

Abstract
Background:
Quercetin, which is considered as a health-promoting antioxidant, belongs to the broad flavonoids group. Numerous experimental studies have proved that quercetin and vitamin C provide anti-inflammatory and antioxidant properties. The aim of this study is to assess the effects of both quercetin and vitamin C on lipid profile and muscle damage in human subjects.
Methods:
A randomized, placebo-controlled, double-blind clinical trial was carried out on 60 males for eight weeks. The subjects were randomly assigned to one of the four groups: 1) quercetin + vitamin C (500 mg/day quercetin + 200 mg/day vitamin C) 2) quercetin (500 mg/day quercetin + 200 mg/day placebo) 3) vitamin C (500 mg/day vitamin C + 200 mg/day placebo) and 4) placebo (500 mg/day placebo + 200 mg/day placebo). Blood samples, body weight and percent of body fat were measured before and after intervention. In addition, dietary intake was estimated using 24-h recall.
Results:
No significant changes occurred in high-density lipoprotein levels between groups and in the four groups before and after supplementation. Low density lipoprotein values decreased significantly (P = 0.048) in the “Quercetin + Vit C” group but decrease was not considerable in other groups before and after intervention and among groups. Fat-soluble vitamins' intake was significantly high among 4 groups.
Conclusions:
Quercetin and vitamin C supplementation may not be beneficial in lipid profile improvement, although it may reduce induce muscle damage and body fat percent.
Keywords: Athletes, lipid profiles, quercetin
INTRODUCTION
Quercetin, which is considered as a health-promoting antioxidant, belongs to the broad flavonoids group.[1–3] Flavonoids present in a variety of natural fruits and vegetables ranging from apple, cranberry to onion, broccoli and teas,[4–7] and along with some nutrients may have positive effects in athletes.[8,9] A large number of epidemiological studies have demonstrated that quercetin provides anti-inflammatory and antioxidant properties.[10–12] Endothelial function is one of the exercise performance determinants and its dysfunction caused by oxidative stress and may induces atherosclerosis.[13] Within a clinic-based study, it has been proved that quercetin improves oxidant status among renal patients through raised serum paraoxonase. Paraoxonase is known as a marker of high-density lipoprotein antioxidant activity which inhibits low-density lipoprotein oxidation.[14] Yi et al., reported that quercetin can reduce oxidized-low-density lipoprotein level and prevent atherosclerosis.[13] In 2011, Yeekh et al., demonstrated that quercetin supplementation significantly alleviates low-density lipoprotein cholesterol concentration and increases serum high-density lipoprotein in the study group.[15] Cadmium oral administration results in an increase in low-density lipoprotein, three acylglycerol, free fatty acids and phospholipids and decrease in high-density lipoprotein. After an experimental investigation, it declared that quercetin can escalate serum high-density lipoprotein and reduce low-density lipoprotein and TG among rats. In addition it eradicates detrimental cadmium effects.[16] Lack of well-documented information about quercetin and vitamin C supplementation containing comprehensive laboratory measurements among athletes draws attention to design more clinical trials in order to define mechanisms. The present study aimed at conducting a research on the effects of both quercetin and vitamin C on lipid profile and muscle damage in human subjects.
METHODS
A randomized, placebo-controlled, double-blind clinical trial was carried out on 60 male athletes who were active, but not involved in professional sports. They were recruited voluntarily and informed about the procedures of study. The exclusion criteria were consumption of quercetin or any other dietary supplements for at least 3 months before the study onset. Participants were requested to abstain from exhaustive exercise 24 h before the beginning of the trial and to keep a record of their recent physical activity and dietary intake. Four subjects left the study due to the gastrointestinal side-effects of supplements. A signed consent was obtained from all participants before the study began. This trial was done in order to test the hypothesis of the beneficial effects quercetin and vitamin C supplementation on male athletes within eight weeks. Participants were randomly assigned to one of four groups including quercetin + vitamin C (500 mg/day quercetin + 200 mg/day vitamin C), quercetin (500 mg/day quercetin + 200 mg/day placebo), vitamin C (500 mg/day vitamin C + 200 mg/day placebo) and placebo (500 mg/day placebo + 200 mg/day placebo). Quercetin, vitamin C and their placebos had a similar appearance. All supplements were orally administrated in capsule form including 500 mg quercetin (Solaray, USA, Inc), 200 mg vitamin C (Razi, Iran, Inc) and placebo (Pharmacy faculty, Isfahan University of Medical Science, Iran) each day after meals. Blood samples were obtained from all subjects between 5:00 pm and 6:00 pm, after intensive exercising, at the outset and after intervention. All measurements were taken at the beginning of the supplementation and end of intervention. Body weight and percentage of body fat were measured using a body composition analyzer (PlusAvis 333, Korea). In addition, plasma samples were collected for the determination of serum lipid profile containing high-density lipoprotein and low-density lipoprotein concentration. high-density lipoprotein and low-density lipoprotein were measured at baseline and again at eight weeks utilizing the Cholestech LDX System (Hayward, CA), according to the manufacturer's instructions. LDH concentrations were measured by the ELISA method, according to the manufacturer's protocol. These ELISA kits were obtained from Bender Medsystems GmbH (Vienna, Austria). Dietary intake was estimated using 24-h recall. Nutrient analyses were performed using nutritionist IV software. Statistical analyses were conducted using the statistical program for social sciences (SPSS Version 13, Inc., Chicago, IL) computer software package. The results are presented as mean ± standard error. One-way multivariate analysis of covariance (MANCOVA) controlling for the pre-test differences followed by Dunnett's post hoc comparison was used for multiple comparisons between groups. Within-group comparisons were done using paired t-test. Due to non-normality of the studied variables (positive skewed distribution) logarithmic transformation was done and homogeneity of covariance matrix was tested via BOX'M statistics. Analyses were performed with the SPSS Version 16 (SPSS Inc, Chicago, IL) statistical package. The registration number of this clinical trial is IRCT201112055062N4.
RESULTS
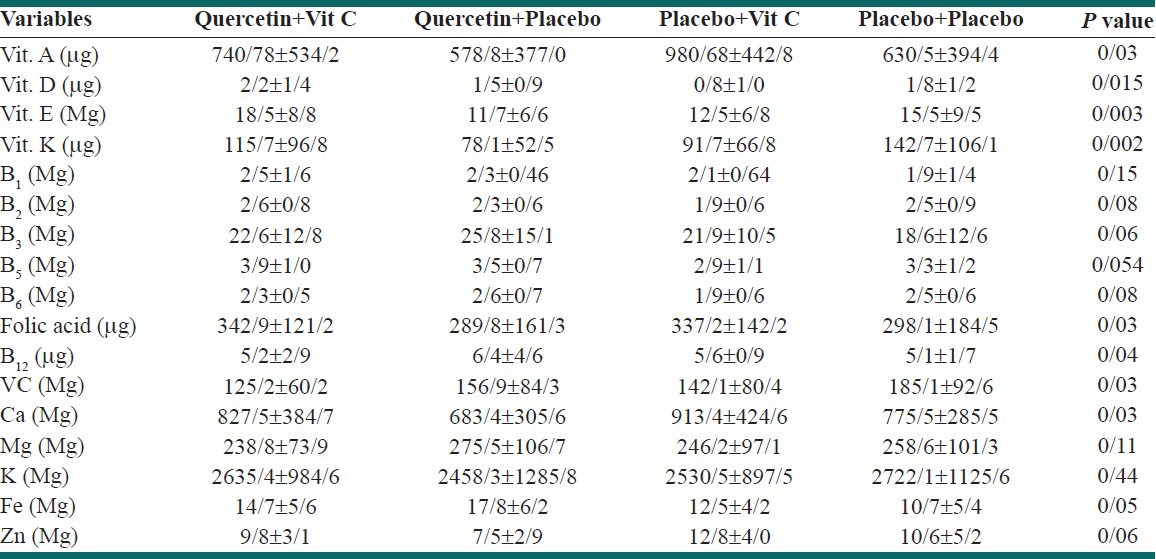
The general mean ± SD of subjects for age (years), weight (kg) and body mass index (BMI, kg/m2) was 21.0 ± 1.6, 67.5 ± 10.8 and 22.3 ± 3.3 respectively. Table 1 shows the mean ± SD values of high-density lipoprotein (HDL), and lactate dehydrogenase (LDH) pre and post supplementation. We did not detect any significant changes in high-density lipoprotein levels between groups and in the four groups before and after supplementation. While LDH values decreased significantly (P = 0.048) in “Quercetin + Vit C” group it was not considerable in other treatments and between groups. Micronutrient intakes are demonstrated in Table 2. Intake of fat-soluble vitamins was significantly high among 4 groups.
Table 1.
The comparison of lactate dehydrogenase and high-density lipoprotein levels between 4 groups
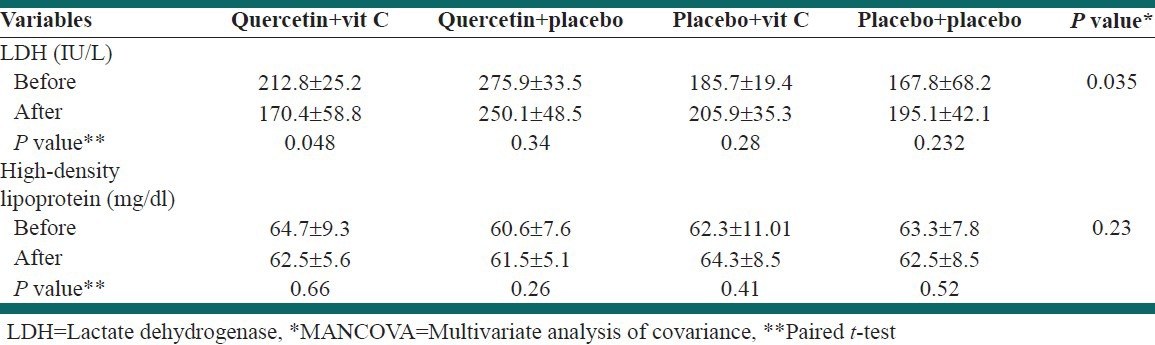
Table 2.
The comparison of mean nutrient intakes between 4 groups
DISCUSSION
The results of our study represent that supplementation with quercetin and vitamin C did not improve the lipid profile as measured by high-density lipoprotein. In contrast to our study, Amengual et al., in a clinical trial study, observed an improved high-density lipoprotein level among renal patients.[14] Different study populations and supplementation dosages might be the possible reasons for the differences in results between the two studies. In line with the previous study, Yeekh et al., reported a significant increase in high-density lipoprotein and decrease in low-density lipoprotein after quercetin supplementation.[15] Another investigation conducted among rats showed different results.[16] The anti-inflammatory and antioxidant properties of quercetin result in reduction of exercise-induced muscle damage.[1,17,18] In accordance with this fact, we observed significant muscle damage as measured by LDH in the quercetin and vitamin C group. The attainable mechanism is that quercetin alleviates the free radical generation during physical activity in skeletal muscle.[18–21]
CONCLUSION
However, in our study, we detected an increase in nutrient intake, notably the fat-soluble vitamins, calcium and folic acid. That may be owing to a gain in dietary intake among all groups. To provide an overview, intake of quercetin and vitamin C supplementation may not be beneficial in lipid profile improvement, although it would probably induce reduction of muscle damage. Hence, more controlled clinical trials considering longer periods of supplementation and larger dosages are needed. The limitations of our study were the limited study population and different physical activity history of athletes. The strengths of this study were human nature of samples and accurate follow-up.
ACKNOWLEDGMENTS
The authors are grateful to the students of the Isfahan Faculty of Nursing and Midwifery, who participated in this study.
Footnotes
Source of Support: This study was conducted as a thesis funded by Isfahan University of Medical Sciences, Isfahan, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Saito K. Possible site of flavonoid synthesis in the photosynthetic apparatus. Biochem J. 1974;144:431–2. doi: 10.1042/bj1440431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Salunkhe DK, Jadhav SJ, Kadam SS, Chavan JK. Chemical, biochemical, and biological significance of polyphenols in cereals and legumes. Crit Rev Food Sci Nutr. 1982;17:277–305. doi: 10.1080/10408398209527350. [DOI] [PubMed] [Google Scholar]
- 3.Middleton EJ, Kandaswami C. The impact of plant flavonoids on mammalian biology: Implications for immunity, inflammation and cancer. In: Harborne JB, editor. The flavonoids: Advances in research since 1986. London: Chapman and Hall; 2005. pp. 619–52. [Google Scholar]
- 4.Shahidi FM. Lancaster: Technomic Publishing Co. Inc; 1995. Food Phenolics: Sources, Chemistry, Effects, Applications. [Google Scholar]
- 5.Kuhnau J. The flavonoids. A class of semi-essential food components: Their role in human nutrition. World Rev Nutr Diet. 1976;24:117–91. [PubMed] [Google Scholar]
- 6.Hertog MG, Hollman PC, Katan MB, Kromhout D. Intake of potentially anticarcinogenic flavonoids and their determinants in adults in The Netherlands. Nutr Cancer. 1993b;20:21–9. doi: 10.1080/01635589309514267. [DOI] [PubMed] [Google Scholar]
- 7.Havsteen B. Flavonoids, a class of natural products of high pharmacological potency. Biochem Pharmacol. 1983;32:1141–8. doi: 10.1016/0006-2952(83)90262-9. [DOI] [PubMed] [Google Scholar]
- 8.Ghiasvand R, Askari Gh, Malekzadeh J, Hajishafiee M, Daneshvar P, Akbari F, et al. Effects of six weeks of β-alanine administration on VO2 max, time to exhaustion and lactate concentrations in physical education students. Int J Prev Med. 2012;8:559–63. [PMC free article] [PubMed] [Google Scholar]
- 9.Ghiasvand R, Djalali M, Djazayery S, Keshavarz S, Hosseini M, Askari G, et al. Effect of Eicosapentaenoic Acid (EPA) and Vitamin E on the blood levels of inflammatory markers, antioxidant enzymes, and lipid peroxidation in iranian basketball players. Iran J Public Health. 2010;1:15–21. [PMC free article] [PubMed] [Google Scholar]
- 10.Hertog MG, Feskens EJ, Hollman PC, Katan MB, Kromhout D. Dietary antioxidant flavonoids and risk of coronary heart disease: The Zutphen Elderly Study. Lancet. 1993;342:1007–111. doi: 10.1016/0140-6736(93)92876-u. [DOI] [PubMed] [Google Scholar]
- 11.Hertog MG, Feskens EJ, Kromhout D. Antioxidant flavonols and coronary heart disease risk. Lancet. 1997;349:699. doi: 10.1016/S0140-6736(05)60135-3. [DOI] [PubMed] [Google Scholar]
- 12.Arts IC, Hollman PC. Polyphenols and disease risk in epidemiologic studies. Am J Clin Nutr. 2005;81:317S–25. doi: 10.1093/ajcn/81.1.317S. [DOI] [PubMed] [Google Scholar]
- 13.Yi L, Jin X, Chen CY, Fu YJ, Zhang T, Chang H, et al. Chemical Structures of 4-Oxo-Flavonoids in Relation to Inhibition of Oxidized Low-Density Lipoprotein (LDL)-Induced Vascular Endothelial Dysfunction. Int J Mol Sci. 2011;12:5471–89. doi: 10.3390/ijms12095471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Amengual-Cladera E, Nadal-Casellas A, Gomez-Perez Y, Gomila I, Prieto RM, Proenza AM, et al. Phytotherapy in a rat model of hyperoxaluria: The antioxidant effects of quercetin involve serum paraoxonase 1 activation. Exp Biol Med (Maywood) 2011;236:1133–8. doi: 10.1258/ebm.2011.011090. [DOI] [PubMed] [Google Scholar]
- 15.Lee KH, Park E, Lee HJ, Kim MO, Cha YJ, Kim JM, et al. Effects of daily quercetin-rich supplementation on cardiometabolic risks in male smokers. Nutr Res Pract. 2011;5:28–33. doi: 10.4162/nrp.2011.5.1.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Prabu SM, Shagirtha K, Renugadevi J. Amelioration of cadmium-induced oxidative stress, impairment in lipids and plasma lipoproteins by the combined treatment with quercetin and α-tocopherol in rats. J Food Sci. 2010;75:T132–40. doi: 10.1111/j.1750-3841.2010.01757.x. [DOI] [PubMed] [Google Scholar]
- 17.Manach C, William G, Morand C, Scalbert A, Remesy C. Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies. Am J Clin Nutr. 2005;81:230S–42. doi: 10.1093/ajcn/81.1.230S. [DOI] [PubMed] [Google Scholar]
- 18.Askari G, Ghiasvand R, Karimian J, Feizi A, Paknahad Z, Sharifirad G, et al. Does quercetin and vitamin C improve exercise performance, muscle damage, and body composition in male athletes? J Res Med Sci. 2012;4:328–31. [PMC free article] [PubMed] [Google Scholar]
- 19.Reid MB. Free radicals and muscle fatigue: Of ORS, canaries, and the IOC. Free Radic Biol Med. 2008;44:169–79. doi: 10.1016/j.freeradbiomed.2007.03.002. [DOI] [PubMed] [Google Scholar]
- 20.Ashrafi F, Haghshenas S, Nematbakhsh M, Nasri H, Talebi A, Eshraghi-Jazi F, et al. The role of magnesium supplementation in cisplatin-induced nephrotoxicity in a rat model: No nephroprotectant effect. Int J Prev Med. 2012;3:637–43. [PMC free article] [PubMed] [Google Scholar]
- 21.Askarian M, Maharlouie N. Irrational antibiotic use among secondary school teachers and university faculty members in Shiraz, Iran. Int J Prev Med. 2012;3:839–45. doi: 10.4103/2008-7802.104854. [DOI] [PMC free article] [PubMed] [Google Scholar]