

Summary
Aim To determine the epidemiology and clinical presentation, and any contributing factors responsible for burns and outcome of care in Kuwait over the 5-yr period January 2006 to December 2010. Patients and methods. The study reviewed 1702 burn patients admitted over the study period to the Saud Al Babtain Burns, Plastic and Reconstructive Surgery Center, Kuwait. Patient characteristics, including age, sex, type of burn, nationality, total body surface area (TBSA) burn, hospital stay in days, and mortality were recorded. Results. Seventy-one per cent of the 1702 burn patients admitted were males; 540 were children. The majority of patients (64%) had less than 15% TBSA burns and only 14% had more than 50% TBSA burns. Flame burns were the most common cause of burn injuries (60%), followed by scalds (29%). Scalds were most common in children. The mortality rate was 5.75%. Flame burn was the leading cause of mortality. Lethal dose 50 (% TBSA at which a certain group has a 50% chance of survival) for adults (16-40 yr) and for the elderly (>65 yr) was 76.5% and 41.8% TBSA respectively. Conclusion. Burn injury is an important public health concern and is associated with high morbidity and mortality. Flame and scald burns are commonly a result of domestic and occupational accidents and they are preventable. Effective initial resuscitation, infection control, and adequate surgical treatment improve outcomes.
Keywords: epidemiology of burns, burns in Kuwait, paediatric burns in Kuwait, LD50 for burns in Kuwait
Abstract
Objectif. Déterminer l’épidémiologie et décrire la présentation clinique et les éventuels facteurs responsables des brûlures et des résultats des soins au Koweït au cours des dernières cinq années. Patients et méthodes. Un nombre total de 1702 patients brûlés hospitalisés dans le Centre de Chirurgie Plastique et Reconstructive Saud Al Babtain au Koweït Center entre janvier 2006 et décembre 2010 ont été pris en considération. Les caractéristiques des patients (âge, sexe, type de brûlure, nationalité, surface corporelle totale (SCT) brûlée, journées de séjour à l’hôpital, mortalité) ont été enregistrées. Résultats. Soixante-et-un pour cent des 1702 patients brûlés hospitalisés étaient des hommes; 540 patients étaient des enfants. La majorité des patients (64%) avaient des brûlures en moins de 15% de la SCT et seulement 14% avaient plus de 50%. Les flammes étaient la cause la plus commune des brûlures (60%), suivies par les brûlures (29%). Les ébouillantements étaient plus fréquents chez les enfants. Le taux de mortalité était de 5,75%. Les brûlures dues aux flammes étaient la principale cause de la mortalité. La dose létale 50 pour les adultes (16-40 ans) et pour les personnes âgées (> 65 ans) était respectivement de 76,5 et de 41,8% SCT. Conclusion. La brûlures constitue un important problème de santé publique et est associée à une morbidité et une mortalité élevée. Les brûlures dues aux flammes et aux ébouillantements sont souvent provoquées par des accidents domestiques. Pour améliorer les résultats il faut avoir une réanimation initiale efficace, un bon contrôle de l’infection et un traitement chirurgical adéquat.
Introduction
Burn injuries are one of the leading causes of morbidity and mortality in the Middle-East1 representing 5-12% of all traumas.2
The incidence of burns ranges from 112 to 518 per 100,000 per yr across all ages.3-9 A much higher incidence of 1,388 per 100,000 per yr is reported amongst children below 5 yr in a study from Pakistan,9 while in Kuwait a study published in 2006 reported an incidence of 34 per 100,000 per yr in children aged 0-4.10
Most burn incidents occur in domestic settings because of defective household appliances, flammable agents in the home, clothing burns, and in some cases self-inflicted injuries.11-12 The majority of burn injuries sustained by children occur at home as the result of an accident,12 thus most of these injuries are preventable. All cases require some degree of medical attention and many patients suffer morbidity or even die.1 People affected are mostly of poor socioeconomic status and of employable age. Life styles and social factors contribute to the high occurrence of burns at home.
The Saud Al Babtain Center, Ibn Sina Hospital, part of the Ministry of Health, is the only tertiary level of care unit specialized in burn management in the State of Kuwait, so our catchment is area covers the whole country’s population (approx. 3.7 million).
The American Burn Association criteria (Table I) for referral to a burn centre are the guidelines followed in our policy of admissions and referral at the Saud Al Babtain Center.13
Table I. American Burn Association burn centre referral criteria.

This study was undertaken to describe the epidemiology, clinical presentation, and outcome in burn patients in our setup and also to identify contributing factors influencing the outcome in burn patients.
Patients and methods
This prospective study was carried out at the Saud Al Babtain Center, from January 2006 to December 2010. Consecutive patients with different types of burn injuries requiring admission were included in the study. Patients with only minor superficial burns treated as out-patients by the Emergency Department were not included. Data were collected using a data sheet including file number, age (children were classed as being 16 yr old or below, adults above 16), nationality, gender, burn type, percentage of TBSA burned, and outcome. The history regarding the aetiology of the burn injury was taken directly and confidentially from patients or from their relatives. Percentage of burn was determined by using the Lund and Browder Chart. On admission to the ward or the Intensive Care Burn Unit (ICBU) the patient received initial resuscitation including burn wound cleansing, airway maintenance (if needed), intravenous fluids (Ringer Lactate) according to Parkland’s formula; moreover, pain relief and Ranitidine were given to all patients. After taking emergency measures, regular wound debridement and dressings were performed. Patients were monitored for pulse, blood pressure, respiratory rate, temperature charts, and urine output. Wound healing was assessed clinically as well as improvement in overall condition. Central venous lines were employed in a few cases. Definitive treatment of the burn wound included skin grafts, Integra® application or, in very rare cases, amputation.
Results
Incidence
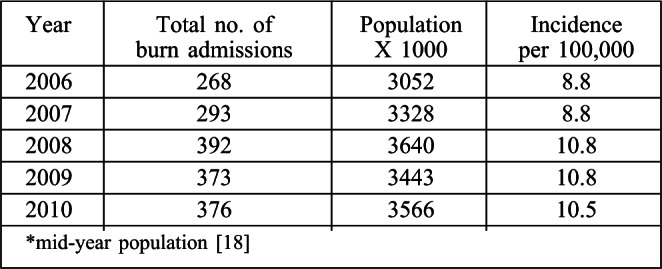
The total incidence of burn injuries requiring hospital admissions in the State of Kuwait is illustrated in Table II. In the five years, the incidence of burn injuries requiring admission was an average of 9.9 per 100,000. The highest incidence was recorded in 2008 and 2009 (10.8 per 100,000) while years 2006 and 2007 recorded the lowest incidence rate (8.8 per 100,000) of burns requiring admission.
Table II. Total incidence of burn cases requiring admission.
The incidence of burn injuries in the state of Kuwait among nationals and non-nationals is illustrated in Table III. The incidence of burn injuries requiring admission amongst nationals ranged from 7.4 per 100,000 in 2006 to 11.8 per 100,000 in 2008, with an average of 9.3 per 100,000. Regarding non-nationals suffering burn injuries, the average incidence was 10.2 per 100,000.
Table III. Incidence of burn injuries requiring admissions by nationality.

In the study period, the average incidence of burns amongst females was lower than amongst males, with an average of 7.4 per 100,000. The highest incidence of female burn cases was reported in 2009 (9 per 100,000), with an over 20% increase compared to average that is attributed to the Jahra mass incident (Table IV).
Table IV. Incidence of burn injuries requiring admissions according to gender.

Using the annual reports regarding age groups issued by the Ministry of Health in the State of Kuwait (Department of Statistics and Information) from 2006 to 2010, we calculated the incidence of burns in children from 0 to 14 yr of age (Table V). The average incidence of burns, from 2006 to 2010, in this group of children was 14.6 per 100,000.
Table V. Incidence of burns in children 0-14 years.

Age
The percentage of paediatric burns remained between 30% and 36% of the total burn cases admitted in the period.
Burn cases in both adults (>16 yr of age) and children (≤16 yr) steadily increased in number from 2006 to 2008, coupled with a reduction in bed capacity due to renovations starting in March 2009, with a slightly negative effect on the number of admissions in 2009 and 2010.
The total number of adults admitted from January 2006 to December 2010 was 1162 (68.3%), while the total number of children was 540 (31.7%). The highest number of adult patients (269 cases) admitted due to burns was recorded in 2008, while in the children’s group the highest number of burn admissions (133 cases) occurred in 2009 (Fig 1 and Table VI).
Fig. 1. Burn admissions according to age.

Table VI. Number of admitted cases according to age.

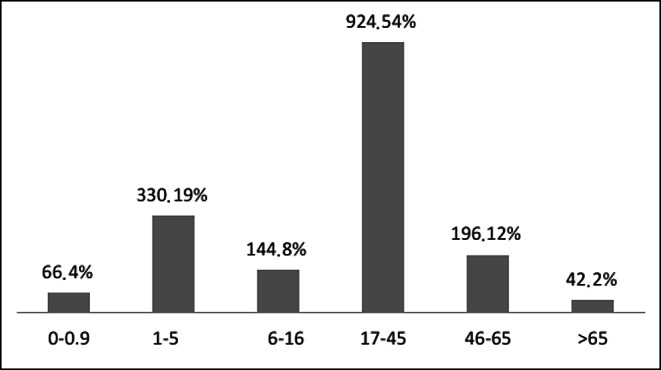
Data in Table VII and Fig 2 show that children (from 1 to 5 yr) and young adults (17-45 yr) were the most common age groups presenting with burns, respectively accounting for 19% and 54% of total patient admissions from 2006 to 2010.
Table VII. Age groups (total number of cases from 2006 to 2010).

Fig. 2. Number and percentage of patients of different age groups.
Gender
The number of male burn patients increased from 184 cases in 2006 to 288 in 2008, while in 2009 and 2010 the number of cases decreased to 255 and 269 respectively (Table VIII).
Table VIII. Number and percentage of admissions according to gender.
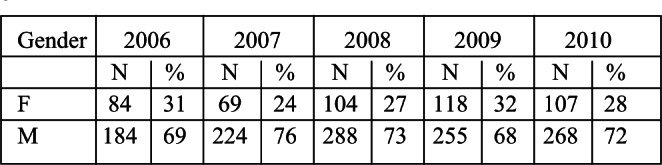
Fig. 3 shows the percentage of females and males in each year, with females representing 28.3% of all admissions (482 cases).
Fig. 3. Distribution of patients by gender.
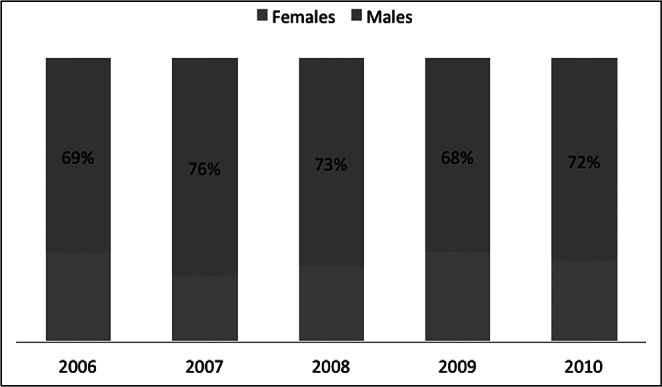
In 2009 we recorded the highest number of female burn cases admitted to our centre (118 cases). Forty-two females, i.e. 36% of total female admissions that year, were admitted in one month (August 2009) following a major fire incident (the Jahra fire incident).
Causes, site, and depth of burns
Flame burn was the leading cause of burns, representing 60% of all causes, followed by scalds (29% of all causes). From 2006 to 2010, burns due to electric current, chemicals, or contact with hot objects represented only 11% of cases (Table IX).
Table IX. Causes of burn injuries.

Interestingly, burn admissions due to flame steadily increased in the five years, with a concomitant decrease in burns due to scald (Fig. 4)
Fig. 4. Annual percentage of flame burns and scalds.

Flame and electric burns are most commonly seen in non-nationals, adults, and males. Almost 76% of adult admissions were due to flame burns. Scald burns represented almost 62% of all burn cases in children 16 yr and below (mean age, 13 yr) (Table X).
Table X. Causes of burn according to nationality, gender and age.

The face and hands were involved in almost 88% of the cases admitted since 2006 (Table XI).
Table XI. Number and percentage of facial and hand burns.

The recorded incidence of inhalational lung injury associated with flame burns has increased dramatically since 2006, as shown in Table XII (from 0.7% of total flame burn cases in 2006 to 17% in 2010). This may be either a false increase due to more detailed documentation and improved diagnostic techniques or to overzealous diagnosis, or it may be considered a true increase - or a bit of both.
Table XII. Inhalational burn injury.

Percentage of total body surface area burned (% TBSA)
Severe burns (above 30% TBSA) were most commonly seen amongst non-nationals, males and adults (78.6%, 69.8%, and 86.7% respectively), and in 91.1% of cases they were due to flame.
Only 1.5% of children admitted presented more than 50% TBSA (8 cases) (Fig. 6).
Fig. 6. Percentage adults and children burned.

As shown in Table XIII, the majority of the burns treated (64.1%) were considered minor, i.e. affecting less than 15% TBSA. This is followed by cases of moderate burns with 16% to 30% TBSA (21.3%). Patients with severe burns (30% TBSA and above) represented 14.6% of cases (Fig. 5).
Table XIII. Percentage TBSA according to year, gender, nationality, type of burn and age.

Fig. 5. Percentage TBSA burned.

Surgery
On average, 55% of patients admitted required surgery in the form of excision and split-thickness skin grafts. Some patients, especially those with a high TBSA percentage, were operated on two or more times. Table XIV shows the number of burn patients with deep burns requiring excision and split-thickness skin grafts every year.
Table XIV. Number and percentage of patients requiring surgery (deep burns).

Mortality
Throughout the study period, the average mortality rate in our centre was 5.76% of all admissions, i.e. 0.58 per 100,000 per yr. The mortality rate was found to correlate closely to the number of burn cases admitted with over 50% TBSA burns. Mortality in the group of patients under 16 yr of age represented 14.3% of the total mortality recorded. The average mortality rate in this group from 2006 to 2010 was 2.4% (Table XV).
Table XV. Mortality among age groups.

Flame burn was the leading cause of mortality (88.8%). Other causes are shown Table XVI.
Table XVI. Burn causes and mortality.

Using logistic regression, mortality, age, and % TBSA were plotted against each other in a graph to extract the Lethal Dose 50 (LD50) for each age group (Fig. 7). LD50 is defined as the % TBSA at which a certain group has a 50% chance of survival. The LD50 for each age group is shown in Table XVII.
Fig. 7. Mortality age and % TBSA plotted to show Lethal Dose 50.

Table XVII. LD50 by age.

Hospital stay
Total hospital days (total number of hospitalization days by all patients in a certain period) more than halved in the five years under investigation, falling from 6860 days in 2006 to 3128 days in 2010, with an almost 55% decrease. This may indicate better surgical practices and a decrease in the number of days of unnecessary hospital stay. In the same context, the average length of hospital stay (the average number of hospitalization days by a patient in a certain period) decreased from 19 days in 2006 to 8 days in 2010.
The capacity of beds assigned for burn case admissions was 46 beds from 2006 to 2008. In 2009 and 2010 bed capacity was reduced to 32 beds, effective from March 2009, due to renovation works.
The average bed occupancy rate remained around 60% in the 5-yr period, reaching up to 100% and 90% in some months of 2009 and 2010 respectively. These high bed occupancy rates increase the risk of hospital-acquired infection among patients and staff,14 and also have a significant and quantifiable negative influence throughout on the emergency department throughout, affecting both discharged and hospitalized patients.15
The bed turnover rate (BTR), i.e. the number of times a single bed is used in a given period of time, increased from 13 in 2006 to 20 in 2010, corresponding to a 35% increase in BTR over the five years. This indicates a higher flow of patients, as evidenced by the higher turnover of beds (Table XVIII).
Table XVIII. Hospital bed utilization indices.

Discussion
Incidence and demography
Considering the fact that the Saud Al Babtain Plastic and Burn Surgery Center is the only specialized centre dealing with burn injuries in the State of Kuwait, and that it accepts referrals of burn injuries from all Kuwait health services (e.g. primary care centres, government hospitals, private sector), it is fair to correlate the admissions of burn cases with the incidence of burn injuries requiring hospital care in the State of Kuwait. Although it might not provide an accurate representation of the real total incidence rate of burn injuries (i.e. burn cases treated at home, in the primary care setting, in the general hospital setting, or burns treated on an out-patient basis), it most likely represents the rate of burns requiring admissions, as almost all burn injuries requiring any level of hospital care are referred to us.
In the Middle East, the annual incidence of burns requiring hospital admissions for all age groups ranges from 112 to 518 per 100,000.1
According to the National Burn Repository, in the US there were 126,000 hospital admissions for burns from 1995 to 2005, with an average overall incidence of 7 per 100,000 per yr.13
The average overall incidence of burns requiring hospital admissions in Kuwait from 2006 to 2010 was 9.9 per 100,000 per yr.
In a study conducted in Kuwait from 1993 to 2001, the overall incidence rate for paediatric patients in the 0-14 age group was 17.5 per 100,00017 while our study showed a 2.9 per 100,000 (16.6%) decrease in the overall incidence of burns in the age group 0-14 between 2006 and 2010 (14.6 per 100,000).
In our study the incidence of female burn admissions was 10.4 per 100,000, compared to 13.4 per 100,000 reported by other studies1 in the same region.
Contrary to many studies in our region of the world, the incidence of burn injuries among males was higher than among females.3-9
The fact that in the state of Kuwait the number of nonnationals is almost 1.5 times18 as much as the population of nationals, plus the fact that most non-skilled occupations are performed by non-nationals (which makes them more vulnerable to burn injuries), explains the higher incidence rate of burn cases requiring admissions amongst non-nationals.
The exceptionally higher than average incidence of female burn admissions in 2009 is explained by the Jahra mass fire incident (when an arsonist set ablaze a wedding tent trapping almost a hundred women inside).
In 23 studies conducted in Egypt, Oman, Saudi Arabia, Afghanistan, Pakistan, and Iran from 1997 to 2005, the median percentage of males of all ages with burn injuries was 51%, while in our study of the burn admissions total, the average percentage of males was 71.3%. The female median percentage, which was 49% in former studies, was only 28.7% in our study. These significant results may be explained by the high standard of living of most females in Kuwait; moreover, most burn injuries happen at work, not at home.19-34
Causes
The majority of cases admitted to our centre in the five years under investigation were due to flame burns (60%) and scalds (29%). Other causes of burns represented about 11% of total burn admissions. Similar results were found in many studies conducted in the same region of the world between 1997 and 2006.5-8,20-24,35
Most studies report that scalds are more common than flame injuries amongst children.1,17 Other studies, such as that conducted in the US between 1990 and 2006, showed that thermal burns were more common (59.5%) in children than scalds.36 As reported in many studies,13 the face and hands are most commonly affected in burns (88%).
Percent TBSA
In the Middle East region the mean TBSA burned in all ages was found to range from 10 to 48%,1 while in the US and Canada13 62% of all patients had less than 10% TBSA affected. Our results were consistent with the results obtained from the US and Canada, as 64% of burns admitted to our centre involved 15% or less TBSA.
Mortality and hospital stay
The World Health Organization37 classifies burn injury as the third most important cause of mortality among children. The mortality rate due to fire-related burns per 100,000 children, in the high income countries (HIC) in the Eastern Mediterranean region, is 0.4 per 100,000 per yr. In our study the mortality rate in children less than 14 yr of age from 2006 to 2010 was 0.3 per 100,000 per yr. In a similar study conducted in Kuwait in 200610 the child mortality rate was 1.3% of all children admitted, surprisingly the same percentage as was found in our study.
With regard to all age groups, in our study the average mortality rate was 0.58 per 100,000 per yr, i.e. 5.74% of admissions. In several studies conducted in Egypt,20 Kuwait,32 Iran,7 and Pakistan,25 the percentage mortality was higher: 33%, 6.4%, 18.7%, and 30%, respectively. This indicates higher standards of care, which rewards the State of Kuwait as being a HIC by the WHO.
In 1997, the average length of hospital stay (ALOS) in Kuwait32 was 16 days, while in our study, ALOS had decreased to 8 days - this also indicating better surgical practices.
In the USA in 2005, according to the National Burn Repository, the mortality rate was 4.67% and the ALOS was 8.22.38
The LD50 in young children (0-5 yr) was 25% TBSA: this is still low and further work is needed to improve our outcome. Compared to the figures from the US for 2002, the LD50 of the elderly (>70 yr) was 30% TBSA39-40 while in our study the LD50 for the elderly (>65 yr) was 41.8%.
The results in the study showed that the outcome measured by the LD50 in the 6-15 yr age group was well behind that reported by renowned burn centres. On the other hand, the LD50 for adults (16-40 yr) was somewhat closer to western world standards.
Conclusion
Burn injuries are an important public health issue in the East Mediterranean region, being one of the leading causes of morbidity and mortality. Our study shows that the epidemiology, pattern, and causes of burns have been almost similar throughout the past decade in Kuwait, except for minor changes. Moreover, most of these numbers are consistent with high income countries in the world. This may be a good indicator that burns, burn management, and outcome of care are closely related to the standard of living of the society, and that burns can be prevented and controlled by multi-disciplinary approaches within the whole society, by raising awareness at home, at the workplace, with fire-fighters, and with hospitals. Effectiveness of burn management is best measured by the LD50, and in our centre the LD50 of children needs attention and improvement. This study can be used as a guideline for devising future national health strategic plans for burns management, including public awareness programmes, the building of hospitals, and the allocation of intensive care unit beds to burn patients.
References
- 1.Othman N, Kendrick D. Epidemiology of burn injuries in the East Mediterranean Region: A systematic review. BMC Public Health. 2010;10:83. doi: 10.1186/1471-2458-10-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Olaitan PB, Olaitan JO. Burns and scalds - epidemiology and prevention in a developing country. Niger J Med. 2005;14:9–16. doi: 10.4314/njm.v14i1.37128. [DOI] [PubMed] [Google Scholar]
- 3.Groohi B, Rossignol AM, Barrero SP, et al. Suicidal behavior by burns among adolescents in Kurdistan, Iran: A social tragedy. Crisis. 2006;27:16–21. doi: 10.1027/0227-5910.27.1.16. [DOI] [PubMed] [Google Scholar]
- 4.Arshi S, Sadeghi-Bazargani H, Mohammadi R, et al. Prevention oriented epidemiologic study of accidental burns in rural areas of Ardabil, Iran. Burns. 2006;32:366–71. doi: 10.1016/j.burns.2005.10.026. [DOI] [PubMed] [Google Scholar]
- 5.Groohi B, Alaghehbandan R, Lari AR. Analysis of 1089 burn patients in the province of Kurdistan, Iran. Burns. 2002;28:569–74. doi: 10.1016/s0305-4179(02)00099-2. [DOI] [PubMed] [Google Scholar]
- 6.Panjeshahin MR, Lari AR, Talei A, et al. Epidemiology and mortality of burns in the South West of Iran. Burns. 2001;27:219–26. doi: 10.1016/s0305-4179(00)00106-6. [DOI] [PubMed] [Google Scholar]
- 7.Maghsoudi H, Pourzand A, Azarmir G. Aetiology and outcome of burns in Tabriz, Iran. An analysis of 2963 cases. Scand J Surg. 2005;94:77–81. doi: 10.1177/145749690509400118. [DOI] [PubMed] [Google Scholar]
- 8.Siddiqui NA. Burn injury is preventable: An analysis of 716 cases in a burns unit. J College of Physicians & Surgeons Pakistan. 1998;8:148–52. [Google Scholar]
- 9.Ahmed M, Shah M, Luby S, et al. Survey of surgical emergencies in a rural population in the northern Areas of Pakistan. Trop Med Int Health. 1999;4:846–57. doi: 10.1046/j.1365-3156.1999.00490.x. [DOI] [PubMed] [Google Scholar]
- 10.Sharma PN, Bang RL, Al-Fadhli AN, et al. Paediatric burns in Kuwait: Incidence, causes and mortality. Burns. 2006;32:104–11. doi: 10.1016/j.burns.2005.08.006. [DOI] [PubMed] [Google Scholar]
- 11.Garner WL, Magee W. Acute burn injury. Clin Plast Surg, 2005;32:187–93. doi: 10.1016/j.cps.2004.11.002. [DOI] [PubMed] [Google Scholar]
- 12.Batra AK. Recent trends and socio-cultural determinants in rural India. Burns. 2003;29:270–5. doi: 10.1016/s0305-4179(02)00306-6. [DOI] [PubMed] [Google Scholar]
- 13.Miller SF, Jeng JC, Bessey PQ, et al. National Burn Repository. Chicago, Ill.: American Burn Association; 2005. 51 p. [Google Scholar]
- 14.Fatovich DM, Hughes G, McCarthy S. High bed occupancy and emergency department are bad for patients, staff and the system itself. MJA. 2009;190:362–3. [Google Scholar]
- 15.Hillier DF, Parry GJ, Shannon MW, et al. The effect of hospital bed occupancy on throughput in the pediatric emergency department. Ann Emerg Med. 2009;53:767–76.e3. doi: 10.1016/j.annemergmed.2008.11.024. [DOI] [PubMed] [Google Scholar]
- 16.Sharma PN, Bang RL, Al-Fadhli AN, et al. Paediatric burns in Kuwait: Incidence, causes and mortality. Burns. 2006;32:104–11. doi: 10.1016/j.burns.2005.08.006. [DOI] [PubMed] [Google Scholar]
- 17.Department of Statistics and Medical Records. Ministry of Health, State of Kuwait; http://www.q8whs.com/ . [Google Scholar]
- 18.Saadat M. Epidemiology and mortality of hospitalized burn patients in Kohkiluye va Boyerahmad province (Iran): 2002-2004. Burns. 2005;31:306–9. doi: 10.1016/j.burns.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 19.Attia AF, Sherif AA, Mandil AM, et al. Epidemiological and sociocultural study of burn patients in Alexandria, Egypt. East Med Health J. 1997;3:452–61. [Google Scholar]
- 20.Bang RL, Gang RK, Sanyal SC, et al. Beta-haemolytic Streptococcus infection in burns. Burns. 1999;25:242–6. doi: 10.1016/s0305-4179(98)00167-3. [DOI] [PubMed] [Google Scholar]
- 21.Sharma PN, Bang RL, Ghoneim IE, et al. Predicting factors influencing the fatal outcome of burns in Kuwait. Burns. 2005;31:199–92. doi: 10.1016/j.burns.2004.09.020. [DOI] [PubMed] [Google Scholar]
- 22.Mahaluxmivala S, Borkar AS, Mathur A, et al. A retrospective study of etiopathological and preventive factors in a burns unit in Saudi Arabia. Burns. 1997;23:337–9. doi: 10.1016/s0305-4179(96)00122-2. [DOI] [PubMed] [Google Scholar]
- 23.Hemeda M, Maher A, Mabrouk A. Epidemiology of burns admitted to Ain Shams University Burns Unit, Cairo, Egypt. Burns. 2003;29:353–8. doi: 10.1016/s0305-4179(03)00044-5. [DOI] [PubMed] [Google Scholar]
- 24.Khan N, Malik MA. Presentation of burn injuries and their management outcome. J Pak Med Assoc. 2006;56:394–7. [PubMed] [Google Scholar]
- 25.Calder F. Four yr of burn injuries in a Red Cross hospital in Afghanistan. Burns. 2002;8:563–8. doi: 10.1016/s0305-4179(02)00071-2. [DOI] [PubMed] [Google Scholar]
- 26.Pitkanen J, Al-Qattan MM. Epidemiology of domestic chemical burns in Saudi Arabia. Burns. 2001;27:376–8. doi: 10.1016/s0305-4179(00)00126-1. [DOI] [PubMed] [Google Scholar]
- 27.Soltani K, Zand R, Mirghasemi M. Epidemiology and mortality of burns in Tehran, Iran. Burns. 1998;24:325–8. doi: 10.1016/s0305-4179(98)00017-5. [DOI] [PubMed] [Google Scholar]
- 28.Mabrouk A, El Badawy A, Sherif M. Kerosene stove as a cause of burns admitted to the Ain Shams burn unit. Burns. 2000;26:474–7. doi: 10.1016/s0305-4179(99)00180-1. [DOI] [PubMed] [Google Scholar]
- 29.Estahbanati HK, Bouduhi N. Role of artificial neural networks in prediction of survival of burn patients - a new approach. Burns. 2002;28:579–86. doi: 10.1016/s0305-4179(02)00045-1. [DOI] [PubMed] [Google Scholar]
- 30.Carini L, Grippaud FR, Bartolini A. Epidemiology of burns at the Italian Red Cross Hospital in Baghdad. Burns. 2005;31:687–91. doi: 10.1016/j.burns.2005.04.003. [DOI] [PubMed] [Google Scholar]
- 31.Bang RL, Sharma PN, Gang RK, et al. Burn mortality during 1982 to 1997 in Kuwait. Eur Jour of Epid. 2000;16:731–9. doi: 10.1023/a:1026702201874. [DOI] [PubMed] [Google Scholar]
- 32.Prasannas M, Thomas C. A profile of methicillin resistant Staphylococcus aureus infection in the burn centre of the Sultanate of Oman. Burns. 1998;24:631–6. doi: 10.1016/s0305-4179(98)00108-9. [DOI] [PubMed] [Google Scholar]
- 33.Ali MH. Pattern of burn injuries at King Fahad Hospital, Al-Baha: A study of 277 cases. Annals of Saudi Medicine. 1997;17:104–7. doi: 10.5144/0256-4947.1997.104. [DOI] [PubMed] [Google Scholar]
- 34.Mousa HA. Aerobic, anaerobic and fungal burn wound infections. J Hosp Infect. 1997;37:317–23. doi: 10.1016/s0195-6701(97)90148-1. [DOI] [PubMed] [Google Scholar]
- 35.D’Souza AL, Nelson NG, McKenzie LB. Pediatric burn injuries treated in USA emergency departments between 1990 and 2006. Pediatrics. 2009;124:1424–30. doi: 10.1542/peds.2008-2802. [DOI] [PubMed] [Google Scholar]
- 36.Peden M, Oyegbite K, Ozanne-Smith J, et al. Burns. World report on child injury prevention. Geneva: WHO and UNICEF; 2008. [PubMed] [Google Scholar]
- 37.National Burn Repository Report. American Burn Association; 2005. Dataset Version 2.0. [Google Scholar]
- 38.Saffle JR, Davis B, Williams P. Recent outcomes in the treatment of burn injury in the United States: A report from the American Burn Association Patient Registry. J Burn Care Rehabil. 1995;16:219–32. doi: 10.1097/00004630-199505000-00002. [DOI] [PubMed] [Google Scholar]
- 39. Herndon, DN , editor. “Total Burn Care”. 2nd ed. New York: WBSaunders; 2002. Epidemiological, demographic, and outcome characteristics of burn injury. pp. 16–30. [Google Scholar]
- 40.Esselman PC. Burn rehabilitation: an overview. Arch Phys Med Rehabil. 2007;88 (12 Suppl 2):S3–6. doi: 10.1016/j.apmr.2007.09.020. [DOI] [PubMed] [Google Scholar]