

Abstract
Introduction
The equipment for taking body weights (scales) are more frequently used in Cameroon health centres than measuring boards for heights. Even when the later exist there are some difficulties inherent in their qualities; thus the height measurement is not always available or accurate. Our objective for this study was to construct statistical models for predicting wasting from weight-for-age.
Methods
3742 children aged 0 to 59 months were enrolled in a cross-sectional household survey (2004 Cameroon Demographic and Health Surveys (DHS)) covering the entire Cameroon national territory.
Results
There were highly significant association between underweight and wasting. For all discriminant statistical methods used, the test error rates (using an independent testing sample) were less than 5%; the Area Under Curve (AUC) using the Receiver Operating Characteristic (ROC) was 0.86.
Conclusion
The study showed that weight-for-age can be used for accurately classifying a child whose wasting status is unknown. The result is useful in Cameroon as too often the height measurements may not be feasible, thus the need for estimating wasted children. This study provides baseline information that will help to design a preliminary pivotal study on an immediate nutrition intervention for acute undernutrition. Its complications that could lead to morbidity and mortality can be greatly reduced or set up a management control strategy that will go a long way in reducing the cost of health care in Cameroon.
Keywords: Anthropometric measures, nutritional status, discriminant analysis, underweight, wasting
Introduction
Childhood undernutrition is one of the important health problems in developing countries. More than 3.6 million mothers and children die each year as a result of undernutrition [1]. The evaluation of young children's nutritional status uses the Z-score which measures the distance, expressed in standard deviations of the standard (reference) population between the individual's anthropometry and the median of the standard (reference) population. The most frequent anthropometric indicators are height-for-age, weight-for-height and weight-for-age. A Z-score greater than 2 would indicate over-nourishment with respect to the corresponding anthropometric measurements. Deficits on these indicators (measured by their values less than -2 standard deviations below the median based on the 2006 WHO Child Growth Standards [2], that is both severe and moderate status for each of the above anthropometric measurements) are known as stunting, wasting and underweight respectively. Some criticisms have been raised regarding the reliability of these indicators. These include the fact that the assumption that the expected weight for a given height does not depend on age is unjustified for constructing the weight-for-height index [3–5]. For instance, Cole [3–5] proposed an age-standardized version of weight-for-height. For the 2006 WHO Child Growth Standards, the standard population is an international sample which is constituted of Brazil, Ghana, India, Norway, Oman and the United States of America (USA), whereas the reference one for NCHS/CDC/WHO is constituted solely of the USA sample population [6–8].
The Millennium Development Goals (MDG) focus on fighting against poverty, mortality, morbidity and undernutrition [9]. One of the aims is to reduce by half the prevalence of underweight among children by 2015. Such an initiative requires the identification of the determinants of undernutrition for the design of appropriate policy interventions.
We were not interested here in the determinants of undernutrition; rather on relationships between the anthropometric measurements. From a practical point of view, apart from the data on age that are easily obtained from recorded files, equipments are required to perform anthropometric assessment. For weight and height, the most common types of equipment used are scales and measurement boards. In Cameroon, electronic scales are available in most health centres. However, the measurement boards for height are not always available, making it difficult to have data on height. Baby balances that are calibrated for length or height are not always readily available in these health centres. Given that high association has been reported between underweight and wasting [6, 7, 17, 18, 24], the main objective of this study was to find out statistical discriminant models to predict wasted children from their weight-for-age scores in the absence of height measurements.
Methods
Data for 3742 children aged 0 to 59 months were obtained from the 2004 Cameroon Demographic and Health Survey (DHS) that was carried out by Cameroon's National Institute of Statistics and ORC Macro (USA). The sample of Cameroon's DHS was a nationally representative household survey that used a two-stage stratified random sampling design. The first stage was the selection of primary sampling units (PSU) within each of the 22 strata and the second was the selection of households within each PSU. The survey consisted of a household questionnaire and a women's questionnaire. On the average, 22 households were selected in an urban PSU and 28 in a rural PSU for a total of 11584 households. Women aged 15-49 years identified in the households were interviewed. The women's questionnaire contained information on several topics including: background characteristics, contraceptive knowledge and use, maternity and breastfeeding, immunization of children, diarrhea, fever, and cough in children, marriage, fertility preferences, husband's background, work status, age, height and weight of children. A more general description of the DHS methodology can be found in Rutstein and Rojas [18].
The methodology for computing anthropometric indicators was based on the 2006 WHO Child Growth Standards. Statistical models used include the following discriminant analysis: Linear Discriminant Analysis (LDA), Quadratic Discriminant Analysis (QDA), K-Nearest Neighbour (KNN), Epanechnikov Kernel Discriminant (EKD), Normal Kernel Discriminant (NKD), Logistic Discriminant Analysis (LDA), Support Vector Machine (SVM), Neural networks (NNET), Mixture Discriminant Analysis (MDA), Flexible Discriminant Analysis (FDA), Multivariate Adaptive Regression Splines (MARS) and Adaptive Backfitting (BRUTO). The K-nearest neighbour (K-NN) discriminant uses K = 3. The method is relatively insensitive to the choice of K, especially for large samples [19]. This was the case in our application; different values of K did not lead to substantial differences. Kernel nonparametric discriminant method such as Epanechnikov and normal were used with radius 0.3. Varying the radius did not substantially modify the result. Other kernel methods such as uniform, biweight and triweight yield similar results. Logistic regression was used to model the probability of being wasted. A description of these discriminant methods can be found in Hastie et al. [20].
Discriminant Analysis (DA) is a multivariate technique designed to find boundaries that separate items belonging to two or more known groups [19]. It provides a different perspective of viewing wasting as a one-dimensional summary of weight-for-age (underweight). The coding was: wasting=underweight=1; not-wasting=not-underweight=0. The response variable was wasting status whereas the predictor was weight-for-age. The sensibility measures the ability of the technique to correctly classify wasted children. It is the percentage of wasted children that the technique correctly classifies as such. The specificity measures the ability of the technique to correctly classify not wasted children. It is the percentage of not wasted children that the technique correctly classifies as not wasted children. True positive (TP) is the number of wasted children correctly classified; False negative (FN) is the number of wasted children incorrectly classified; True negative (TN) is the number of not wasted children correctly classified and False positive (FP) is the number of not wasted children incorrectly classified.
Ideally, one would like the sensibility and specificity to be 1. However it is not uncommon to have higher sensitivity but lower specificity (or the reverse). A receiver-operator characteristic (ROC) curve helps to visualize and understand the magnitude of the tradeoff between sensitivity and specificity, especially when the technique involves making a choice between continuum cut-off values. Because of the tradeoff between sensitivity and specificity, the Area Under the Curve (AUC) and the error rate are common tools for measuring the quality a discriminant model. A perfect model has AUC of 1 and no error rate.
In order to determining the test error rate, we randomly split the data (3742 children) in two, two thirds (2495) for estimating the discriminant model and one third (1247) for prediction. This avoided using the same data for estimation and prediction.
Statistical analyses were performed with the Statistical Analysis Systems statistical software package version 6.12 (SAS Institute, Cary, NC, USA) [21] and R (version 2.14.1) [22].
Results
Wasting was observed in 5.5% of children and underweight in 12.9% (Figure 1). As expected, Figure 1 shows that the predicted probability of being wasted (using logistic regression) decreased as the height-for-age score increased. Pearson's correlation between weight-for-age and weight-for-height was 0.6. Underweight status was associated with wasting (Pearson's chi-squared = 534.4, P=0) (Table 1)
Figure 1.
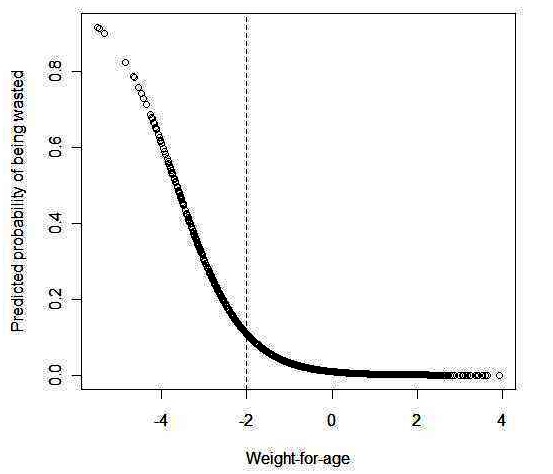
Predicted probability of being wasted using logistic regression as function of weight-for-age
Table 1.
Discriminant analysis methods for wasting as function of weight-for-age
| Discriminant Method | TP* | FP | FN | TN | Se | Sp | Test Error rate |
|---|---|---|---|---|---|---|---|
| Linear Discriminant Analysis (LDA) | 13 | 8 | 45 | 1181 | 0.224 | 0.993 | 0.043 |
| Quadratic Discriminant Analysis (QDA) | 13 | 9 | 45 | 1180 | 0.224 | 0.992 | 0.043 |
| K-Nearest Neighbour (KNN) | 17 | 16 | 41 | 1173 | 0.293 | 0.987 | 0.046 |
| Epanechnikov Kernel Discriminant (EKD) | 13 | 8 | 45 | 1181 | 0.224 | 0.993 | 0.043 |
| Normal Kernel Discriminant (NKD) | 9 | 2 | 49 | 1187 | 0.155 | 0.998 | 0.041 |
| Logistic Discriminant Analysis (LDA) | 13 | 9 | 45 | 1180 | 0.224 | 0.992 | 0.043 |
| Support Vector Machine (SVM) | 9 | 3 | 49 | 1186 | 0.155 | 0.997 | 0.042 |
| Neural networks (NNET) | 11 | 8 | 47 | 1181 | 0.190 | 0.993 | 0.040 |
| Mixture Discriminant Analysis (MDA) | 15 | 13 | 46 | 1176 | 0.259 | 0.989 | 0.045 |
| Flexible Discriminant Analysis (FDA) | 13 | 8 | 45 | 1181 | 0.224 | 0.993 | 0.043 |
| Multivariate Adaptive Regression Splines (MARS) | 14 | 12 | 44 | 1177 | 0.241 | 0.990 | 0.045 |
| Adaptive Backfitting (BRUTO) | 13 | 9 | 45 | 1180 | 0.224 | 0.992 | 0.043 |
True Positive (TP), False Positive (FP), False Negative (FN), True Negative (TN), Sensitivity (Se), Specificity (Sp)
The comparison between true wasting status (from data) and the predicted wasting status (using DA) showed that the agreement was excellent between both as evidenced by low error rates in Table 1. The grouping of children given in the data was almost identical to that obtained using DA, using an independent sample of children. The predictive ability of various discriminant analysis methods was demonstrated by their test error rate less than 5%. Figure 2 showed an AUC of 0.86, providing evidence of a good classification.
Figure 2.
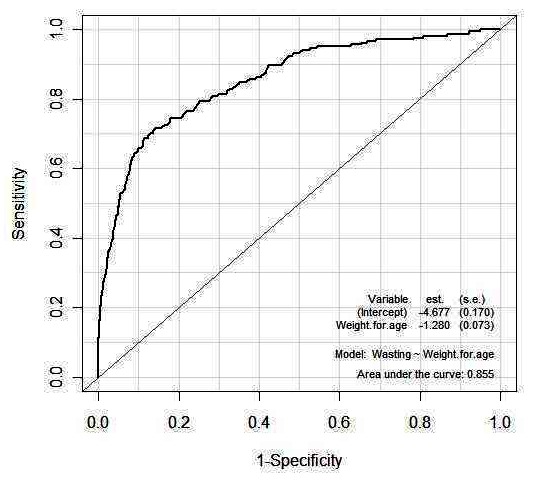
Receiver Operating Caracteristics (ROC) Curve for Wasting Status
Discussion
According to WHO classification, the 5.5% observed for wasting and 12.9% for underweight were both considered medium. These figures were slightly different from the 5.0% and 13.2% respectively for wasting and underweight that were obtained using the NCHS/CDC/WHO international reference standard worldwide used prior to year 2006.
The results of these studies only apply to this sample and associations may change depending on sample′s settings, age range, and prevalence rates. Thus a multi-country study could be carried out to find out how the results would vary across countries. One could also perform an ecological study across selected countries (or all countries with similar available data). However, the drawbacks of such studies are well known. The results may be very different at the individual level. It is well known that ecological correlation studies should be interpreted with caution [23]. De Onís et al. [24] performed an ecological correlation analysis of 22 African countries and found that the prevalence of underweight was positively associated with wasting and stunting and there was a very low correlation between wasting and stunting. Victora [25] showed similar results for others African countries. Similar results could also be found in Centers for Disease Control and Prevention [26]. Blössner et al. [27] in an ecological study using 122 countries also developed a simple regression model using least squares method to predict the prevalence of stunting from the prevalence of underweight. Their models performed well only for the region of Asia and the prediction was not reliable for other regions. In related studies with thirty-eight anthropometric surveys of Brazilian children aged up to 5 years, Victora et al.[28] used the prevalence of weight deficits to estimate that of height deficits with a linear model and concluded that anthropometric surveys as conducted in Brazil, in the context of health services, can be simplified by measuring weight only, instead of both weight and height.
Various factors can affect undernutrition: inadequate intake of vitamins and minerals, suboptimal breastfeeding and complementary feeding practices, socioeconomic factors, demographic and environmental characteristics, food intake that is continuously insufficient to meet dietary energy requirements, poor absorption and/or poor biological use of nutrients consumed may affect undernutrition. There is a sizeable literature on the determinants of undernutrition using anthropometric indicators as dependent variables [10–16]. It is important to note that two other (less popular) methods for evaluating the children's nutritional status are the percentage of the median and the percentile methods. WHO Child Growth Standards can serve as a diagnostic tool to assess unhealthy trends. In addition, the standard could help in monitoring the nutritional status of communities and alert practitioners and policymakers to unhealthy trends in the population. Stunting status, usually referred as chronic (past) undernutrition (growth retardation) represents a measure of long term effects of malnutrition in a population and does not vary significantly according to the season of data collection [17]. Wasting status, usually referred to as acute (current) undernutrition (emaciation) is appropriate for examining short-term effects such as seasonal changes in food supply or short-term nutritional status due to a factor like an illness. Underweight takes into account both chronic and acute undernutrition and is usually used to monitor nutritional status on a longitudinal basis. This suggests that the choice of a particular anthropometric indicator depends on the goal of the policy maker; that is no single index is to be used for all situations.
Conclusion
In Cameroon, measuring boards for height measurements of children are not always available in some health centres. The weight-for-age scores can be useful for predicting the wasting status of children in these centres. This study provides baseline information that will help to design a preliminary pivotal study on an immediate nutrition intervention for acute undernutrition. Its complications that could lead to morbidity and mortality can be greatly reduced or set up a management control strategy that will go a long way in reducing the cost of health care in Cameroon.
Acknowledgments
We thank the DHS Data Archive (ICF Mac¬ro, USA) for providing us with the data. Special thanks to Mercedes de Onìs (Nutrition for Health and Development, World Health Organization, Geneva) for helpful comments on earlier versions of this paper.
Competing interests
The author(s) declare that they have no competing interests.
Authors’ contributions
Dr Nguefack-Tsague conceptualized the paper, performed the statistical analyses and methods, and wrote the preliminary manuscript. Drs Tanya and Fokunang guided the analyses and were co-responsible for nutritional aspects and policy implications. All authors reviewed different drafts of the manuscript, contributed to the final paper and approved de final version.
References
- 1.Black RE, Allen LH, Bhutta ZA, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371:243–260. doi: 10.1016/S0140-6736(07)61690-0. [DOI] [PubMed] [Google Scholar]
- 2.Geneva: WHO; 2007. WHO Anthro for personal computers, version Software for assessing growth and development of the world's children. http://www.who.int/childgrowth/software/en/ [Google Scholar]
- 3.Cole TJ. A method for assessing age-standardized weight-for-height in children seen cross-sectionally. Ann Hum Biol. 1979;6:249–268. doi: 10.1080/03014467900007252. [DOI] [PubMed] [Google Scholar]
- 4.Cole TJ. A critique of the NCHS weight for height standard. Hum Biol. 1985;57:183–196. [PubMed] [Google Scholar]
- 5.Cole TJ. A new index of child weight-for-height based on weight and height Z scores. Ann Hum Biol. 1994;21:96. [Google Scholar]
- 6.Gorstein J, Sullivan K, Yip R, et al. Issues in the assessment of nutritional status using anthropometry. Bull World Health Organ. 1994;72:273–283. [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. WHO Technical Report Series. Geneva: WHO; 1995. Physical status: the use and interpretation of anthropometry. N0 854. [PubMed] [Google Scholar]
- 8.de Onís M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr. 1996;64:650–658. doi: 10.1093/ajcn/64.4.650. [DOI] [PubMed] [Google Scholar]
- 9.United Nations. United Nations Development Programme; A better world for all. Available at http://www.paris21.org/betterworld/pdf/bwa_e.pdf. Accessed 26 May 2012. [Google Scholar]
- 10.Pelletier D. The relationship between child anthropometry and mortality in developing countries. J Nutr. 1994 Oct;124(10 Suppl):2082S–2105S. doi: 10.1093/jn/124.suppl_10.2082S. [DOI] [PubMed] [Google Scholar]
- 11.UNICEF. New York: UNICEF; 1998. The State of World's Children: Focus on Nutrition. [Google Scholar]
- 12.de Onís M, Frongillo EA, Blössner M. Is malnutrition declining? An analysis of changes in levels of child malnutrition since 1980. Bull World Health Org. 2000;78:1222–1233. [PMC free article] [PubMed] [Google Scholar]
- 13.Smith L, Haddad L. How potent is economic growth in reducing undernutrition? What are the pathways of influence? New cross-country evidence. Econ Dev Cult Change. 2002;51:55–76. [Google Scholar]
- 14.Caputo A, Foraita R, Klasen S, et al. Undernutrition in Benin-an analysis based on graphical models. Soc Sci Med. 2003;56:1677–1697. doi: 10.1016/s0277-9536(02)00162-4. [DOI] [PubMed] [Google Scholar]
- 15.Behrman J, Skoufias E. Correlates and determinants of child anthropometrics in Latin America: background and overview of the symposium. Econ Hum Biol. 2004;42:335–352. doi: 10.1016/j.ehb.2004.10.002. [DOI] [PubMed] [Google Scholar]
- 16.Klasen S. Poverty, undernutrition, and child mortality: some interregional puzzles and their implications for research and policy. Journal of Economic Inequality. 2008;6:89–115. [Google Scholar]
- 17.Cogill B. Food and Nutrition Technical Assistance Project. Washington D.C: Academy for Educational Development; 2003. Anthropometric Indicators Measurement Guide. [Google Scholar]
- 18.Rutstein SO, Rojas G. Guide to DHS Statistics, Demographic and Health Survey. Maryland: ORC Macro Calverton; 2006. [Google Scholar]
- 19.Khattree R, Naik DN. Multivariate Data Reduction and Discrimination with SAS Software. Cary NC: SAS Institute Inc; 2000. [Google Scholar]
- 20.Hastie T, Tibshirani R, Friedman J. The elements of statistical learning: data mining, inference and prediction. New York: Springer; 2001. [Google Scholar]
- 21.SAS Institute Inc. Cary NC: SAS Institute Inc; SAS/STAT Software: Changes and Enhancements, through Release 6.11 and 6.12. [Google Scholar]
- 22.R Development Core Team. Vienna, Austria: R Foundation for Statistical Computing; R: A language and environment for statistical computing. Avialbale at http://www.R-project.org. Accessed 26 May 2012. [Google Scholar]
- 23.Kelsey JL, Thompson WD, Evans AS. Methods in observational epidemiology. New York: Oxford University Press; 1986. [Google Scholar]
- 24.de Onís M, Monteiro C, Akré J, et al. The worlwide magnitude of protein-energy malnutrition: an overview from the WHO Global Database on Child Nutrition. Bull World Health Org. 1993;71:703–712. [PMC free article] [PubMed] [Google Scholar]
- 25.Victora CG. The association between wasting and stunting: an international perspective. J Nutr. 1992;122:1105–1110. doi: 10.1093/jn/122.5.1105. [DOI] [PubMed] [Google Scholar]
- 26.Centers for Disease Control and Prevention. Nutritional assessment of children in drought-affected areas--Haiti, 1990. MMWR Morb Mortal Wkly Rep. 1991 Apr 5;40(13):222–5. [PubMed] [Google Scholar]
- 27.Blössner M, de Onis M, Uauy R. Estimating stunting from underweight survey data. J Hum Ecol. 2006;14:145–152. [Google Scholar]
- 28.Victora CG, Gigante DP, Barros AJ, et al. Estimating the prevalence of height for age deficits based on the prevalence of weight for age deficits among Brazilian children. Rev Saúde públ. 1998;32(4):321–327. doi: 10.1590/s0034-89101998000400003. [DOI] [PubMed] [Google Scholar]