

Abstract
Background
Current examination methods to assess the anatomical variations of flexor digitorum superficialis (FDS) tendon in the little finger necessitate a strong external force applied by the examiner and cause false negatives. A new examination method was designed to detect the variations more accurately.
Methods
We examined the little fingers of 220 adult hands (110 subjects) by 2 methods: the expanded examination method advocated by Tan et al., and a new examination method. Variations of the FDS in the little finger were examined by both methods and categorized separately as having independent FDS function, FDS connection to the tendons of the ring finger or of the multiple adjacent fingers, and functional substitution of the flexor digitorum profundus (FDP) with or without tendinous connection to the ring or multiple adjacent fingers. By our new method, we could further divide the FDS connection or FDP substitution with connection to the ring finger into 2 subtypes: loose and close connections. Data were reported as case numbers and percent. Date on symmetry were statistically analyzed by matched case-control studies.
Results
Among 220 hands, 113 hands (51.4%) had independent FDS function by the new examination method, which was lower than the incidence (55.5%) detected with the existing expanded examination method. In the hands with connections between FDS tendons of the little and the ring fingers, 32 hands (14.5%) demonstrated loose and 37 (16.8%) close connections. Three hands (1.4%) had loose and 19 (8.6%) had close FDP substitution with tendinous connection to the ring finger. Among 110 hands without independent FDS function, variants of 42 hands (38.2%) were asymmetric. There was no statistical significance in symmetry of variations.
Conclusions
This new examination method offers other assessment variations of FDS tendon in the little finger. We recommend using this test to assess the variations and function of the FDS of the little finger.
Keywords: Anatomical variations, Flexor tendons, Examination test
Anatomic studies have shown frequent variations of the flexor digitorum superficialis (FDS), especially of the little fingers.1-6) These variations include thin FDS tendon,1) additional muscle slip from FDS of the adjacent finger,1,3,6) tendinous interconnections between FDS and flexor digitorum profundus (FDP),6) FDS tendon arising from FDP1) or complete absence of the FDS.1,3) Clinically, it is sometimes difficult to judge the variations of the FDS tendon. Traditional exams widely used to detect are the standard and modified superficialis tests. In performing this test, the examiner asks the subject to flex the proximal interphalangeal (PIP) joint of the little finger alone while the other fingers were held extended by the examiner.1,6-9) The modified test,6-9) first described by Baker et al.,7) was based on the standard test. In the modified test, the little and ring fingers were released to flex together to observe the improvement in the PIP joint flexion. Results based on the standard and modified examinations were recorded as FDS-independent, FDS-common, or FDS-deficient.7)
Recently Tan et al.9) recommended a simple expanded Baker's examination technique, which involved a serial release of adjacent finger or multiple fingers to better define the variations of the FDS. However, these tests for FDS were performed with strong extraneous force holding the other fingers fully extended on the table, thus the diversionary effect may exist when there is an interconnection between two adjacent fingers. Different variations may show similar signs. The purpose of this study is to use a new examination method designed to more accurately detect the variations of FDS in the little finger and to compare the results of the expanded Baker's test and this new test.
METHODS
One hundred and ten adult subjects (220 hands) were assessed. They were 50 men and 60 women, with the average age of 34 years (range, 22 to 63 years). They had no previous history of injury, and no tendonitis or connective tissue disorders. They were randomly selected from a pool of college students and office workers. All subjects were evaluated by the same examiner, and all anomalies were photographed.
The FDS function of the little finger was measured by two methods, the expansion of Baker's modified test (abbreviated as "expanded method" below) and the new examination method. The expanded method was based on the standard and modified FDS tests,9) involving serial release of multiple adjacent fingers. Results of FDS functional variants of the little finger tested by the expanded method were categorized into independent FDS function (Fig. 1), FDS connection, and FDP substitution as Tan et al.9) described. The FDS connection (as called "FDS-common") indicates a connection between the little finger of the FDS and adjacent fingers, including two types: the FDS tendon of the little finger has a connection with that of the ring finger or has a connection with the FDS tendons of both the ring and middle fingers (Figs. 2 and 3). FDP substitution designates that inability to actively flex the PIP joint of the little finger without active distal interphalangeal (DIP) joint flexion. This phenomenon occurs when the function of FDS tendon of the finger was deficient. Therefore, the FDP tendon of the little finger has to play a major role in the flexion of PIP joint of the little finger. According to the expanded test of Tan et al.,9) three types of FDP substitutions may exist: 1) the FDP tendon of the little finger has no anatomical connection with the FDP tendon of the other fingers. The FDS tendon of the little finger may be deficient, or anatomically there is fibrous band between the FDS and FDP tendons of the little finger. Therefore there is no independent FDS function; 2) anatomically, the FDP tendon of the little finger has a connection with the FDS or FDP tendons of the ring finger; and 3) the FDP tendon of the little finger has a connection with the flexor tendons of the ring and middle fingers. The methods of testing the above variants were the same as those used by Tan et al.,9) which were detailed in their report.
Fig. 1.

Independent flexor digitorum superficialis function, examined by both the expanded and our new tests. (A) Bilateral palms and corresponding fingers are held facing each other in our new method. (B) The little fingers can touch the dorsal sides of both hands, with the proximal interphalangeal (PIP) joints flexed and the distal interphalangeal (DIP) joints extended in our new method. No gap between the ring fingers is seen. (C) The little fingers flex the PIP joint without DIP flexion by the expanded test.
Fig. 2.

Showing a connection of the flexor digitorum superficialis (FDS) between the little and ring fingers of the right hand by the expanded and our new tests. (A) Examination by the expanded test shows slight flexion at the proximal interphalangeal (PIP) joint, unless (B) releasing of the ring finger allows PIP joint of the little finger flexion. (C) Our new examination test shows when the two ring fingers keep straight and maintain closely touched, difficulty in flexing the PIP joint of the little finger to touch the target. (D) Mild flexion of the PIP joint of the adjacent ring finger was recorded as the loose FDS connection between the little and ring fingers in our new test.
Fig. 3.

The flexor digitorum superficialis (FDS) connection between the little and ring fingers of the right hand. (A) Inability of flexing the proximal interphalangeal (PIP) joint of the little finger of the right hand to touch the target by our new test, in contrast to the little finger of the left hand. (B) When the adjacent ring finger was permitted to flex together, the little finger could flex the PIP joint to reach the aim. Full flexion of the adjacent ring finger was recorded as the close connection between the little and ring fingers. (C) However, this case exhibited independent FDS function of the little finger when tested by the expanded method.
In performing this new examination method, we asked subjects to hold the palms and fingers to be tested and contralateral hand facing each other. Both elbows were in positions of approximately 100 degrees flexion and the wrists were in neutral positions. Then, the little finger of the tested hand was freed and the PIP joint was flexed to a maximal extent. If the little finger could flex the PIP joint to touch the dorsal side of contralateral hand without flexion of the DIP joint of the tested hand and two ring fingers could keep straight and maintain closely touched (Fig. 1), then this would indicate independent FDS function of the little finger. We recorded the FDS function of this little finger as FDS-independent. To touch the dorsal side of the contralateral hand, the PIP joint of the little finger of the tested hand would need to be flexed almost entirely, exceeding 100 degrees.
If the PIP joint of the little finger could not be flexed when the adjacent ring finger was kept straight, or could only be flexed associated with the PIP joint flexion of the same finger, then these would indicate no independent FDS function of the little finger. Then the adjacent ring finger of the tested hand was permitted to be loosened and flexed, while the index and middle fingers of both hands remained straight. If the PIP joint of the little finger could be flexed without the PIP joint flexion, but this occurred together with the PIP joint flexion of the ring finger, we recorded this variant as FDS-connection (or FDS-common). We further divided the FDS-connection into two subtypes according to the extent of flexion of the PIP joint of the adjacent ring finger of the tested hand. Mild flexion (less than 30 degrees) of the PIP joint of the adjacent ring finger of the tested hand was interpreted as the loose connection, which was recorded as FDS-connection to ring finger (loose) (Fig. 2). Conversely, full flexion (more than 110 degrees) of the PIP joint of ring finger of the tested hand indicates a close connection between FDS tendons of the ring and little fingers, which was recorded as FDS-connection to the ring finger (close). Under this condition, the ring fingers of both hands were unable to maintain support and often led to stagger each other. The ring finger of the tested hand flexed the PIP joint by more than 90 degrees, and in most times flexed together with the little finger to touch the dorsal side of the contralateral hand (Fig. 3).
If the PIP joint flexed dependently on the DIP flexion of the same little finger, we asked subjects to attempt to actively flex the PIP joint of the little finger alone. Inability to do so was designated as FDP substitution (or FDS deficiency), including three types as previously mentioned (Fig. 4).
Fig. 4.

The proximal interphalangeal (PIP) joint of the little finger could only be flexed in conjunction with the distal interphalangeal (DIP) joint flexion of the same finger, this was designated as flexor digitorum profundus (FDP) substitution (flexor digitorum superficialis [FDS] deficiency), including three types. 1) A&E showed the PIP joint of the little finger of the right hand flexed dependent on the FDP action of the same finger, but the FDP tendon of the little finger has no anatomical connection with the other fingers. 2) B&F (loose) and C&G (close) showed the FDS deficiency of the little finger of the right hand, and the FDP tendon of the little finger has connection with the FDS or FDP tendons of the adjacent ring finger. 3) D&H showed the FDS deficiency of the little finger of the left hand, and the FDP tendon of the little finger has connection with the flexor tendons of the ring and middle fingers. (A-D) were examined by the expanded method, and (E-H) by our new test.
Data were reported as case number and percent. Date on symmetry were statistically analyzed by matched case-control studies (Stata ver 7.0, Stata Co., College Station, TX, USA). A p-value of more than 0.05 was considered statistically significant.
RESULTS
The results of examination by two methods are given in Table 1. Among the 220 hands, 113 hands (51.4%) had independent FDS function by the new examination method, which was lower than the incidence (55.5%) detected by the expanded method. Nine little fingers (4.1%) showed tendinous FDS connection to the ring finger by the new examination method, but these cases had exhibited independent FDS function when tested by the expanded method.
Table 1.
Variants of FDS of the Small Finger Detected by Two Methods of Examination
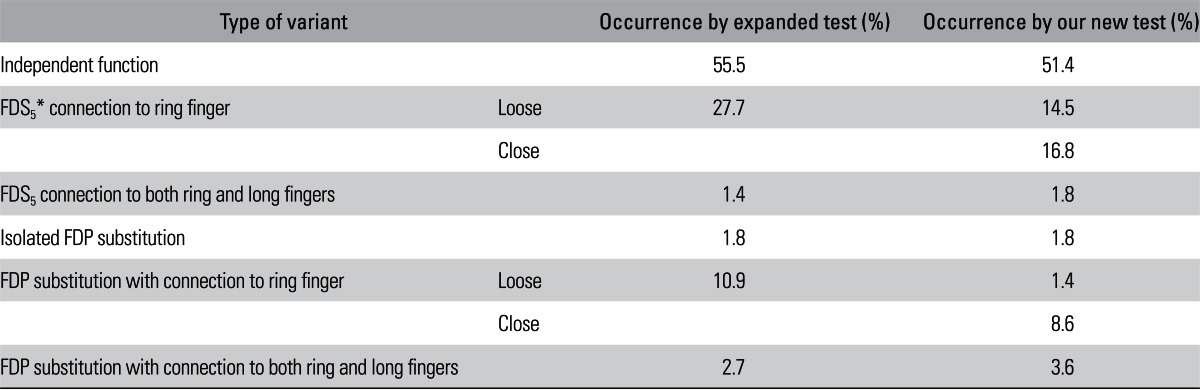
FDS: flexor digitorum superficialis, FDP: flexor digitorum profundus.
*FDS5 is the FDS of the small finger.
The two methods revealed different occurrence of the tendinous FDS connection of the adjacent fingers: 29.1% by the expanded test and 33.2% by the new examination method. For connections of the FDS tendon of the little finger to that of the ring finger, 32 hands (14.5%) demonstrated loose and 37 (16.8%) close connections. Occurrences of FDP substitution detected by the two methods were identical (34 hands of 220, 15.5%). Among the hands with FDP substitution with tendinous connections to the ring fingers, three hands (1.4%) showed loose connection with the ring finger and 19 (8.6%) close connections.
In 110 subjects, 41 (37.3%) showed independent FDS function of the little finger of the bilateral hands. In the subjects of one or two hands without independent FDS function, 38.2% of the FDS variations in the little finger were asymmetric (Table 2). Statistical analysis showed that the occurrences of these variants in two hands were not significantly matched (p < 0.01). Therefore, there was no symmetry of variations of FDS of the little finger between the two hands.
Table 2.
Symmetry of Variations of the FDS of Bilateral Small Fingers (n = 110)
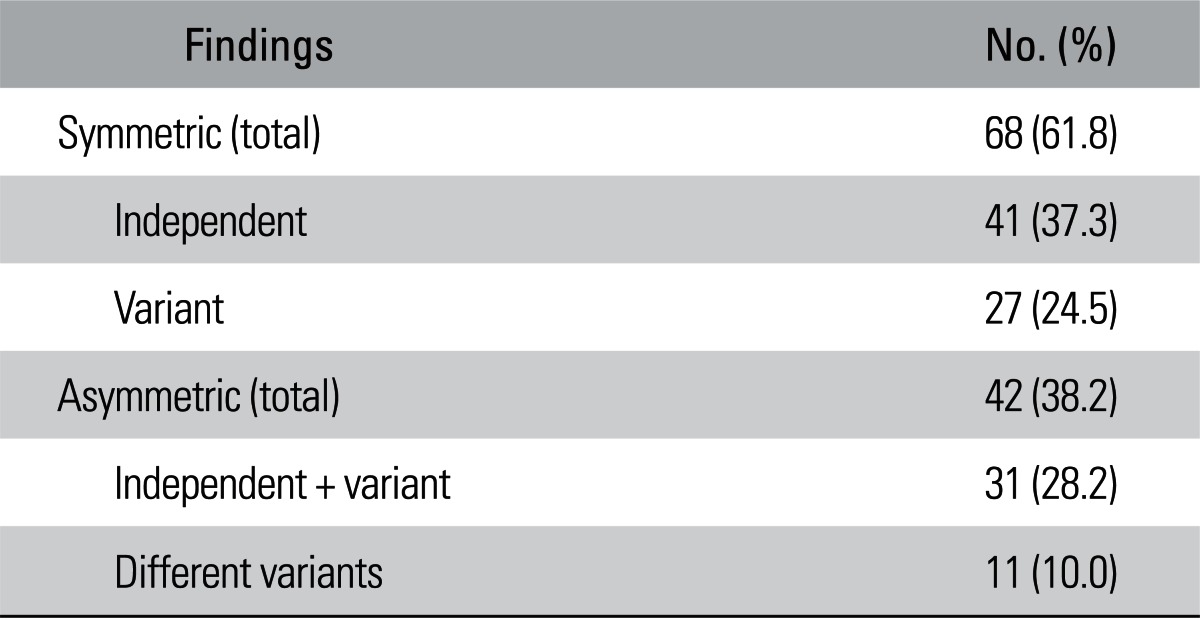
FDS: flexor digitorum superficialis.
DISCUSSION
Variations in the anatomy of the FDS in the fingers are frequent,1-6) which presents difficulty in making a correct clinical diagnosis. Several previous reports have described abnormalities of the superficialis in the little finger.1,3,6-9) FDS tendon was reported absent in about 4%-20% of the hands or FDS common in about 18%-27% of the hands.1,3,6-9) The variations increase the difficulties in deciding suitability of the FDS to the little or ring finger as a potential donor for tendon grafting or transposition procedures. An accurate FDS examination test, therefore, can help hand surgeons make a better judgment of the variations.
The current FDS tests for the little finger are the standard and modified examinations.1,6-8) FDS function was classified into three types: independent, common, and deficient. Tan et al.9) considered that the standard test described by Kaplan1) and Baker's modified test was inadequate to discern between the several variants of the FDS.2) They suggested an expanded method. The expanded method was based on Baker's modified test and involves serial release of not only the ring finger but also the middle finger and observation for the concurrent DIP joint flexion. 9) In our study, 122 of 220 hands (55.5%) showed an independent FDS function by the expanded method.
Our new examination test involves putting the bilateral palms and corresponding fingers face to face closely relied on the forces of their own hands. While the little finger is ordered to flex, influence of the adjacent fingers can be observed apparently if there exists a connection between the little finger and the adjacent fingers. We defined the independent FDS function as no connection between the little finger of the FDS and adjacent fingers; thus the PIP joint of the little finger can move individually. We categorized independent FDS function when the finding that isolate flexing the PIP joint of the little finger touched the dorsal side of the contralateral hand. Among 220 hands, we found that 113 hands (51.4%) had independent FDS function by our new test. The occurrence of independent FDS function was lower compared to the previously reported findings by other tests (Table 3).
Table 3.
Comparison of Studies of Independent FDS Function in the Small Finger
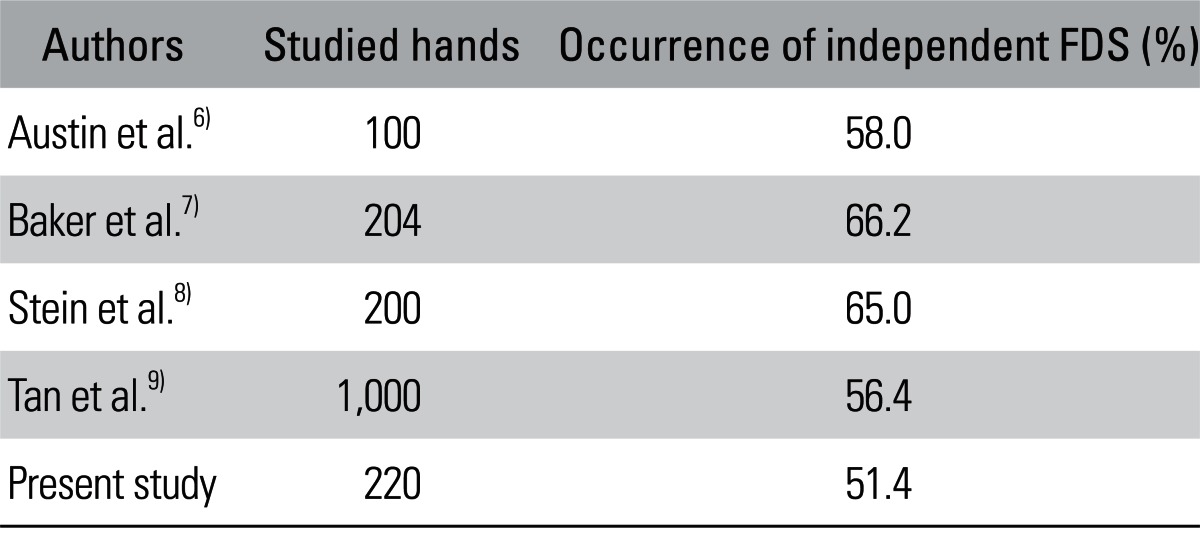
FDS: flexor digitorum superficialis.
The reason for such discrepancies may be that in performing previous tests, the subject is asked to maximally flex the PIP joint of the little finger. To eliminate any effects of FDP on finger flexion, all other fingers are fully extended by a strong extraneous force provided by the examiner. With the strong force, the little finger may deliberately flex the PIP joint, leading to a false independent FDS function. Therefore, connections between the little and adjacent fingers are masked. Our new examination test relies on forces of patients' fingers, which reduces the likelihood of false negatives. In our study, there were nine little fingers (4.1%) that demonstrated independent FDS function by the expanded method, but when tested by our new examination method these showed FDS-connection to the ring finger with various extent.
We used the term "FDP substitution", as described by Tan et al.,9) to designate those cases with PIP joint flexion accompanied by obligatory DIP joint flexion. In those cases, the PIP joint flexion is mostly depended on the FDP function and the role of FDS is weak or deficient. The incidence of FDP substitution (15.5%) in the little finger, tested by both expanded examination and the new tests, is identical. Our findings of FDP substitution were similar to the results (15.5%) reported by Tan et al.,9) Stein et al.8) found that complete absence of function of the FDS in the little finger was rare. This finding of "FDP substitution" by Tan et al.9) was confirmed by our present study.
Our present study is an attempt to exactly assess the variations of FDS tendon in the little finger. Our new examination test revealed that about half of the little fingers have independent FDS function, and about one-third have a connection between the FDS of the little finger and adjacent fingers, and about one-sixth have FDP substitution. These novel findings will aid in better diagnosis of injury of the FDS tendon of the little finger.
Our study showed that 38.2% of subjects were asymmetrical with regard to the variations of the FDS of the little finger, and there was no significant symmetry between the bilateral little fingers. That indicates that results of FDS examination of the little finger of the contralateral hand are of little reference value.
Our study was limited in that, without intuitive dissections or indirect imaging information support, we can only speculate the relations between the variations of the FDS tendon of the little finger and sign of the new test. Another limitation of the new test is that the results may be affected by the muscle tension of hand. Repeated exercises to loosen up the muscle tone before examination may be of help in this regard.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Kaplan EB. Muscular and tendinous variations of the flexor superficialis of the fifth finger of the hand. Bull Hosp Joint Dis. 1969;30(1):59–67. [PubMed] [Google Scholar]
- 2.Shrewsbury MM, Kuczynski K. Flexor digitorum superficialis tendon in the fingers of the human hand. Hand. 1974;6(2):121–133. doi: 10.1016/0072-968x(74)90076-x. [DOI] [PubMed] [Google Scholar]
- 3.Gonzalez MH, Whittum J, Kogan M, Weinzweig N. Variations of the flexor digitorum superficialis tendon of the little finger. J Hand Surg Br. 1997;22(2):277–280. doi: 10.1016/s0266-7681(97)80082-4. [DOI] [PubMed] [Google Scholar]
- 4.Christensen S. Anomalous muscle belly of the flexor digitorum superficialis in two generations. Hand. 1977;9(2):162–164. doi: 10.1016/s0072-968x(77)80013-2. [DOI] [PubMed] [Google Scholar]
- 5.Elias LS, Schulter-Ellis FP. Anomalous flexor superficialis indicis: two case reports and literature review. J Hand Surg Am. 1985;10(2):296–299. doi: 10.1016/s0363-5023(85)80128-3. [DOI] [PubMed] [Google Scholar]
- 6.Austin GJ, Leslie BM, Ruby LK. Variations of the flexor digitorum superficialis of the small finger. J Hand Surg Am. 1989;14(2 Pt 1):262–267. doi: 10.1016/0363-5023(89)90018-x. [DOI] [PubMed] [Google Scholar]
- 7.Baker DS, Gaul JS, Jr, Williams VK, Graves M. The little finger superficialis: clinical investigation of its anatomic and functional shortcomings. J Hand Surg Am. 1981;6(4):374–378. doi: 10.1016/s0363-5023(81)80047-0. [DOI] [PubMed] [Google Scholar]
- 8.Stein A, Lemos M, Stein S. Clinical evaluation of flexor tendon function in the small finger. Ann Emerg Med. 1990;19(9):991–993. doi: 10.1016/s0196-0644(05)82560-0. [DOI] [PubMed] [Google Scholar]
- 9.Tan JS, Oh L, Louis DS. Variations of the flexor digitorum superficialis as determined by an expanded clinical examination. J Hand Surg Am. 2009;34(5):900–906. doi: 10.1016/j.jhsa.2009.01.002. [DOI] [PubMed] [Google Scholar]