 24-h, 84-h, and 168-h rhythms [Figure 8, p 76].)21,22 In 1974, Frederic C. Bartter, of Bartter syndrome fame, then head of the Hypertension-Endocrine Branch at the US National Institutes of Health (NIH) and later the director of the Clinical Center at the NIH,b recognized that the reason his patient was diagnosed differently by 2 physicians who saw him at different times of day stemmed from circadian changes in BP (Figure 9A, p 76). His foresight was later illustrated in the abstract (Figure 9B, p 77), with additional evidence accumulating since the availability of automatic BP monitoring (Figure 9C, p 77).
Figure 8.

Results from 4 subjects φ in degrees 360° equated to period length (168, 84, or 24 hours). By 1880-1881, Ignaz Zadek had enough data on 4 patients to allow the demonstration by cosinor of daily, half-weekly, and weekly rhythms, seen with cosinor diagrams by error ellipses around the tip of vectors that do not overlap the center of the graph (pole) with the length of the directed line indicating the amplitude and its direction the acrophase.24
Figure 9A.

Blood pressure (BP) of Frederic C. Bartter's patient, a 61-year-old man, who had been diagnosed as normotensive by 1 physician seen in the morning and as hypertensive by another provider seen in the afternoon. BP measurements were taken 6 times each day for 17 days at NIH. Reprinted with permission from Bartter FC.23
Figure 9B.

Limitation of fixed limits for a circadian rhythmic function: fixed (horizontal) limits must go. We are reminded of outmoded laws and guidelines, still on the books in many states, intended to protect horses and mules at a time when automobiles (read chronobiologic monitors) were regarded as noisy toys, imposing obligations on motorists, such as “In the event that a horse refuses to pass a car on the road, the owner must take his car apart and conceal the parts in the bushes.”
Figure 9C.

Odd-time diastolic blood pressure (DBP) excess (dark section of diagram) for DJ (78-year-old man) taking “daily” 10 mg Vasotec (ACE inhibitor). Daytime office or dense waking self-measurements would have missed very high blood pressures by night. Reliance on office or self-measurements only during waking must go.
Frederic C. Bartter reached the following conclusion after having his patient studied in the clinical center23,24:
By conventional standards, this patient is clearly normotensive every morning. Yet the BP determined each day at 6 in the afternoon provides especially convincing evidence that this patient is a hypertensive…. My plea today, first made in 1974, is that information contained in such curves[cosinor fits; see Figures 2 and 3: our addition] become a routine minimal amount of information accepted for the description of a patient's blood pressure. The analysis of this information by cosinor should become a routine. It is essential that enough information be collected to allow objective characterization of a periodic phenomenon, to wit, an estimate of M [the time structure or chronome-adjusted mean, or MESOR] … an estimate of [the amplitude] A itself, and finally an estimate of acrophase,φ[a measure of timing, Figure 10A, p 78: our addition24]. In this way, a patient can be compared with himself at another time[Figure 10B, p 79: our addition25], or under another treatment, and the patient can be compared with a normal [Figure 2: our addition] or with another patient.23
Figure 10A.

Circadian ecphasia of cardiovascular variables in diabetic pregnancy. BP and HR monitoring of an 18-year-old, gravida 1, para 0, with type I brittle diabetes treated by an insulin pump during the 23rd week of pregnancy reveals not only a low BP and a high HR MESOR, but also ecphasia (actually a delayed acrophase, ie, epiphasia) by reference to peer group limits (68% prediction intervals). Results from Maggioni C, Halberg F, Cornélissen G, Work BA. Nocturnal heart rate and blood pressure peaking quantified as circadian ecphasia in a diabetic pregnancy. Chronobiologia. 1987;14:201.
*0° = local midnight; 360° = 24 hours (N = 131; P < .001 in each case).
Abbreviations: BP, blood pressure; DBP, diastolic blood pressure; HR, heart rate; MESOR, midline-estimating statistic of rhythm; SBP, systolic blood pressure.
Figure 10B.

Excessive circadian blood pressure amplitude is a more sensitive warning ( ) than a conventional stress test. Presence of circadian hyper-amplitude-tension (CHAT) found in 2 consecutive short records from a 35-year-old man precededing by a few months the occurrence of a heart attack while a stress test, carried out following the abnormal alarming BP monitoring results, found no abnormality. Even if warning was justified, sampling must not be restricted to actual spans of monitoring as short as those in BR.
) than a conventional stress test. Presence of circadian hyper-amplitude-tension (CHAT) found in 2 consecutive short records from a 35-year-old man precededing by a few months the occurrence of a heart attack while a stress test, carried out following the abnormal alarming BP monitoring results, found no abnormality. Even if warning was justified, sampling must not be restricted to actual spans of monitoring as short as those in BR.
What to do With 24-hour CHAT or With Other Records Covering a Single Cycle
Turning back to Figure 2, by using “clinically” healthy in its title rather than just “healthy” in 1984, we implied that we had no outcome data on the subjects investigated but were not aware of any abnormality. We still lack outcomes for CH, but have (we emphasize tentative) gender- and age-specified reference standards (RS) for whites, among others.26 We can make a diagnosis of 24-hour CHAT27 specifically in the light of now-available acceptability limits for the 24-hour amplitude, still to be improved by restriction to long-lived disease-free individuals. Having diagnosed 24-hour CHAT, we must realize the limitations of the record's brevity.5,16–18 Taking a 24-hour profile to assess a single circadian cycle being equivalent to taking the pulse for 1 second to gauge just a single cardiac cycle was recognized long ago.27,a The analogy of taking the pulse for only 1 second as assessing only a single cycle can now be extended to the physiological counterparts of a half-year and of the seasons and to periods shorter than 6 months, the cis-half-year (on this side of the period = cis) or longer than 12 months, the transyear (beyond = trans). Like the 11-year (undecennian) or decadal period of the sunspots, they are all reflected in the human circulation (Figures 11A–11C, pp 80-82).28–30 Whether it is normal or abnormal, neither a 24-hour nor a single 10- or 11-year record can eventually remain the basis of a diagnostic, therapeutic, or etiologic decision. In any case, the need remains for further lifelong C-ABPM and for continued epidemiological data collection and analysis, the purpose of the website. When the 24-hour record happens to be abnormal, it constitutes no more than an indication of the urgency of C-ABPM to assess a possibly acceptable physiological response. Reliance on data covering less than a solar cycle length has led to controversy31,32 and has retarded recognition of heliobiology in the West (Figures 12A–12D, pp 83-85).32,33
Figure 11A.

Different decadal and/or multidecadal periods in different variables of the same elderly man (FH) treated with hypotensive drugs. Periods,* τ, characterizing average (MESOR; blue) and circadian double amplitude (2A; red) of systolic (S; top) and diastolic (D; middle) blood pressure (BP) and heart rate (HR; bottom) of FH.**
Figure 11C.

Different decadal and/or multidecadal periods in different variables of WRB, a man treated for high blood pressure. Periods characterizing average (MESOR) and 7-day cycle double amplitude during 35 years of self-measured systolic (S, upper left) and diastolic (D, lower left) blood pressure (BP), and heart rate (HR, upper right) and body weight (BW, lower right) of WRB, a man 52 years old at start; increment and interval analyzed: 14 days.
Figure 12A.

Geographic as well as temporal differences in the association of the incidence pattern of myocardial infarction and magnetism in the United States, Israel, and Russia (where the original studies were done). An excess of death at peak solar activity can be demonstrated in sufficiently (29-year) long series. Time-varying associations revealed by also changing phase synchronizations and coherences readily account for site- and time-specific results. Controversy can be avoided when aeolian time- and site-specific changes are anticipated and documented in time series covering the length of several critical cycles characterizing the data.
The limitation of a blood pressure measurement over a single circadian cycle comes to mind: such a spotcheck may lead to a lifetime of unneeded treatment (when, in several repeated sessions, the patient was excited and the spotchecks showed “hypertension,” not the “white-coat effect,” which in a group examined was hypertension in the morning and hypotension in the evening. A hypertensive patient may be caught on several measurements with occasional normotensive values and hence will not be treated until a stroke or other severe event occurs. Furthermore, an individual with blood pressure overswinging limited to the normal range may not be recognized as being at a very high risk of stroke by limitation of a record to a single cycle. Likewise, studies that cover a single solar cycle may not be conclusive and may miss a relation that can be documented in the same solar cycle elsewhere or over 3 solar cycles (in Minnesota, United States). Taking evidence over a single solar cycle, just like relying on a single circadian cycle, is equivalent to taking the pulse for 1 second.
Association of magnetic storms and mortality from myocardial infarction (MI) not detected in the United States (1962-1966 daily data and only monthly to 1971) but detected in Russia (including morbidity) in 1979-1981 (top) and earlier. Bottom: association also detected in 1962-1968 in Russia and in 1974-1976 in Israel, at minima of Schwabe (∼10.5-y) and Hale (∼21-y) cycles, unless data in the late 1960s in Russia contribute the outcome at the preceding minimum. Minnesotan data over several solar cycles (1968-1996) document excess of 220 MI/year during solar maxima vs solar minima (black horizontal arrow along abscissa).
Figure 12D.

During years of maximal solar activity, there is an about 5% excess mortality (220 cases per year) from myocardial infarction in Minnesota (1968-1996) as compared to years of minimal solar activity. Twenty-nine years of data allow detection of differing mortality from myocardial infarction associated with solar cycle stages. Further analyses in Figures 32B–32D.
A record of the beating heart for a minute or 2 may be compatible with diagnosing death vs life, but it is hardly recommended when a full 24-hour record can fail to reveal abnormality that is present during each of 11 subsequent days and of course vice versa.
Figure 11B.

Different decadal and/or multidecadal periods in different variables of YW, a man untreated for his developing MESOR-hypertension. Periods, τ, characterizing average (MESOR) and double circadian amplitude (2A) of systolic (SBP) and diastolic (DBP) blood pressure and heart rate of YW.*
A 1-Week CHAT
A diagnosis of 24-hour CHAT, of an excessive circadian swing, can be physiologically associated in certain individuals, with events such as the arrival of welcome visitors (Figure 13, p 85)5 or any other pleasant tasks (not necessarily loads) such as giving a party5 or discussing important-seeming topics with a friend or even with a dear family member or without any obvious reason but perhaps one hidden in space weather.34,35 When a 24-hour cosine curve is fitted to a 7-day series as a whole (rather than to a 24-hour profile, as in Figure 2), a few days of CHAT may be smoothed out and the record as a whole may be acceptable (Figure 14A, p 86) or at least the number of weeks with CHAT is reduced (Figure 14B, p 87).36 On a population basis, the high risk of severe events associated with CHAT (Figures 5A–5C) and more so with coexisting VVDs is clearly demonstrated (Figures 15A and 15B, pp 88-90).4 A VVA for a single day should invariably prompt, as a follow-up, at least an added 7-day C-ABPM. In a case of fulminating CHAT (Figure 10B, p 79),25 this recommendation was not fully implemented, albeit a second short record was even more abnormal than the first. The patient took a conventional stress test instead, which was normal, and hence nothing else was done. Some months later, he returned asking for an implanted BP sensor. We asked why, and he told us that in the interim he had had a myocardial infarction.25 C-ABPM was also ignored in a single case of CHAT during pregnancy (but not in other cases with this diagnosis in the same investigation). In that case, the systolic BP average (MESOR) was 115 mmHg (Figure 16, p 91)4 and the cost of ignoring variability approximated $1 million US for the case of a very premature baby.
Figure 13.

Original data underlie an association of circadian hyper-amplitude-tension (CHAT; fit not shown) with visitors who were friendly, one a prospective collaborator, the other an earlier provider of important data for analysis. FH, an elderly man, was unaware of the fact that the arrival on March 7 of one and of the other on March 10 was preceded by spikes in BP by hours or a day, respectively. All results were within the acceptable range, yet the swing within that range was excessive. CHAT was present while the visitors were around.
Figure 14A.

Consecutive averages (above) and circadian swings (below) of SBP during ∼2-year alternate between mostly acceptable and rarely unacceptable. A 24-hour cosine fit to 7-day data sections removes the occasional abnormality (bottom) found in analyses of 24-hour data sections (top) in an elderly woman. Results from non-overlapping 1-day (top) and 7-day (bottom) intervals in serial sections on half-hourly around-the-clock data; OS (an 81-82-year-old woman) on atenolol treatment. When 1-day intervals are used, occasional unacceptable results occur.
Figure 14B.

Consecutive averages (above) and circadian swings (below) of systolic blood pressure (SBP) during ∼16-year alternate between mostly acceptable and rarely unacceptable. A 24-hour cosine fit to 7-day data sections reduces the extent of abnormality (bottom) found in analyses of 24-hour data section (top) in an elderly man. Results from non-overlapping 1-day (top) and 7-day (bottom) intervals in serial sections on half-hourly around-the-clock data; FH (a 71-87-year-old man) on varying treatments.
Figure 15A.

(Above and opposite) Percentages of vascular variability disorders (VVDs) or rather vascular variability anomalies (VVAs) and vascular variability syndromes (VVSs) missed in current practice. The incidence of VVDs in this graph is assessed in a clinic population of 297 patients. BP and HR of each subject were monitored around the clock for 2 days at 15-minute intervals at the start of study. Each record was analyzed chronobiologically and results interpreted in the light of time-specified reference limits qualified by gender and age. On this basis, MESOR-hypertension (MH, diagnosed in 176 patients), excessive pulse pressure (EPP), circadian hyper-amplitude-tension (CHAT), and deficient heart rate variability (DHRV) were identified and their incidence related to outcomes (cerebral ischemic attack, coronary artery disease, nephropathy, and/or retinopathy). Outcomes, absent at the start of study in these nondiabetic patients, were checked every 6 months for 6 years to estimate the relative risk associated with each VVD alone or in combination with 1, 2, or 3 additional VVDs, shown in columns complementing each circular display of incidences of variability disorders.
Earlier work showed that CHAT was associated with a risk of cerebral ischemic event and of nephropathy higher than MH and that the risks of CHAT, EPP, and DHRV were mostly independent and additive. It thus seemed important to determine the incidence of each VVD, present alone or in combination with one or more additional VVDs. Results from this investigation are summarized in this graph.
Results related to MH are shown in the upper section of the graph. The 176 patients with MH are broken down into 103 (34.7% of the whole study population of 297 patients) with uncomplicated MH, 55 (18.5%) with MH complicated by 1 additional VVD (EPP, CHAT, or DHRV), and 15 (5.1%) and 3 (1.0%) with MH complicated by 2 or 3 additional VVDs. In the latter group, all 3 patients had a morbid outcome within 6 years of the BP monitoring. Ambulatory BP monitoring over only 48 hours, used for diagnosis, is much better than a diagnosis based on casual clinic measurements, yet its results apply only to groups. With this qualification, of the 176 patients with MH, 73 (42.2%) have additional VVDs that further increase their vascular disease risk and that are not considered in the treatment plan of these patients since current practice does not assess these VVDs. This proportion may be smaller in a 7-day record (available for CHAT).
Results related to EPP (second row), CHAT (third row), and DHRV (bottom) illustrate that these conditions can be present in the absence of MH in as many as 12 (4.0%) of the 297 subjects. Since they do not have MH, it is unlikely that these subjects would be treated from a conventional viewpoint even though their vascular disease risk can be as high as or even higher than MH. Evidence suggests that treatment of these conditions may translate into a reduction in morbidity and/or mortality from vascular disease. Another lesson from these results is that around-the-clock monitoring of BP and HR interpreted chronobiologically is needed, even in the absence of MH, to detect vascular disease risk associated with VVDs such as CHAT and DHRV that cannot be assessed on the basis of casual clinic measurements so that nonpharmacologic and/or pharmacologic intervention can be instituted in a timely fashion before the occurrence of adverse outcomes. Once implemented across the board rather than in selected patient populations, vascular disease could be curbed to a much larger extent at relatively low cost if the monitoring is offered directly to the public and care providers become involved only after detection of a VVD. A website has to be built to interest many people and to provide cost-free analyses in exchange for the data, as is now provided worldwide by the BIOCOS project on a small scale.
Figure 15B.

Top 4 pie charts: incidence of a given vascular variability disorder (VVD) alone or in combination with other VVDs in a study population. Bottom pie chart: incidence of MESOR-hypertension alone or in combination with other VVDs in a study population. VVDs or rather vascular variability anomalies (VVAs) (lightest shading) are complicated to a differing extent by one or more added VVDs (darker shading). In this graph, MESOR-hypertension (MH) is diagnosed in a total of 289 subjects, representing 24.6% of the 1177 untreated, presumably normotensive subjects included in the study. Among these 289 subjects, as many as 137 (47.4% of those diagnosed with MH) have at least 1 additional VVD that is not part of the current screening but increases the vascular disease risk beyond that associated with MH alone. The 4 graphs illustrate that VVDs other than MH occur in the absence of MH in very few patients with excessive pulse pressure (EPP) and in more patients with circadian hyper-amplitude-tension (CHAT) and in yet more with ecphasia and in 87 patients with deficient heart rate variability (DHRV), that is for a total of 182 subjects, representing 15.5% of the study population. In this study, BP and HR data available hourly for only 24 hours were complemented by an assessment of the left ventricular mass index as a surrogate outcome measure. In addition to MH, EPP, CHAT, and DHRV summarized from another earlier study, ecphasia was assessed. The great limitation of a record covering only 24 hours is not overcome by the relatively large study population of 1177 subjects not treated with antihypertensive agents, yet results in keeping with those obtained in a clinic population of 297 patients suggest that MH is to be recognized as a VVD and that its risk can be very greatly increased when other VVDs combine into vascular variability syndromes that escape current diagnostics. None of the 1177 untreated subjects had 4 additional VVDs.
Figure 16.

An unheeded chronobiologic warning: eclampsia followed overswinging or circadian hyper-amplitude-tension (CHAT). Eight weeks later, convulsions began, and a boy in the 27th gestational week was delivered. The cost-accounted care during his first 13 months totals US $615 000; 26-month hospitalization may have increased the cost to about US $1 million. By sole reliance on the average blood pressure (of 115 mmHg systolic), disregarding our strong advice for bed rest and treatment in view of CHAT, a particular obstetrician did not prevent a very premature delivery, which happened to be avoided in all other deliveries in a National Institutes of Health–sponsored study in which chronobiologic advice usually resulted in bed rest and/or drug treatment without incurring major cost.
A chronobiologic approach works when a dipping classification can fail19,37,38 or dipping misleads39 on a small-group basis. It seems the more important to realize that dipping cannot be recommended for the diagnosis of individuals, even for 7-day records because it is not equivalent to C-ABPM,4,40,41 in keeping with Einstein's admonition to “make everything as simple as possible but no simpler.” Dipping is “simpler.”
When the diagnosis of MESOR-hypertension is made, the dose prescribed is preferably varied, starting with a time preceding the peak by several hours. Hence, the circadian acrophase of BP as a marker preceded by an interval whose length depends on the chronopharmaceutics of the drug(s) involved is a procedure that has yielded a faster desired response, with fewer side effects compared to traditional therapy (Figure 17, p 91) in the hands of Rina Zaslavskaya, MD, the leading chronocardiologist.42,43 If needed, the timing of the drug can next be varied empirically to find the optimum (Figures 18A and 18B, p 92).44 This is the more important since the same dose of the same drug in the same patient tested at 6 different circadian stages, for approximately 1 month at each time (at clock hours after awakening 3 h apart) can induce or enhance an existing CHAT at 1 test time or at another remove CHAT and lower BP, as intended (Figure 19, p 93).45,46 Sometimes, a single change in the timing of a medication can correct abnormality (Figure 20, p 94).2 Continued surveillance is indicated (Figure 21, p 95).2 The many millions receiving hypotensive drugs need not fly blind, concerning risks in Figures 9A and 9B (pp 76-77), while for security on the road we routinely automatically measure the pressure in automotive tires. Moreover, if we monitor ourselves continuously and automatically, we may learn about a new world of infradian rhythms that reflect physical environmental counterparts and relate to sudden cardiac death (Figure 22, p 96), suicide (Figures 23A–23D, pp 97-99), homicide (Figure 24, p 100), and terrorism (Figures 25 and 26, pp 100-101). We may even find, on a population basis, the antecedents (Figure 27, p 102)30,47 as well as the consequences48 of a tsunami accompanying an earthquake at some distance from its epicenter.
Figure 17.

Efficacy, safety, and cost effectiveness of chronotherapy vs traditional therapy with 3 antihypertensive drugs. There were 20 patients per group; hypotensive effect was more pronounced on CT than TT (P < .05). The chronocardiologist Rina Zaslavskaya was first to demonstrate a longer desired effect, by comparison to conventional therapy, by timing hypotensive treatment prior to the circadian peak in blood pressure, on a group basis, with less medication and fewer complications. Minnesotan meta-analysis.
Figure 18A.

Monitoring the mean seems successful, but what happens to the amplitude? Changing timing of medication (ĐRx) during consecutive spans shows efficacy of treatment. An empirical approach to chronotherapy: immediately after diagnosis, one should ascertain that the treatment is effective. Optimization of treatment effects by timing can be achieved for the individual patient by systematically changing, eg, advancing the time of treatment (in relation to hours after awakening). Successful treatment of MESOR-hypertension assessed by a self-starting cumulative sum control chart. To optimize his hypotensive treatment (Rx), a just-diagnosed 24-year-old individual (TT) switched his Rx first every 17 days by 4 h and then mostly at shorter intervals. Note statistically significant decrease in MESOR, evidenced by the breakout outside the decision interval of the negative CUSUM line. With continued Rx, the blood pressure MESOR leaves the decision interval, indicating a statistically significant decrease in overall blood pressure. (J Appl Biomed. 2006;4:73-86.)
Figure 18B.

Monitoring the circadian amplitude shows an otherwise silent putative large risk. Changing timing of medication (ĐRx) during consecutive spans shows risk of iatrogenic CHAT (Circadian Hyper-Amplitude-Tension). An empirical approach to chronotherapy: immediately after diagnosis, one should ascertain that one does not induce CHAT by inappropriate timing of anti-hypertensive medication. In this 24-year old man (TT) who advanced the time of treatment by 4 hours every 17 days initially and at shorter intervals thereafter, treatment in the evening was associated with an increase in circadian amplitude, raising the question whether the risk of MESOR-hypertension may not have been traded for the even higher risk of stroke that CHAT represents. Iatrogenic CHAT, induced by treatment is silent to office visits. One must not inadvertently trade benefit (lowering of the MESOR of blood pressure) for something worse (circadian overswinging of blood pressure). This danger applies to some hypertensives (who tend to have a large circadian amplitude of blood pressure) to whom treatment time is not specified by the care provider, as was the case for TT (or is specified for bedtime). A few others who took hypertensive medication at bedtime were also found to have CHAT. The figure also shows the assessability of otherwise undetected harm by as-one-goes sequential analysis.
Figure 19.

A popular drug, if prescribed without personalised surveillance, can induce a vascular variability disorder (VVD) such as Circadian Hyper-Amplitude-Tension (CHAT). A change in the time when the drug is taken can make the same dose of the same drug in the same person beneficial or vice versa. At one administration time (before noon), Hyzaar induces CHAT in diastolic blood pressure and exacerbates a preexisting CHAT in systolic blood pressure (red). At another time of administration, Hyzaar eliminates a pre-existing VVD (green). These opposite effects were found in tests at 6 medication times, each administered for about a month, with half-hourly surveillance of BP during the last week of each span. These differences occur as a function of the timing of the drug's use along the scale of 24 h. Original study of Yoshihiko Watanabe of a 66-year-old man treated with Losartan (50 mg) and hydrochlorothiazide (12.5 mg). Each point represents 1 week of half-hourly around-the-clock monitoring after ∼1 month on a given treatment time. After this graph was completed, treatment at AW + 15h yielded a SBP-A of 10.36 ± 2.09 mmHg and a DBP-A of 8.69 ± 1.85 mmHg. By cosinor, a circadian stage-dependent response to treatment could be shown to account, with statistical significance for both endpoints, for 39% and 32% of the overall variance, respectively.
Figure 20.

Individualized blood pressure chronotherapy. Lower circadian double amplitude (2A) and MESOR (M) after switching treatment time from 08:30 (left) to 04:30 (right).* The usefulness of a chronobiologic approach is supported by the demonstration that treatment with antihypertensive drugs can be optimized by timing. The same dose of the same drug can have different effects on the MESOR and circadian amplitude of the same patient's blood pressure when it is administered daily at a different circadian stage as seen by the naked eye and documented by parameter tests.
Figure 21.

Control chart assesses individualized anti-MESOR-hypertensive chronotherapy.* The chronobiological approach includes inferential statistical methods for the rigorous assessment of intervention effects applicable to the individual patient, eg, detecting whether the lowering in the MESOR of systolic (left) and diastolic (right) blood pressure can be associated with the time when the change in treatment timing was instituted.
Figure 22.

Geographic and time-varying differences in the spectrum of sudden cardiac death. A curtain of uncertainty, because of limited available data, hides any time- and geographic (geomagnetic or dip-magnetic) site-specificity of various spectral aspects of sudden cardiac death. Thus, we find a transyear (T) in Minnesota with a cis-half-year (cY/2) and both a calendar year (Y) and a transyear in Arkansas and the Czech Republic: at the latter site, a cis-half-year, corresponding in length to an also-transient period of hard solar flares, is detected after but not before 1999. Whether other geographic differences in sudden cardiac death may also relate to any magnetic latitude deserves scrutiny. It is noteworthy in any event that cardiac arrhythmias can also transiently reveal a transyear or a cis-half-year, each in a different Horrebow-Schwabe sunspot cycle stage.
Note site-specificity in the frequency domain displayed by patterns of sudden cardiac death worldwide. Time-specificity is seen at bottom left in the Czech Republic. Rhythms (spectral components) with one or several widely differing periods are found even when focusing solely upon the United States. (A phase difference of changes mirroring a didecadal [Hale sunspot bipolarity] cycle in newborns' body weight in Minnesota vs Denmark is documented by millions of cases; it shows that the local setting on earth, while depending upon input from the sun, also plays a major role.)
Note differences within United States and vs Europe, Middle East (Georgia), and Asia (Hong Kong).
*T, transyear; Y, calendar year; cy/2, cis-half-year.
Figure 23A.

Daily incidence of suicide by day of death in the 2 genders in Minnesota (1979-2007). Top: Signatures of the seasons (1.0 y), geomagnetics (0.5 y), and solar dynamics (∼17, ∼9.8, ∼1.3, and ∼0.28 y); men, N = 11 371. Bottom: Hale (∼24-y) and extra-annual and extra-semiannual components with periods of ∼1.43, ∼1.07, ∼1.02, and ∼0.37 years; women: N = 2794. In addition to a circannual and circasemiannual variation, a far-transyear is detected by least squares spectra, with a slightly different period in males (∼1.28 years) and females (∼1.43 years). A near-transyear is detected in females but not in males.
Figure 23D.

Suicides in England and Wales by day of birth reveal a different spectrum without the transyears found in Minnesota by day of death.
Figure 24.

The Kondratiev and Hale cycles are mirrored in US homicides (1900-1998). National Center for Health Statistics (Homicide rates from the vital statistics: http://www.ojp.usdoj.gov/bjs/glance/hmrt.htm).
Figure 25.

(Opposite, bottom) A gliding (local, left) and aligned overall (global, right) spectral window (A, left) show similarities in the para-annual region, a transyear around 1.33 years in solar wind speed (SWS, top), the antipodal geomagnetic disturbance index (aa, middle), and in the incidence of terrorism in the MIPT's (Memorial Institute for the Prevention of Terrorism) 39-year-old database (bottom). Phases of chronomic serial sections are shown for the transyear at the average period for the three variables (B, right). The transyear is observed to be particularly prominent in all three variables during solar cycle 22, as seen from the darker shading at a frequency of 1 cycle in about 1.33 years. Changes with time of the phase of the transyear component indicate further that statistical significance for terrorism relatively shortly follows (with only a lag) that in solar wind speed and geomagnetism and that it may persist, in terrorism for quite a while, after statistical significance is lost for the two environmental variables. Despite some expected wobbliness, the transyear appears to be relatively stable in all variables during most of solar cycle 22. The fact that a predictable cycle characterizing the incidence of terrorism is also present in the physiology of individuals renders it amenable to monitoring by a population marker rhythm for further scrutiny and for the eventual design of rational countermeasures against undesirable effects of the cosmos. Gliding spectra prepared by Professor George S. Katinas.
Figure 26.

In data then available from the Memorial Institute for the Prevention of Terrorism's (MIPT) Terrorism Knowledge Base (1968-2008) (http://www.tkb.org/) (top), a transyear of ∼ 1.3 years is detected in the absence of a calendar year component, suggesting that space weather (gauged by magnetism) is more important than any (absent) effect of the seasons. From February 1968 to March 2007, daily incidence computed from monthly totals (adjusted for differences in the number of days per month).
Figure 27.

Proposed biospheric contributions to the understanding, if not prediction of earthquakes. Upper left: Locomotor activity of some of the mice telemetered around the clock was statistically significantly decreased starting 3 days prior to the magnitude 8.0 earthquake in Chengdu, China on 12 May 2008. Upper right: Human systolic blood pressure started increasing 2 days prior to the magnitude 9.0 earthquake in Sendai, Japan on 11 March 2011, documented on the basis of weeklong records of around-the-clock ambulatorily obtained data from 13 Japanese. Similar records from longitudinal and transverse controls differ in their time course, suggesting that the trend observed before the earthquake was related to it rather than being a feature of an anticipated weekly pattern. Lower left: The monthly incidence of major earthquakes since 1900 is characterized by the presence of cycles with periods of about 49.3, 12.2, 1.44, and 0.41 year(s), given with their uncertainties in parentheses. Lower right: The prominent about–50-year cycle is also documented in physiology, pathology, societal upheavals and space weather. Nonlinearly estimated periods are displayed with their 95% confidence intervals shown as the length of corresponding horizontal bars. N = 331.
Multiple Circadian Rhythms and beyond
Time series collected and accumulating for the goal of self-surveillance, once aligned with physical environmental time series, enlarge the scope of Vladimir Ivanovich Vernadsky's noösphere,49,50 the sphere of the human mind by a chronosphere, a trans-disciplinary spectrum of cycles congruent insofar as their periods in us and around us have overlapping confidence intervals (CIs 95%) (Figures 28A–28H, pp103-109).51–54 Our inclusion of the moon in Figure 28B (p 104) is in keeping with studies on his own heart55 by Miroslav Mikulecky, emeritus head of internal medicine and professor of statistics at Comenius University in Bratislava, Slovakia, and organizer of meetings on this and related topics.56–60 It is here prompted by the first patient encountered by us who shows the double period of tides61 averaging 24.8 hours, repeatedly in the computer output (not input) of analyses of time series.
Figure 28A.

Frame on lower right half lists some components of the transdisciplinary set of cyclic components found in the bio- and/or in the litho-, hydro-, atmo-, iono-, helio-, magneto- and cosmospheres, underlying a time-structured sphere of the human mind (Attic Gk nous), the chronousphere.
Figure 28H.

Distribution of period estimates, τs (histograms on left, individual results on right, shown with their 95% confidence intervals [CIs]) displayed as a function of time (upward) along the ordinate for a 54-60-year-old woman (GC), based on around-the-clock ∼24-hour/7-day records at 30-minute intervals. Monthly summaries of a patient's (JF's) τ and CI during “downtimes” (shaded) and outside such episodes of loss of vigor are shown (right, top of each section). The first winter adynamia (shaded) is characterized for SBP by 2 consecutive τs longer than 24.8 hours for JF, a finding not seen in GC. For all 3 of GC's variables, desynchronized τs are rare and are absent in a sequence, while in JF's second upper adynamic episode, based on automatic measurements, desynchronization from society is the rule: the CIs of τs invariably fail to cover 24 hours.
*JF (above dashed lines): estimates during consecutive lunar cycles; GC (below dashed lines): circadian rhythm invariably detected (P < .05) in about week-long (rather than month-long) spans.
Figure 28B.

Chronousphere: genetically coded biospheric resonance including terrestrial luni-solar and/or cosmic cycles. Signatures of the cosmos with validated statistical significance of anticipated periods characterize (1) dozens of decades-long time series of human blood pressure and heart rate; (2) other physiology and psychology, including human mental functions; (3) religious proselytism; (4) suicide; (5) sudden cardiac death; (6) terrorist activity for the past 39 or 41 years; (7) 2556 years of international battles compiled by Raymond Holder Wheeler; (8) military expenditures for training in non-medical science; (9) degrees earned; (10) Gallup Polls; and (11) political and military actions in nearly 200 years, meta-analyzed from the much broader treasure of data compiled by Alexander Leonidovich Chizhevsky. While chance can never be ruled out, it would be further greatly reduced by systematic lifetime monitoring of physiology in health, of pathology and disease, notably in archives to separate effects of sun, tides, and earth, many of which are beneficial. Other effects such as extreme cold and heat or extreme light can be met by countermeasures such as housing, heating and air conditioning. The task remains to develop countermeasures to those nonphotic effects that can be documented as harmful. While the earth is the immediate actor, and for that action the sun is the modulator, the biosphere reacts directly, yet sometimes selectively to only 1 (or both) terrestrial and lunisolar factors, the tides, as well as natural and artificial light competing with each other under certain circumstances, as seen in patient JF (Figures 28C–28G). There may be other more subtle effects of synchronized human action upon the earth. Effects of the moon, contributing about two-thirds of the tides, are thus also demonstrated (Figures 25C–25G). The roles of actor, reactor and modulator are continuously changing. In the greenhouse effect, organisms are the actors, as shown by a double-headed arrow (B2). Original compilation by Mary Sampson.
Figure 12B.

Meta-analyses in Minnesota on diagnoses made in response to a set of ambulance calls in Moscow are confirmed and extended by Villoresi G, Breus TK, Iucci N, Dorman LI, Rapoport SI. The influence of geophysical and social effects on the incidences of clinically important pathologies (Moscow 1979-1981). Physica Medica. 1994;10:79-91. Top: Southward turns of the vertical component (Bz) of the interplanetary magnetic field's induction vector and prior changes (for BP) affect pathology and physiology: Halber et al, 1991. Bottom: Confirmation of Bz effect and extension to AA and FD effects on pathology: Villoresi et al, 1994. Means ± SE (vs all other days = 100%: horizontal line); *P < .05; NS: P > .05.
Figure 12C.

Demonstration of about 10.5-year cycle in mortality from myocardial infarction in Minnesota (1968-1996) after removal of decreasing linear trend, aligned with about 10.5-year solar activity cycle. Fitted curves represent fundamental component as a first approximation that does not account for the asymmetry of the solar activity cycle considered in Figure 12D. Minnesota data on myocardial infarction and solar activity (Figure 12A) reveal association of the latter with the former (Figure 12D).
JF is a woman, 61 years of age, at start of a years-long around-the-clock study, including C-ABPM, with a 20-year history of twice-yearly adynamic depression, each lasting 2 to 3 months. During “downtimes,” JF is unable to get out of bed and to keep synchronized with a 24-hour periodic sleep-wake schedule. Her sleep pattern scans the hours of the day during her episodes. She self-rated vigor-wellness while claiming sensitivity to the moon. In the first months of the first two adynamic episodes investigated, we found a double tidal period of 24.8 hours supporting her impression of selenosensitivity. JF self-measured BP and HR for 5 initial months and for >16 months thereafter (Figure 28D, p 106). At least 2 circadian periods coexist most of the time (Figure 28E, p 107). She also collected saliva at 4-hour intervals around the clock for the determination, in 11 702 assays, of cortisol, aldosterone, dehydroepiandrosterone, estradiol, testosterone, and melatonin (Figure 28F, p 107), showing multiple recurring circadian endocrine as well as vascular ecfrequentia. Several circadian periods were also present in her outside downtimes during relative wellness,62 suggesting a “wrangling” of the tides with society and natural and artificial light. We may speculate whether the tides act via gravity and magnetism, a view shared with physicist-chemist Dr Vladimir Evstafyev63 and Prof Mikulecky (their personal communications), acting by mechanisms considered by Friedemann Freund.64 In any event, in JF, this tug of war yields (compromise?) periods between 24.0 and 24.8 hours except that during some of the first months of an adynamic desynchronized episode, a precise average double-tidal period prevails. The diagnosis in JF of dysfrequentia, visualized by a comparison with an age- and gender-matched control in Figures 28G and 28H (pp 108-109) can be made by C-ABPM (but not by self-measurement, a highly motivated JF notwithstanding, in keeping with earlier results65).
Figure 28D.

Self-measurements of systolic blood pressure of JF, from lunar cycles (vertical dashed lines) 4 to 8 inclusive, followed by automatic monitoring in lunar cycle 8. Original data on top reveal lack of lower values during rest/sleep. The lower curve in the second row is the circadian average (MESOR), which is higher during measurements restricted to wakefulness. The circadian amplitude, the distance between the 2 curves in the second row, is small and not statistically significant, as seen from the penultimate row of P values for test of the zero 24-hour amplitude assumption in cycles 4 through 8. Note acrophases in row 3, shown with 95% confidence interval when statistical significance is reached (ie, as soon as automatic measurements start in lunar cycle 9 to the end). Their time course continues in alternation horizontally (during wellness) and upward diagonally (during adynamia), thereby indicating a changing dominance between the 24-hour synchronized and desynchronized circadian components of variation, a wrangling of the tides with society in JF.
Period: 24 h; Interval: 168 h; Phas ref: 01/01/09; Start time: 03/01/09; End time: 04/15/09; No. of data: 10 078; Increment: 12 h.
Figure 28E.

Coexisting societal-light 24-hour (dots) and tidal 24.8-hour (diamonds) components dominating during wellness and illness, respectively, in JF's (a 62-year-old woman) blood circulation.
Figure 28F.

Competition of 24.0-hour (light and society) and 24.8-hour (tides) periods in JF's endocrines with 24-hour dominance during wellness and the tides pulling most during illness. N = 11 700 salivary hormonal assays (JF: 61-62-year-old woman; 20 years of adynamic episodes lasting 2-3 months and recurring half-yearly).
Figure 28G.

Chronobiologically interpreted automatic ambulatory blood pressure (BP) and heart rate (HR) monitoring (C-ABPM) monitors circadian ecfrequentia of JF (top) by comparison to a gender- and age-matched control, GC. Circadian acrophases of systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR) from 11/03/09 to 10/12/10 for both subjects. Fit of 24-hour cosine curve to data in 168-hour intervals, displaced in 12-hour increments for consecutive analyses. Acrophases are doubly plotted (top) when nearing midnight, indicated by horizontal dashed lines at 0° and 360°. More or less horizontal time course = 24-hour synchronization. ⇊ indicates brief trans-meridian roundtrip across 8 time zones.
Cycles in us, such as the physiological week, among others, led to natural geomagnetic near-weeks (Figures 29A and 29B, p 110).51 Reports of new cycles by physicists prompted our discovery of coperiodic biospheric signatures of the cosmos such as approximately 5 or 16 months long (Figures 30A–30C, pp 111-112)34 and other cycles (Figures 31A–31C, pp 113-115).53,54 There are further cross-spectral coherences54,66–68 and phase synchronizations68 between endpoints around us, such as Bz, Kp, Wolf number, or coronal mass ejection or cosmic rays and urinary variables or the decades-long monitored BP of individuals. Associations are also seen from cross-wavelets and coherence between myocardial infarctions of populations or the incidence of terrorism on the one hand and space weather on the other hand (Figures 32A–32D, pp 115-117). We trust that with Figures 33 and 34 (pp 118-119), among others, a chronouspherea emerges, consisting of many infradians with periods longer than 28 hours up to myriadennians.69,70 For some of the infra-dian pairs of periods, the disappearance or reappearance of the environmental (eg, solar) or interplanetary component entails corresponding biospheric consequences (Figures 34–36, pp 119-121).44,61,62 The approach by removal of a gland and replacement of its hormone started endocrinology and eventually chronobiology.71 Investigation seems indicated not only by mapping51,54,71–74 but also by the subtraction and/or addition approach44,75 (or preferably by the remove-and-replace approach implemented by the sun), notably for those in healthcare interested in the effects of space weather.34
Figure 29A.

Congruence in certain environmental circaseptan spectral components and in some cardiovascular counterparts during 1998-2005. *Selective transdisciplinary congruence in the spectral region around 1 week.
*All peaks are statistically significant (P < .001) by linear-nonlinear least squares cosinor spectra (not corrected for multiple testing). HR, SBP, and DBP (N = 124 263 each) – half hourly records of GSK, a 72-year-old-man at start of around-the-clock monitoring, Data: SW (N = 68 845) hourly values from http://omniweb.gsfc.nasa.gov/ Dst, Ap, and Kp 3-hourly data (N = 23 376 each) from http://spidr.ngdc.noaa.gov/.
**CI = confidence interval.
***Two separate spectral peaks without CI-overlapping.
****All available daily SW data during 1963-2005.
Figure 29B.

Combination of gliding spectral window (top) with special focus on the behavior of 2 selected periods (chronomic serial sections, middle and bottom), with the time course of the phase validating the 6.77-day period by a more or less horizontal trajectory of phases bracketed by CIs (dots) indicating statistical significance in only part of the record, but invalidating a precise 7-day periodicity since with this fit no dots bracket any horizontal time course of phases, and the small initial section with dots shows a gradual advance (rather than being horizontal).
Data from http://omniweb.gsfc.nasa.gov/html/ow_data.html. In gliding spectral window, interval = 1 year, increment = 1 week; shaded areas show percentage of rhythm (from 1.2% to 6.8%). Statistical significance seen as 95% confidence intervals of φs shown as dots bracketing curves (middle and bottom). Reference time: 00:00 on December 21, 1997. Dotted arrows indicate correspondence between circaseptan components in the phase (middle and bottom) and period (top) domains. Twenty-third solar cycle began in May 1996; its maximum was in April 2000, and the cycle still continued descending after the end of record.
Figure 30A.

Waxing and waning of the aeolian ∼5-month (∼0.41-year) cycle in solar flares (top), sunspots (middle), and with a lag in the heart rate of a clinically healthy man (RBS). Concomitant changes occur in sudden cardiac death incidence not here shown. Influence of solar flares (SF, A, × in C) and sunspots (B) on human heart rate amplitude (HR-A, φ in C) in cis-half-year window suggested by shared ∼11-year cycle andhigh cross-correlation (HR-A vs SF) with 3.2-year lag (D): a helio-geo-bio-feedsideward (E).
Figure 30C.

Far-transyears around us (top 10 rows), incidence of myocardial infarctions in Minnesota and in 43 blood pressure and heart rate records from 13 subjects who each provided longitudinal records covering several years. The trans-year (a ∼1.3-year component) in the cosmos (top 10 rows), pathology (myocardial infarction), and physiology (bottom 43 rows)—all differing by non-overlapping 95% CIs from the precise calendar year and many differing among each other, a putative hint of endogenicity. Similar results found for another man providing 3 additional series.
Figure 31A.

Paradecadals and paradidecadals, ∼10.5- and ∼21-year cycles similar in length to the Schwabe and Hale solar activity cycles characterize a host of biological variables, from micro-organisms to human physiology, pathology, anthropometry, and sociology, assessed from population statistics, yet critically dependent upon also-available individual “pilot studies.” Such self-experimentation is indispensable for a scrutiny of mechanisms underlying population cycles.
Figure 31C.

Kondratiev cycle beyond economics in the biosphere. Transdisciplinary mapping of about 5-year spectral components.
Figure 32A.
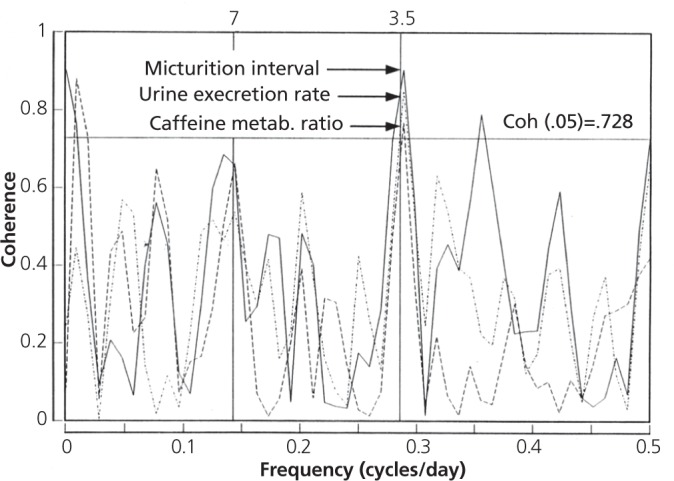
Coherence at a period of about 3.5 days is found between the daily standard deviation of hourly neutron monitor courses from Dourbes, Belgium, and daily values for the inter-micturition interval, urine excretion rate and caffeine metabolite ratio of a woman (VLG) during social isolation in a cave. The coherence values are 0.90 (P = .001), 0.85 (P = .006) and 0.77 (P = .029) for each variable, respectively, calculated by standard approximate χ2. At a period of about 7 days, similar agreement is found among the three variables, albeit coherence with the environmental variable is not statistically significant.
Figure 32D.

(Above and opposite) Cross-wavelet coherence with Wolf numbers (WN, gauging solar activity, above) differs between the incidence of myocardial infarctions (MI) in Minnesota (next page, left column) and the incidence of international terrorist acts (TA, from the total Global Terrorism Database, next page, right column). Whereas a low-frequency component is visible in the wavelet spectra of all 3 variables (left) and in the cross-wavelets of MI and TA with WN (middle), only MI (but not TA) shows coherence in this region.
Figure 33.

Anticipated influence of the antipodal index of geomagnetic disturbance “aa” (top) and of the non-photic environment (gauged by solar wind speed, an approximation of interplanetary magnetism) on human psychophysiology was assessed by means of the congruence of periods of their spectral components (defined by overlap of the 95% confidence intervals of the periods, Đs, in the frequency range of one cycle in 2.5 years to 3 cycles per year). The biological data stem from 40 years of self-measurements of oral temperature (Temp), systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) and of ratings of mood and vigor and the estimation of 1-minute by counting (1MTE), performed about 5 times a day by a clinically healthy man, Dr Robert B. Sothern. Congruences (assessed by means of odds ratios based on the noncentral hypergeometric distribution) found for 1MTE and for several other variables more than equal that of the known association of helio- and geo-magnetism (bottom, last column on right). Mental functions (full red) show higher congruence than somatic functions (green). Among the latter, SBP is responsive, perhaps constituting a seemingly acceptable proxy for the mental functions. P values are based on the non-central Fisher hypergeometric distribution, with 95% confidence intervals computed using Fisher's exact test, used since the null hypothesis was rejected in some but not all cases.
Figure 34.

The transyear can prominently characterize solar wind speed, as shown in the top gliding spectral window by the wide dark band around 1.3 years (vertical scale are frequencies in the range of 1 cycle in 2 to 0.7 y). This component, however, is Aeolian in nature, its characteristics (frequency and amplitude) changing as a function of time. This is exemplified around 1998 (E) when its amplitude is considerably decreased (the darker the band, the larger the amplitude). After E, the transyear is no longer detected in solar wind speed. A transyear is also found to characterize systolic blood pressure (SBP) of a man (FH) who monitored himself around the clock for more than 23 years (with interruptions), as seen in the gliding spectral window (row 2). With a lag (at E'), the transyear in FH's SBP is dampened but remains detectable, suggesting that the frequencies characterizing the solar wind may still drive us and may be built into us since they persist in the absence of a counterpart in the Sun. Somewhat similar results are suspected by some viewers for diastolic blood pressure (DBP, row 3) and heart rate (HR, row 4), but they are most clearly apparent only for SBP.
Figure 36.

About-weekly (circaseptan) resonance of human mortality from myocardial infarction with solar circaseptans demonstrated by “remove and replace” approach.* This approach focuses on a weekly component by investigators from the Republic of Georgia who built a clinical facility to study effects of geomagnetism.
DISCUSSION
In confronting congruent cycles in us and around us, the biospheric cycles when they are coded in our genes may reflect what goes on and went on outside us from the origins of living matter more reliably than the relatively recently recorded corresponding physical cycles. The dynamics of the cosmos almost certainly went on for a very long time and have left their mark in our makeup. We have just begun to scratch the surface of measurement. A record of polar lights and sunspots traces only a millennium or less; time series of sun-related, interplanetary, lunar, or geomagnetic variables cover a much shorter span; recordings by satellites of interplanetary, solar, and cosmic variables are still more recent. None of them, however, matches in density or length the dynamic information provided by cycles in living matter.
In this context, the cycles of the biosphere, mimicking those of the cosmos, constitute another novel way of dating and certainly serve to validate, as magnetometers or cosmometers, the relatively recent physical counterparts.52 This dating by mapping reveals a set of transdisciplinary cycles pervading all disciplines, each a sphere of the human mind (also Attic Greek nous) yielding a novel time structure. We can get much information about such a chronousphere by monitoring ourselves with repeated passes over the accumulating data as a whole (globally) and in sections of varying lengths (locally)—that is glocally in time and glocally in space, eventually from the womb to the tomb in the individual and in the population.
In the first issue of Global Advances in Health and Medicine, McCraty et al,76 and in another journal, McCraty and Childre,77 presented the Global Coherence Initiative aimed at a shift from “competition” to “greater cooperation” in a coherent planetary standing wave. The “increased power of connected intention and consciousness,” also a topic of interest in Michael Persinger's78,79 and Hans Wendt's80 research already explored at atomic and quantum81 levels, should all prompt attempts to seek better measures of coherence beyond those used herein from macroscopic physics and time series analysis. Perhaps the language of frequencies within them and far outside Schumann's resonances is pertinent, that yielded Figure 23 and remove-and-replace approaches in arriving at Figures 24 to 26 constitute a step in that direction.
It seems the more important to assess the status quo of information measured as tangible “coherence,” the topic of this paper. From this viewpoint, C-ABPM, while worth implementing for immediate health benefit, once it is aligned with physical environmental monitoring provides marker rhythm information concerning both environmental magnetism and other nonphotic factors competing with oscillations in the visible range.
The findings herein of a largely novel spectrum of transdisciplinary components—the chronosphere and its entry into the noösphere (ie, the chronousphere)—constitute a complement to work by a great many others.82–89 Most pertinent are Alexander Leonidovich Chizhevsky's heliobiology and Vladimir Ivanovich Vernadsky's even broader noösphere. Bernhard and Traute Düll,90 Harlan True Stetson,91 Alexander P. Dubrov,84 Frank A. Brown Jr,85 and Rutger Wever86 pioneered in the field, as did Sergei M. Chibisov87 and Tamara Breus,88 contributing a review of the status quo in Russia.89
Many tasks remain to reach two goals: (1) a miniaturized, unobtrusive, and ambulatorily functional C-ABPM device that is affordable to all and communicates with (2) an also automated, manned website providing analyses of several kinds of incoming data flows such as (a) physiological, to start with of BPs and HRs; (b) epidemiological, to start with of natality, morbidity, and mortality; and (c) sociological, to start with military, political, and criminological (time series). The feasibility of a device costing less than $100 has been demonstrated,92 as well as the ability of glocal analyses in space and time of all 3 kinds of time series (a, b, c) as steps in concept validation and feasibility demonstration.4,53 For the epidemiological data analyses, which should be ongoing as natality, morbidity, and mortality data accumulate, state health departments constitute a major hurdle: a few offer to sell these data or just refuse to provide them in the United States, as was the case in 45 of 48 states to which requests for data were sent. The time has come for realizing that replacing baselines for all statistics with mapped cycles is the mandate of the health department, of the World Health Organization and of the United Nations; analyses of epidemiological data are their job. Here, governmental action is required to place as a minimum the data into the public domain and as an optimum to have health departments realize the need for retrospective and ongoing analyses. The biggest hurdle, however, is the attitude of well-meaning teachers currently prevailing in medical schools, where the majority are unaware that continued reliance on a single BP measurement or a single 24-hour profile will leave many people who need treatment untreated, and equally regrettable, many people who may not need treatment will be treated. The proposition that it would be best to perhaps give an antihypertensive drug to everybody reaching a certain age is the best documentation of the fact that concern about “do no harm” is forgotten and the need to diagnose variability disorders leading to personal severe disease (such as stroke) and to other social disasters (such as crime or terrorism) or to natural cataclysms (such as earthquakes) is ignored. An alternative is available in the project on The BIOsphere and the COSmos, BIOCOS.
CONCLUSION
The BP cuff in the healthcare provider's office must go for the moment to the homes of each individual. In the 1960s and 1970s, it seemed worthwhile to plead, as Frederic C. Bartter also did, for moving the BP cuff from the providers' offices to everybody's (including his own) office by day and home by night. This recommendation holds until a system of C-ABPM becomes affordably available to everybody. Bartter advocated this as head of the Hypertension-Endocrine Branch at the US National Institutes of Health (NIH) and later as head of the NIH's Clinical Center. In 2012, self-measurements at home have detected an effect of the great earthquake in Japan, proving their value.48 They confirmed, if not the finding of antecedents30,47 at least the consequences of the same quake found on a small scale yet worldwide in a de facto validation test of an ongoing C-ABPM system, serving for cost-free analyses of self-surveillance data by all comers.
Figure 23B.

Suicides in Australia by day of death and gender, 1968-2001. Top: Seasons' (1.0 y) and geomagnetics (0.5 y) signatures in men joining solar 9.2- and 0.42-year.* Bottom: Extra-annual and extrasemiannual putatively solar about 0.56-year, a 1.21-[trans]year and a 9.2-year component in women.** The circannual component is prominent in males but not in females. A far-transyear is detected for both genders, albeit with different periods.
Figure 23C.

Suicides in Bulgaria by day of death (1929-1945). In addition to the prominent year, the half-year, a transyear, and a cis-half-year are also detected.
Figure 28C.

Replicated lunar synchronization of JFF's vigor during first month (shaded) of (2-month-long) adynamia episodes.* Chronomic serial section of self-rated vigor-wellness of JF, a woman aged 61 years at start of study during the first 14 lunar months of investigation, revealing extreme changes in vigor and mostly a lack of statistical significance of 24.0-h (row 4) and 24.8-h (row 6) cosine fits. Lunar cycles 4 and 11, the first months of the first two episodes of depression investigated, are characterized by a delaying acrophase when a 24-h cosine is fitted and, as anticipated, by a more or less horizontal time course with a 24.84-h cosine fit (rows 3 and 5 respectively). Each first month of an adynamic episode in nonlinear analyses is characterized by a 24.8-h period twice in succession, never found by us earlier (also further in other variables of JF during adynamic episodes).
Figure 30B.

Near-transyears around us (rows 1-6) and in living matter (rows 7-10).
Figure 31B.

Key to Figure 31A.
Figure 32B.

Cross-spectral coherence between daily incidence of myocardial infarctions* and the Bz-GSE component of the interplanetary magnetic field (1979-1981). Multiple coherence findings depend, of course, upon resolution used.
Figure 32C.

- Phase synchronization does not depend on the amplitudes of rhythms. It appeals also for rhythms with low amplitudes.
- Phase synchronization signals a strong phase coupling between different oscillators. Thus, it is an indicator for a common time regime of different processes.
Figure 35.

A ∼7-day spectral component in the heart rate of 5 men is less prominent when the solar wind loses its counterpart of corresponding length. Implied, but not shown, is the persistence in the biosphere of a ∼7-day component that can be amplified (driven) by a reciprocal component in solar activity.
- Is dampened in the absence of a solar counterpart (blue, still driven after subtraction of solar wind) yet (not shown)
- It persists (since it is genetically anchored).
Footnotes
Dr Howard Levine, the late head of medical education at the New Britain (Connecticut) General Hospital and professor of medicine at the University of Connecticut, implemented self-measurements of blood pressure, heart rate, and other performance variables, including grip strength, around the clock from the time of a chronobiologic diagnosis of MESOR-hypertension until the end of his life from amyotrophic lateral sclerosis, his weakness notwithstanding.
Dr Bartter also self-measured BP around the clock from the time of diagnosis until a fatal stroke.
Halberg et al wrote in 1997, “Even a single heartbeat, however faint, will rule in at least a glimmer of life. The taking of the pulse for only a second or two then provides valuable information as to the merits of further efforts in resuscitation. But if the pulse were routinely taken for only a second or so, a bradycardic athlete in the best of health might be presumed dead!”27
From Greek chronos, time; Attic Greek nous, mind; and Greek sphairos, globe. We used nous in the portmanteau'd chronousphere to credit Vladimir Ivanovich Vernadsky, Pierre Teilhard de Chardin, and Edouard le Roy, who used the derivation of noosphere from noos, recognizing the need for a sphere of the human creative mind or broader culture, courageously extrapolating beyond the sphere of available data (criticized by Hagemeister M. In: Rosenthal BG, editor. The occult in russian and Soviet culture. Ithaca: Cornell University Press; 1997. p. 185-202, yet endorsed with extensive study by Ertel S. Stud Psychol. 1996;38:3-22). Cosmism's pioneers as yet did not have the means (computers and satellites) for detecting and documenting the pervading transdisciplinary spectrum of solar, interplanetary, geopheric, and biospheric cycles and the consequences in the human mind of the aeolian disappearance and/or reappearance of nonphotic rhythms.
Contributor Information
Franz Halberg, Franz Halberg, MD, Dr hc mult, is professor of laboratory medicine and Pathology at the Halberg Chronobiology Center at the University of Minnesota, Minneapolis..
Germaine Cornélissen, Germaine Cornélissen, PhD, is professor of integrative biology and physiology and director at the Halberg Chronobiology Center at the University of Minnesota, Minneapolis..
Dewayne Hillman, Dewayne Hillman, PhD, is a consultant at the Halberg Chronobiology Center at the University of Minnesota, Minneapolis..
Larry A. Beaty, Larry A. Beaty, BS, is the senior member of the Phoenix Study Group, composed of volunteering members of the Twin Cities chapter (Minneapolis) of the Institute of Electrical and Electronics Engineers..
Shiyu Hong, Shiyu Hong is a student of statistics at the Halberg Chronobiology Center at the University of Minnesota, Minneapolis..
Othild Schwartzkopff, Othild Schwartzkopff, MD, FAAP, is an assistant clinical professor of pediatrics at the Halberg Chronobiology Center at the University of Minnesota, Minneapolis..
Yoshihiko Watanabe, Yoshihiko Watanabe, MD, is an associate professor and cardiologist at Tokyo Women's Medical University, Medical Center East, Japan..
Kuniaki Otsuka, Kuniaki Otsuka, MD, is a professor and hospital president at Tokyo Women's Medical University, Medical Center East, Japan..
Jarmila Siegelova, Jarmila Siegelova, MD, is professor and head of the Department of Functional Physiology and Rehabilitation, St Anna Hospital, Masaryk University, Brno, Czech Republic..
REFERENCES
- 1.International Congress: Natural Cataclysms and Global Problems of the Modern Civilization; 2011 September 19-21; Istanbul, Turkey [Google Scholar]
- 2.Halberg F, Cornélissen G; International Womb-to-Tomb Chronome Initiative Group Resolution from a meeting of the International Society for Research on Civilization Diseases and the Environment; 1995 March 17-18; Brussels, Belgium [Google Scholar]
- 3.Halberg F, Cornélissen G, Otsuka K, et al. Chronomics detects altered vascular variabilities constituting risks greater than hypertension: with an illustrative case report. In: Mitro P, Pella D, Rybar R, Valocik G, editors. Proceedings of the 2nd Congress on Cardiovascular Diseases; 2002 April 25-27; Kosice, Slovakia Bologna: Monduzzi Editore; 2002. p. 223–58 [Google Scholar]
- 4.Halberg F, Cornelissen G, Otsuka K, et al. ; BIOCOS project Extended consensus on need and means to detect vascular variability disorders (VVDs) and vascular variability syndromes (VVSs). Geronto-Geriatrics: Int J Gerontology-ChronomeGeriatrics 2008;11(14):119–46 [Google Scholar]
- 5.Halberg F, Cornélissen G, Halberg F, Kessler T, Otsuka K. Measuring mental strain by duration of blood pressure overswing (CHAT): case report. World Heart J. 2010;2(2):47–73 [Google Scholar]
- 6.Halberg F, Cornélissen G, Spector NH, et al. Stress/strain/life revisited. Quantification by blood pressure chronomics: benetensive, transtensive or maletensive chrono-vasculo-neuro-immuno-modulation. Biomed Pharmacother. 2003October;57Suppl 1:136s–63s [DOI] [PubMed] [Google Scholar]
- 7.Maschke C, Harder J, Cornélissen G, Hecht K, Otsuka K, Halberg F. Chronoecoepidemiology of “strain”: infradian chronomics of urinary cortisol and catecholamines during nightly exposure to noise. Biomed Pharmacother. 2003October;57Suppl 1:126s–35s [DOI] [PubMed] [Google Scholar]
- 8.Halberg F. Organisms as circadian systems; temporal analysis of their physiologic and pathologic responses, including injury and death. In: Symposium on medical aspects of stress in the military climate Washington DC: US Government Printing Office; 1965. p. 1–36 [Google Scholar]
- 9.Halberg F, Smith HN, Cornélissen G, Delmore P, Schwartzkopff O; International BIOCOS Group Hurdles to asepsis, universal literacy, and chronobiology—all to be overcome. Neuro Endocrinol Lett. 2000;21(2):145–60 [PubMed] [Google Scholar]
- 10.Halberg F, Drayer JI, Cornélissen G, Weber MA. Cardiovascular reference database for recognizing circadian mesor- and amplitude-hypertension in apparently healthy men. Chronobiologia. 1984Jul-Sep;11(3):275–98 [PubMed] [Google Scholar]
- 11.Whitworth JA; World Health Organization, International Society of Hypertension Writing Group 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003November;21(11):1983–992 [DOI] [PubMed] [Google Scholar]
- 12.Verdecchia P, Porcellati C, Schillaci G, et al. Ambulatory blood pressure. An independent predictor of prognosis in essential hypertension. Hypertension. 1994December;24(6):793–801 Erratum in: Hypertension. 1995 Mar;25(3):462 [DOI] [PubMed] [Google Scholar]
- 13.O'Brien E. Dipping comes of age: the importance of nocturnal blood pressure. Hypertension. 2009March;53(3):446–7 [DOI] [PubMed] [Google Scholar]
- 14.Stolarz K, Staessen JA, O'Brien ET. Night-time blood pressure: dipping into the future? J Hypertens. 2002November;20(11):2131–3 [DOI] [PubMed] [Google Scholar]
- 15.Staessen JA, Bieniaszewski L, O'Brien E, et al. Nocturnal blood pressure fall on ambulatory monitoring in a large international database. The “Ad Hoc” Working Group. Hypertension. 1997January;29(1 Pt 1):30–9 [DOI] [PubMed] [Google Scholar]
- 16.Halberg F, Cornélissen G, Schwartzkopff O. In memoriam— Howard Burchell: Lifetime chronobiologically-interpreted (C-) ABPM for strain assessment for everybody, with diagnostic dividends. World Heart J. 2010;2(3):177–96 [Google Scholar]
- 17.Fiser B, Havelkova A, Siegelova J, et al. Night-to-day blood pressure ratio during seven-day ambulatory blood pressure monitoring. Noninvasive Methods in Cardiology; 2010September16-17; Brno, Czech Republic [Google Scholar]
- 18.Siegelova J, Havelkova A, Fiser B, et al. Day and night blood pressure variability during seven-day ambulatory blood pressure monitoring. Noninvasive Methods in Cardiology; 2010September16-17; Brno, Czech Republic [Google Scholar]
- 19.Otsuka K, Cornélissen G, Halberg F. Predictive value of blood pressure dipping and swinging with regard to vascular disease risk. Clin Drug Invest. 1996;11(1):20–31 [Google Scholar]
- 20.Janeway TC. The clinical study of blood pressure. New York: D. Appleton & Co; 1904 [Google Scholar]
- 21.Zadek I. Die Messung des Blutdrucks am Menschen mittelst des Basch'chen Apparates [medical dissertation]. Berlin: Schumacher; 1880 [Google Scholar]
- 22.Zadek I. Die Messung des Blutdrucks am Menschen mittelst des Basch'chen Apparates. Z klin Med. 1881;2:509–51 [Google Scholar]
- 23.Bartter FC. Periodicity and medicine. In: Scheving LE, Halberg F, Pauly JE, editors. Chronobiology. Tokyo: Igaku Shoin Ltd; 1974. p. 6–13 [Google Scholar]
- 24.Halberg F, Cornélissen G, Halberg E, et al. Chronobiology of human blood pressure. Medtronic continuing medical education seminars. 4th ed Minneapolis: Medtronic Inc; 1988 [Google Scholar]
- 25.Cornélissen G, Halberg F, Gubin D, et al. Carpe diem mensuratem: Fulminant CHAT, its recognition a chronobiologic path to preventing a myocardial infarction? Abstract, 4° Convegno Nazionale, Società Italiana di Cronobiologia, Gubbio; 1996June1-2; Perugia, Italy [Google Scholar]
- 26.Hillman DC, Cornélissen G, Scarpelli PT, et al. ; International Womb-to-Tomb Chronome Initiative Group Chronome maps of blood pressure and heart rate. University of Minnesota/Medtronic chronobiology seminar series #2; 1991December [Google Scholar]
- 27.Halberg F, Cornélissen G, Otsuka K, et al. Rewards in practice from ‘recycling’ heart rate, ectopy, ischemia and blood pressure information. J Med Eng Technol. 1997Sep-Oct;21(5):174–84 [DOI] [PubMed] [Google Scholar]
- 28.Halberg F, Hillman D, Cornélissen G, et al. Putative solar signatures can differ among variables and circadian endpoints and in individuals vs populations. International Congress: Natural Cataclysms and Global Problems of the Modern Civilization; 2011 September 19-21; Istanbul, Turkey [Google Scholar]
- 29.Watanabe Y, Cornélissen G, Hillman D, Otsuka K, Halberg F. Long periods in 23 years of around-the-clock automatic measurements of human blood pressure and pulse. International Congress: Natural Cataclysms and Global Problems of the Modern Civilization; 2011 September 19-21; Istanbul, Turkey [Google Scholar]
- 30.Halberg F, Cornélissen G, Schwartzkopff O, et al. Preventive cardiology concerns avoidance of personal and societal health-related and natural cataclysms. Noninvasive Methods in Cardiology; 2011October17; Brno, Czech Republic [Google Scholar]
- 31.Feinleib M, Rogot E, Sturrock PA. Solar activity and mortality in the United States. Int J Epidemiol. 1975September;4(3):227–9 [DOI] [PubMed] [Google Scholar]
- 32.Lipa BJ, Sturrock PA, Rogot E. Search for correlation between geomagnetic disturbances and mortality. Nature. 1976January29;259(5541):302–4 [DOI] [PubMed] [Google Scholar]
- 33.Halberg F, Bakken EE, Katinas GS, et al. Chronoastrobiology: Vernadsky's future science? Benefits from spectra of circadians and promise of a new transdisciplinary spectrum of near-matching cycles in and around us. International Conference: Civilization Diseases in the Spirit of V.I. Vernadsky; 2005 October 10-12; People's Friendship University of Russia, Moscow [Google Scholar]
- 34.Halberg F, Cornélissen G, McCraty R, al-Abdulgader A. Time structures (chronomes) of the blood circulation, populations' health, human affairs and space weather. World Heart J. 2011;3(1):73–114 [Google Scholar]
- 35.Vallot J, Sardou G, Faure M. De l'influence des taches solaires: sur les accidents aigus des maladies chroniques. Gazette des Hôpitaux. 1922;904–5 [Google Scholar]
- 36.Schwartzkopff O, Halberg F, Katinas G, et al. Strain tests: gauging variability in a day, week, year or decade. 59th Annual Meeting, Japan Society of Neurovegetative Research; 2006 November 1-3; Tokyo, Japan [Google Scholar]
- 37.Cornélissen G, Halberg F, Otsuka K, Singh RB, Chen CH. Chronobiology predicts actual and proxy outcomes when dipping fails. Hypertension. 2007January;49(1):237–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gupta AK, Greenway FL, Cornélissen G, Pan W, Halberg F. Prediabetes is associated with abnormal circadian blood pressure variability. J Human Hypertension. 2008September;22(9):627–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cornélissen G, Halberg F, Beaty L, et al. Cugini's syndrome in statu nascendi. Oratio contra morem prevalentem et pro chronobiologica ratione ad pressione sanguinis curandam. A plea against the prevailing custom and in favor of a chronobiological approach to treating blood pressure. Clin Ter. 2009;160(2):e13–24 [PubMed] [Google Scholar]
- 40.Müller-Bohn T, Cornélissen G, Halhuber M, Schwartzkopff O, Halberg F. CHAT und Schlaganfall. Deutsche Apotheker Zeitung. 2002January24;142:366–70 [Google Scholar]
- 41.Müller-Bohn T, Cornelissen G, Halberg F, Halhuber M, Delea CS. Blood pressure variability gauged by circadian overswing (CHAT) and lifespan. Time Series (not spotcheck) 1st International Workshop of the TsimTsoum Institute: Evidence-based Holistic Approach to Health; 2010 June 3; Krakow, Poland [Google Scholar]
- 42.Zaslavskaya RM. Chronodiagnosis and chronotherapy of cardiovascular diseases. 2nd ed Moscow: Medicina; 1993. In English [Google Scholar]
- 43.Güllner HG, Bartter FC, Halberg F. Timing antihypertensive medication. Lancet. 1979September8;2(8141):527. [DOI] [PubMed] [Google Scholar]
- 44.Halberg F, Cornélissen G, Katinas G, et al. ; International BIOCOS Group Chronobiology's progress: season's appreciations 2004-2005. Time, frequency, phase, variable, individual, age- and site-specific chronomics. J Appl Biomed 2006;4:1–38 [Google Scholar]
- 45.Watanabe Y, Cornélissen G, Halberg F, et al. Harm vs. benefit from losartan with hydrochlorothiazide at different circadian times in MESOR-hypertension or CHAT. Noninvasive Methods in Cardiology; 2008October4-7; Brno, Czech Republic [Google Scholar]
- 46.Halberg F, Cornélissen G, Wilson D, et al. Chronobiology and chronomics: detecting and applying the cycles of nature. Biologist (London). 2009;56(4):209–14 [PMC free article] [PubMed] [Google Scholar]
- 47.Watanabe Y, Halberg F, Otsuka K, Cornelissen G. Physiological changes in relation to the 2011 East Japan earthquake. International Congress: Natural Cataclysms and Global Problems of the Modern Civilization; 2011 September 19-21; Istanbul, Turkey [Google Scholar]
- 48.Satoh M, Kikuya M, Ohkubo T, Imai Y. Acute and subacute effects of the great East Japan earthquake on home blood pressure values. Hypertension. 2011December;58(6):e193–4 [DOI] [PubMed] [Google Scholar]
- 49.Vernadsky VI. Some words about the noösphere. 21st Century Sci Technol. 2005; Spring:16–21 [Google Scholar]
- 50.Bailes KE. Science and Russian culture in an age of revolutions: V.I. Vernadsky and his scientific school, 1863-1945. Bloomington/Indianapolis: Indiana University Press; 1990 [Google Scholar]
- 51.Halberg F, Cornélissen G, Sothern RB, Katinas GS, Schwartzkopff O, Otsuka K. Cycles tipping the scale between death and survival (=“life”). Progr Theor Phys Suppl. 2008;Suppl 173:153–81 [Google Scholar]
- 52.Halberg F, Cornélissen G, Schack B, et al. Blood pressure self-surveillance for health also reflects 1.3-year Richardson solar wind variation: spin-off from chronomics. Biomed Pharmacother. 2003October;57Suppl 1:58s–76s [DOI] [PubMed] [Google Scholar]
- 53.Halberg F, Cornélissen G, Regal P, et al. Chronoastrobiology: proposal, nine conferences, heliogeomagnetics, transyears, near-weeks, near-decades, phylogenetic and ontogenetic memories. Biomed Pharmacother. 2004October;58Suppl 1:S150–87 [DOI] [PubMed] [Google Scholar]
- 54.Halberg F, Breus TK, Cornélissen G, et al. ; International Womb-to-Tomb Chronome Initiative Group Chronobiology in space. 37th Annual Meeting Japan Society for Aerospace and Environmental Medicine; 1991 November 8-9; Nagoya, Japan [Google Scholar]
- 55.Mikulecký M. Paroxysmal tachyarrhythmia and moon. Chronobiologia. 1990Jan-Mar;17(1):71–3 [PubMed] [Google Scholar]
- 56.Mikulecky M, editor. Sun, moon and living matter. Bratislava, Slovakia. Bratislava: Slovak Medical Society; 1994 [Google Scholar]
- 57.Mikulecky M, editor. Chronobiology and its roots in the cosmos. High Tatras; 1997September2-6; Bratislava, Slovakia [Google Scholar]
- 58.Mikulecky M, Florida PL. Daily birth numbers in Davao, Philippines, 1993-2003: Halberg's transyear stronger than year. 26th Seminar: Man in His Terrestrial and Cosmic Environment; 2005 May 17-19; Upice, Czech Republic [Google Scholar]
- 59.Kovac M, Mikulecky M. Secular rhythms and Halberg's paraseasonality in the time occurrence of cerebral stroke. Bratisl Lek Listy. 2005;106(2):423–7 [PubMed] [Google Scholar]
- 60.Kovac M, Mikulecky M. Time sequence of epileptic attacks from the point of view of possible lunisolar connections. International Conference on the Frontiers of Biomedical Science: Chronobiology; 2006 September 24-26; Chengdu, China [Google Scholar]
- 61.Doodson AT. The harmonic development of the tide-generating potential. Proc Roy Soc Lond A. 1921;100(704):305–29 [Google Scholar]
- 62.Halberg F, Cornélissen G, Hillman D, et al. Multiple circadian periods in a lady with recurring episodes of adynamic depression: case report. Noninvasive Methods in Cardiology; 2011October17; Brno, Czech Republic [Google Scholar]
- 63.Evstafyev VK. How solar activity influences earth's molecular processes. Open Biol J. 2009;2:38–41 [Google Scholar]
- 64.Freund F. Toward a unified solid-state theory for pre-earthquake signals. Acta Geophys. 2010;58(5):719–66 [Google Scholar]
- 65.Stinson SM, Cornélissen G, Scarpelli PT, Halberg F. Self-measurement and ambulatory monitoring of blood pressure: a subject's chronobiological perspective. Biomed Pharmacother. 2002;56Suppl 2:333s–8s [DOI] [PubMed] [Google Scholar]
- 66.Hillman DC, Siffre M, Milano G, Halberg F. Free-running psycho-physiologic circadians and three-month pattern in a woman isolated in a cave. New Trends Exp Clin Psychiatry. 1994;10:127–33 [Google Scholar]
- 67.Hillman DC. Physiologic 7- and 3.5-day patterns in health and disease revealed by free-run and single-stimulus induction. Doctoral Thesis, May1993 [Google Scholar]
- 68.Halberg F, Cornélissen G, Bingham C, et al. Chronomics: imaging in time by phase synchronization reveals wide spectral-biospheric resonances beyond short rhythms. Neuro Endocrinol Lett. 2003October;24(5):355–80 [PubMed] [Google Scholar]
- 69.Cornélissen G, Bakken EE, Sonkowsky RP, Halberg F. A 38-million-year cycle among myriadennians in the diversity of oceanic genera. International Conference: Civilization Diseases in the Spirit of V.I. Vernadsky; 2005 October 10-12; People's Friendship University of Russia, Moscow [Google Scholar]
- 70.Sonkowsky RP, Cornélissen G, Chibisov SM, Schwartzkopff O, Sampson M, Halberg F. Myriadennian, including perhaps millionennian or the shorter megennian—a choice to be made: invitation for comment. International Conference: Civilization Diseases in the Spirit of V.I. Vernadsky; 2005 October 10-12; People's Friendship University of Russia, Moscow [Google Scholar]
- 71.Halberg F, Cornélissen G, Katinas G, et al. Transdisciplinary unifying implications of circadian findings in the 1950s. J Circadian Rhythms. 2003October29;1(1):2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Cornélissen G, Halberg F, Gheonjian L, et al. Schwabe's ∼10.5- and Hale's ∼21-year cycles in human pathology and physiology. In: Schröder W, editor. Long-and short-term variability in sun's history and global change. Bremen: Science Edition; 2000. p. 79–88 [Google Scholar]
- 73.Hrushesky WJ, Sothern RB, Du-Quiton J, Quiton DF, Rietveld W, Boon ME. Sunspot dynamics are reflected in human physiology and pathophysiology. Astrobiology. 2011March;11(2):93–103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Sello S, Halberg F, Cornélissen G. Human babies: a slow-to-read, sensitive population magnetometer, also read by wavelets. Noninvasive Methods in Cardiology; 2011October17; Brno, Czech Republic [Google Scholar]
- 75.Cornélissen G, Halberg F, Wendt HW, et al. Resonance of about-weekly human heart rate rhythm with solar activity change. Biologia (Bratisl). 1996December;51(6):749–56 [PubMed] [Google Scholar]
- 76.McCraty R, Deyhle A, Childre D. The Global Coherence Initiative: creating a coherent planetary standing wave. Global Adv Health Med. 2012;1(1):62–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.McCraty R, Childre D. Coherence: bridging personal, social, and global health. Altern Ther Health Med. Jul-Aug 2010;16(4):10–24 [PubMed] [Google Scholar]
- 78.Persinger MA. On the possible representation of the electromagnetic equivalents of all human memory within the Earth's magnetic field: implications for theoretical biology. Theoret Biol Insights. 30September2008;1:3–11 [Google Scholar]
- 79.Persinger MA, Koren SA, Lafreniere GF. A neuroquantologic approach to how human thought might affect the universe. Neuroquantology. 2008;6(3):262–71 [Google Scholar]
- 80.Wendt HW. Interplanetary magnetic field (IMF) polarity, collective emotions and entropy changes of random event generators. 8th International Congress: Health and Education Millennium; 2007 November 14-17; Moscow, Russia [Google Scholar]
- 81.Ulmer W, Cornélissen G, Halberg F. Physical chemistry and the biologic week in the perspective of chrono-oncology. In Vivo. 1995Jul-Aug;9(4):363–74 [PubMed] [Google Scholar]
- 82.Tchijevsky AL. de Smitt VP, translator. Physical factors of the historical process. Cycles. 1971January22:11–27 [Google Scholar]
- 83.Sigel F, Dreier W. Schuld ist die Sonne. Frankfurt am Main: Deutsch Harri GmbH; 1979 [Google Scholar]
- 84.Dubrov AP. Sinclair FL, translator. The geomagnetic field and life: geomagneto-biology. New York: Plenum Press; 1978 [Google Scholar]
- 85.Brown FA., Jr A unified theory for biological rhythms. In: Aschoff J, editor. Biological clocks. Amsterdam: North-Holland Publishing Co; 1965. p. 231–61 [Google Scholar]
- 86.Wever RA. The circadian system of man: results of experiments under temporal isolation. New York: Springer-Verlag; 1979 [Google Scholar]
- 87.Chibisov SM, Cornélissen G, Halberg F. Magnetic storm effect on the circulation of rabbits. Biomed Pharmacother. 2004October;58Suppl 1:S15–9 [DOI] [PubMed] [Google Scholar]
- 88.Breus TK, Cornélissen G, Halberg F, Levitin AE. Temporal associations of life with solar and geophysical activity. Ann Geophys. 1995;13:1211–22 [Google Scholar]
- 89.Breus TK, Chibisov SM, Baevsky RM, Schebzuhov KV. The chronostructure of heart biorhythms under effects of external environment factors. Moscow: Russian University of People's Friendship, Polygraph Service; 2002 [Google Scholar]
- 90.Düll B, Düll T. Erd- und Sonnenphysikalische Vorgänge in ihrer Bedeutung für Krankheits- und Todauslosung. Nosokomeion. 1938;9:103–20 [Google Scholar]
- 91.Stetson HT. Sunspots in action. New York: Ronald Press Co; 1947 [Google Scholar]
- 92.Beaty L, Cornélissen G. Towards inexpensive ambulatory blood pressure variability monitors for home use: a first experiment using off-the-shelf devices as the basis for ABPMs. 2008. www.phoenix.tcieee.org/0001_Bibliography/20081221beat_FirstHomemadeABPM.pdf Accessed April 4, 2012