

Abstract
Background:
Ginger rhizomes (rich in gingerols, shogaols, paradols and zingerone) have been used in Asia for the treatment of asthma, diabetes, and pain, and have shown potent anti-inflammatory attributes. Common spices such as Cinnamon (including cinnamic aldehyde and cinnamyl aldehydeis) are used in food and many studies have focused on its anti-inflammatory components. Intense exercise can result in an inflammatory response to cell damage and also muscle soreness. The efficacy of dietary ginger and cinnamon as anti-inflammatory agents and their effectiveness in reducing muscle soreness has been investigated in limited studies on humans. Therefore, we have studied the effects of dietary ginger and cinnamon on inflammation and muscle soreness in Iranian female taekwondo players.
Methods:
Sixty healthy, trained women, aged 13-25 years, were enrolled in the six-week investigation and randomly categorized into three groups (cinnamon, ginger or placebo) and received 3 g of ginger, cinnamon or placebo powder each day, depending on the group they belonged to. The IL-6 level and Likert Scale of Muscle Soreness were evaluated at the beginning and the end of the study and compared among the groups.
Results:
Forty-nine of the participants completed the six-week intervention. There were no significant changes in the IL-6 cinnamon and ginger group when compared with the placebo group, whereas, there was a significant fall in muscle soreness in the cinnamon group and placebo (P < 0.1) and ginger group and placebo (P < 0.01).
Conclusions:
Administration of ginger and cinnamon in athlete women for six weeks did not show any significant change in the IL-6 level, but showed a decrease in muscle soreness in the cinnamon and ginger groups.
Keywords: Athletes, cinnamon, ginger, inflammation, muscle soreness
INTRODUCTION
Zingiber officinale—ginger—has been used in Asia and tropical countries for the treatment of asthma, diabetes, nausea, and pain, and it is classified by the Food and Drug Administration (FDA) as a food additive.[1,2] Several constituents of ginger, especially gingerols and shogaols, paradols, and zingerone, have demonstrated potent anti-inflammatory properties in vitro, through the inhibition of cyclooxygenase 1 and 2,[3–5] blocking of leukotriene synthesis,[6–8] and decreasing the cytokine gene TNF-α and IL-6 expression.[9] This pharmacological property distinguishes ginger from non-steroidal anti-inflammatory drugs.[6]
On the other hand, Cinnamon, the brown bark of the cinnamon tree, is commonly used as a spice and flavoring agent for the preparation of many foods. It was used as a medicine for many years, as well.[10,11] Many nutrients including manganese, dietary fiber, iron, and calcium, occur in cinnamon. Furthermore, it contains three major compounds, cinnamaldehyde, cinnamyl acetate, and cinnamyl alcohol, too.[11,12] Several studies show that the cinnamon extract treatment decreases the mRNA expression of the inflammatory factors [interleukin (IL) 1β, IL6, and TNF-α],[13] and it is able to promote pro-inflammatory gene expression in RAW macrophages,[14] Furthermore, oral administration of the cinnamon extract inhibited development and progression of inflammation by inhibiting expression of COX-2 and pro-inflammatory cytokines (IL-1β, IFN-γ, and TNF-α), while enhancing IL-10 levels.[15]
Strenuous Physical exercise can be regarded as a model of physical stress. Many clinical stressors (e.g., surgery, trauma, burn, sepsis) induce a pattern of hormonal and immunological responses that have a similarity to those of exercise.[16] Several studies have demonstrated increases in mRNA expression for inflammatory cytokines following exercise,[17] as also an increase in IL-1 and TNF-α production.[18,19] Functionally, the cytokines play an important role in initiating the inflammatory response to cell damage. This has been the heightened study of the damage that occurs in the early stages of exposure to eccentric exercise and is commonly referred to as delayed onset muscle soreness (DOMS).[20] Although multiple practices exist for the treatment of DOMS, few have scientific support. The suggested treatments for DOMS are numerous and include pharmaceuticals, herbal remedies, stretching, massage, nutritional supplements, and many more, but DOMS is particularly prevalent in resistance training.[21]
Therefore, in this study, we investigated the effects of 3 g of dietary ginger or cinnamon on muscle soreness and the serum level of IL-6.
METHODS
We conducted a randomized, double-blind, placebo-controlled clinical study involving 60 apparently healthy, well-trained, martial art females (aged 13-25 years), who had exercised at least thrice weekly for three years. Following a health-screening questionnaire, all volunteers provided a written, informed consent. The Committee on Human Research at the University of Isfahan approved the study protocol. Subject eligibility was determined by a history and physical examination. Exclusion criteria included the existence of pathologies interfering with the immune function (i.e., inflammatory diseases), pregnancy or lactation, and participants who avoided taking anti-inflammatory medication, therapies, and additional nutritional supplements during the study. Blood samples were obtained from all subjects 24 hours after specific resistance exercise for the competitive season, a seven-point Likert scale of muscle soreness[22,23] was obtained at 24-hour intervals up to 46 hours post exercise at the baseline and after intervention. The treatment order was determined by an online randomization program (http://www.randomization.com).
Participants consumed 3 g of ginger powder, cinnamon powder or placebo per day with any food, depending on their groups, for a duration of eight weeks. The participants were strongly advised to maintain regular dietary habits and avoid taking additional protein or any supplements for the duration of the study. In an attempt to control the diet, the participants were asked to record their food intake every two weeks of the trial, four times. The serum IL-6 levels were determined using the method described by the Boste human IL-6 ELISA kit.
Statistical analysis
The results are presented as a mean ± standard error. One-way multivariate analysis of covariance (MANCOVA) controlling was used for the pre-test differences, followed by Dennett's post hoc comparison for multiple comparisons between the groups. Within group comparisons were done using the paired samples t-test. On account of the non-normality of the studied variables (positive skewed distribution), a logarithmic transformation was done and homogeneity of the covariance matrix was tested via the Box'M statistics. Analyses were performed with the SPSS version 16 (SPSS Inc, Chicago, IL) statistical package.
RESULTS
Sixty subjects were recruited, with a median (range) age of 19 (13-25) years. Forty-nine of them completed the six-week intervention. Withdrawal from the study was considered as non-compliance of the study. General mean ± SD for all study samples for age (years), weight (kg), and body mass index (BMI, kg/m2) was (17.58 ± 3.6), (53.32 ± 8.35), and (20.49 ± 2.94), respectively. Table 1 presents these variables for each studied group. There are no statistically significant differences between groups in terms of basic characteristics.
Table 1.
Basic characteristics of the participants in the studied groups
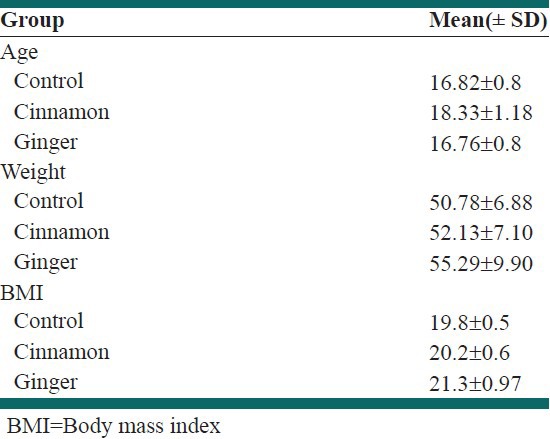
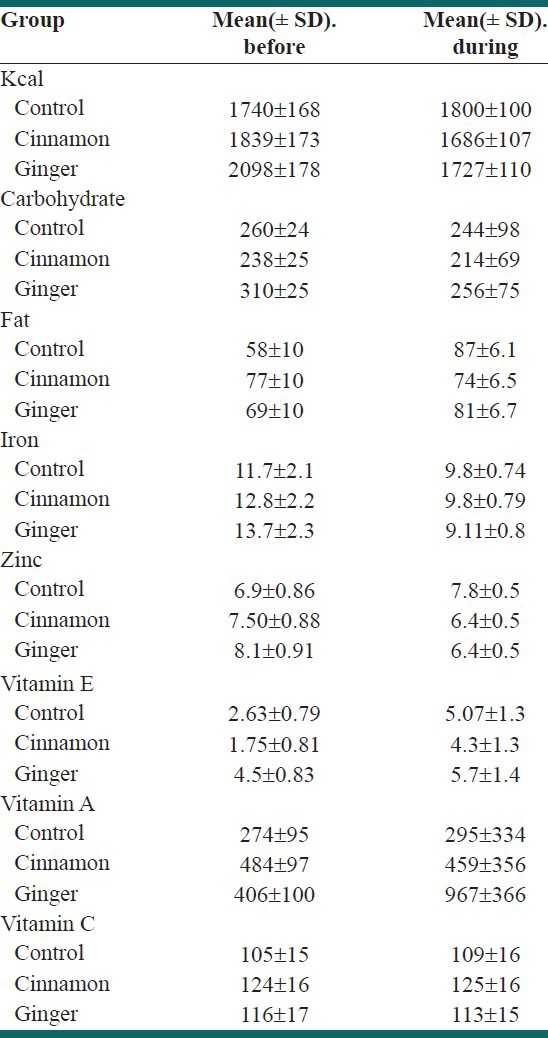
Table 2 illustrates the estimated average intake of some nutrients, before and during the intervention study. There are no statistically significant differences between and within groups in the indicated nutrients.
Table 2.
Estimated average intake of some nutrients, before and during ingestion of placebo (Q), ginger (G), cinnamon (C)
The multivariate analysis of covariance (ANCOVA) result showed a significant difference among the studied groups in terms of study variables (Wilk's λ =0.261, F = 3.467; P < 0.05).
The mean plasma levels of IL-6 and the average data of the muscle soreness, before and after intervention, are shown in Table 3. There were significant falls (paired t-test) in IL-6, in the cinnamon group (P < 0.01) and ginger group (P < 0.001), and a significant decrease in muscle soreness in the ginger group (P < 0.001), whereas, there were no significant differences in IL-6 between all groups (P < 0.1). There was, however, a significant reduction in muscle soreness in the cinnamon group and placebo (P < 0.1) and ginger group and placebo (P < 0.01).
Table 3.
Plasma concentrations of the inflammatory marker and muscle soreness before and after ingestion of placebo (Q), ginger (G), cinnamon (C)
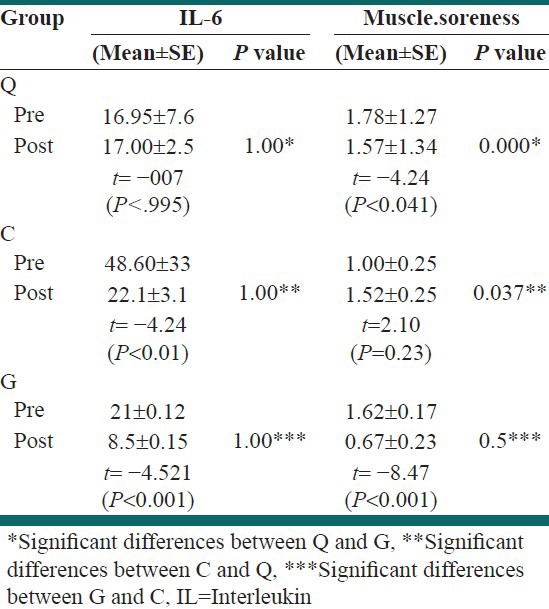
Pre- and post changes in IL-6 for group 1 and control were not statistically significant at P < 0.05 and for group 3 they were decreased but were not statistically significant at P < 0.05. There were no significant changes in the between-group analysis in interleukin 6 (P < 0.5, f = 1.989). However, pre- and post changes in muscle soreness were marginally significant for groups 2 and 3 (P < 0.05). The test between subjects revealed that there were significant falls for muscle soreness (P < 0.05, f = 188.867).
DISCUSSION
The present study was designed to determine whether six weeks intake of 3 g of ginger or cinnamon would influence the plasma levels of IL-6 and the muscle soreness caused by eccentric exercise in female martial athletes. The primary finding was that there were significant falls (paired t-test) in IL-6 in the cinnamon group (P < 0.01) and ginger group (P < 0.001) and a significant decrease in muscle soreness in the ginger groups (P < 0.001). These findings were consistent with the data from the randomized controlled trials, which showed a reduction in an acute-phase inflammatory response, and pain, after daily intake of ginger or cinnamon.[24–26] Another study had detected that ginger consumption demonstrated no effect on muscle pain dysfunction compared with placebo.[27] Considerable evidence supported the anti-inflammatory properties of ginger for several constituents, especially gingerols, shogaols, paradols, and zingerones, through decreased cytokine gene TNF-α and IL-6 expression[9] and inhibition of cyclooxygenase 1 and 2.[3–5,28,29] These established biological actions suggest that ingested ginger could block the increase in IL-6 and pain.
On the other hand, we found that there were no significant differences in IL-6 between all the groups (P < 0.1), which could be explained by the dose of ginger and cinnamon that was not large enough for the assessment time frame and the number of participants in this study, to produce meaningful effects in IL-6 between groups. However, there was a significant reduction in muscle soreness in the cinnamon group and placebo (P < 0.5) and ginger group and placebo (P < 0.01).
CONCLUSION
In summary, the present investigation demonstrated that six weeks of 3 g dietary ginger and cinnamon, on consecutive days, reduced the plasma levels of IL-6 caused by eccentric exercise in female martial athletes, and 3 g of ginger also effectively reduced muscle soreness, but this finding was not supported by 3 g of cinnamon consumption.
Footnotes
Source of Support: Nil
Conflict of Interest: The authors have declared that there is no conflict of interest
REFERENCES
- 1.White B. Ginger: An overview. Am Fam Physician. 2007;75:1689–91. [PubMed] [Google Scholar]
- 2.Wattanathorn J, Jittiwat J, Tongun T, Muchimapura S, Ingkaninan K. Zingiber officinale mitigates brain damage and improves memory impairment in focal cerebral ischemic rat. Evid Based Complement Alternat Med. 2011;2011:429505. doi: 10.1155/2011/429505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Van Breemen RB, Tao Y, Li W. Cyclooxygenase-2 inhibitors in ginger (Zingiber officinale) Fitoterapia. 2011;82:38–43. doi: 10.1016/j.fitote.2010.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nurtjahja-Tjendraputra E, Ammit AJ, Roufogalis BD, Tran VH, Duke CC. Effective anti-platelet and COX-1 enzyme inhibitors from pungent constituents of ginger. Thromb Res. 2003;111:259–65. doi: 10.1016/j.thromres.2003.09.009. [DOI] [PubMed] [Google Scholar]
- 5.Han AR, Kim MS, Jeong YH, Lee SK, Seo EK. Cyclooxygenase-2 inhibitory phenylbutenoids from the rhizomes of Zingiber cassumunar. Chem Pharm Bull (Tokyo) 2005;53:1466–8. doi: 10.1248/cpb.53.1466. [DOI] [PubMed] [Google Scholar]
- 6.Grzanna R, Lindmark L, Frondoza CG. Ginger-an herbal medicinal product with broad anti-inflammatory actions. J Med Food. 2005;8:125–32. doi: 10.1089/jmf.2005.8.125. [DOI] [PubMed] [Google Scholar]
- 7.Jeong CH, Bode AM, Pugliese A, Cho YY, Kim HG, Shim JH, et al. [6]-Gingerol suppresses colon cancer growth by targeting leukotriene A4 hydrolase. Cancer Res. 2009;69:5584–91. doi: 10.1158/0008-5472.CAN-09-0491. [DOI] [PubMed] [Google Scholar]
- 8.Ramadan G, Al-Kahtani MA, El-Sayed WM. Anti-inflammatory and anti-oxidant properties of Curcuma longa (turmeric) versus Zingiber officinale (ginger) rhizomes in rat adjuvant-induced arthritis. Inflammation. 2011;34:291–301. doi: 10.1007/s10753-010-9278-0. [DOI] [PubMed] [Google Scholar]
- 9.Li XH, McGrath KC, Nammi S, Heather AK, Roufogalis BD. Attenuation of liver pro-inflammatory responses by Zingiber officinale via inhibition of NF-kappa B activation in high-fat diet-fed rats. Basic Clin Pharmacol Toxicol. 2012;110:238–44. doi: 10.1111/j.1742-7843.2011.00791.x. [DOI] [PubMed] [Google Scholar]
- 10.Brahmachari S, Jana A, Pahan K. Sodium benzoate, a metabolite of cinnamon and a food additive, reduces microglial and astroglial inflammatory responses. J Immunol. 2009;183:5917–27. doi: 10.4049/jimmunol.0803336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tung YT, Chua MT, Wang SY, Chang ST. Anti-inflammation activities of essential oil and its constituents from indigenous cinnamon (Cinnamomum osmophloeum) twigs. Bioresour Technol. 2008;99:3908–13. doi: 10.1016/j.biortech.2007.07.050. [DOI] [PubMed] [Google Scholar]
- 12.Khuwijitjaru P, Sayputikasikorn N, Samuhasaneetoo S. Subcritical water extraction of flavoring and phenolic compounds from cinnamon bark (Cinnamomum zeylanicum) J Oleo Sci. 2012;61:349–55. doi: 10.5650/jos.61.349. [DOI] [PubMed] [Google Scholar]
- 13.Qin B, Panickar KS, Anderson RA. Cinnamon: Potential role in the prevention of insulin resistance, metabolic syndrome, and type 2 diabetes. J Diabetes Sci Technol. 2010;4:685–93. doi: 10.1177/193229681000400324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cao H, Urban JF, Jr, Anderson RA. Cinnamon polyphenol extract affects immune responses by regulating anti- and pro inflammatory and glucose transporter gene expression in mouse macrophages. J Nutr. 2008;138:833–40. doi: 10.1093/jn/138.5.833. [DOI] [PubMed] [Google Scholar]
- 15.Kwon HK, Hwang JS, Lee CG, So JS, Sahoo A, Im CR, et al. Cinnamon extract suppresses experimental colitis through modulation of antigen-presenting cells. World J Gastroenterol. 2011;17:976–86. doi: 10.3748/wjg.v17.i8.976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chatzinikolaou A, Fatouros IG, Gourgoulis V, Avloniti A, Jamurtas AZ, Nikolaidis MG, et al. Time course of changes in performance and inflammatory responses after acute plyometric exercise. J Strength Cond Res. 2010;24:1389–98. doi: 10.1519/JSC.0b013e3181d1d318. [DOI] [PubMed] [Google Scholar]
- 17.Liburt NR, Adams AA, Betancourt A, Horohov DW, McKeever KH. Exercise-induced increases in inflammatory cytokines in muscle and blood of horses. Equine Vet J Suppl. 2010;38:280–8. doi: 10.1111/j.2042-3306.2010.00275.x. [DOI] [PubMed] [Google Scholar]
- 18.Streltsova JM, McKeever KH, Liburt NR, Gordon ME, Filho HM, Horohov DW. Effect of orange peel and black tea extracts on markers of performance and cytokine markers of inflammation in horses. Physiology. Equine Comp Exerc Physiol. 2006;3:121–30. [Google Scholar]
- 19.Liburt NR, McKeever KH, Streltsova JM, Franke WC, Gordon ME, Filho HM, et al. Effects of ginger and cranberry extracts on the physiological response to exercise and markers of inflammation in horses. Comp Exerc Physiol. 2009;6:157–69. [Google Scholar]
- 20.Zimmermann K, Leidl C, Kaschka M, Carr RW, Terekhin P, Handwerker HO, et al. Central projection of pain arising from Delayed Onset Muscle Soreness (DOMS) in human subjects. PLoS One. (e47230) 2012;7 doi: 10.1371/journal.pone.0047230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cheung K, Hume P, Maxwell L. Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med. 2003;33:145–64. doi: 10.2165/00007256-200333020-00005. [DOI] [PubMed] [Google Scholar]
- 22.Connolly DA, Sayers SP, McHugh MP. Treatment and prevention of delayed onset muscle soreness. J Strength Cond Res. 2003;17:197–208. doi: 10.1519/1533-4287(2003)017<0197:tapodo>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 23.Vickers AJ. Time course of muscle soreness following different types of exercise. BMC Musculoskelet Disord. 2001;2:5. doi: 10.1186/1471-2474-2-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tung YT, Chua MT, Wang SY, Chang ST. Anti-inflammation activities of essential oil and its constituents from indigenous cinnamon (Cinnamomum osmophloeum) twigs. Bioresour Technol. 2008;99:3908–13. doi: 10.1016/j.biortech.2007.07.050. [DOI] [PubMed] [Google Scholar]
- 25.Gaus K, Huang Y, Israel DA, Pendland SL, Adeniyi BA, Mahady GB. Standardized ginger (Zingiber officinale) extract reduces bacterial load and suppresses acute and chronic inflammation in Mongolian gerbils infected with cagAHelicobacter pylori. Pharm Biol. 2009;47:92–8. doi: 10.1080/13880200802448690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Black CD, Herring MP, Hurley DJ, O'Connor PJ. Ginger (Zingiber officinale) reduces muscle pain caused by eccentric exercise. J Pain. 2010;11:894–903. doi: 10.1016/j.jpain.2009.12.013. [DOI] [PubMed] [Google Scholar]
- 27.Black CD, O'Connor PJ. Acute effects of dietary ginger on muscle pain induced by eccentric exercise. Phytother Res. 2010;24:1620–6. doi: 10.1002/ptr.3148. [DOI] [PubMed] [Google Scholar]
- 28.Haghdoost A, Baneshi MR, Zolala F, Farvahari S, Safizadeh H. Estimation of basic reproductive number of flu-like syndrome in a primary school in Iran. Int J Prev Med. 2012;3:408–13. [PMC free article] [PubMed] [Google Scholar]
- 29.Adibi P, Akbari L, Kahangi LS, Abdi F. Health-state utilities in liver cirrhosis: A cross-sectional study. Int J Prev Med. 2012;3(Suppl 1):S94–S101. [PMC free article] [PubMed] [Google Scholar]