

Abstract
Background:
The investigation and comparison of the effects of acupuncture and isometric exercises on pain and quality of life in patients suffering from knee osteoarthritis (OA).
OA is the most common form of joint disease and one leading cause of disability in the elderly. The symptoms of OA are pain, morning stiffness, and joint limited motion. Different treatments have been proposed for management of OA, but the results are not clear. We studied the effects of acupuncture and isometric exercises on symptoms of the knee OA.
Methods:
Forty patients with knee OA according to, American college of rheumatology criteria were recruited using strict inclusion and exclusion criteria. All the patients were randomly divided into two groups (A and B).The acupuncture group (A) received only acupuncture at selected acupoint for knee pain. The exercise group (B) received isometric exercise of the knee. Each group received treatment 12 sessions for 4 weeks. Evaluating measuring tools were pain intensity and function was measured with knee injury and OA outcome score (KOOS) questionnaire.
Results:
After treatment, acupuncture and in isometric exercise groups reported that KOOS increased significantly (improvement) in Quality of Life score as shown (P value <0.05). VAS of acupuncture group changed from 7.25 ± 0.91 to 5.41 ± 1.23.In additions, VAS in isometric exercise group changed from 7.85 ± 1.35 to 5.34 ± 1.26. Total KOOS scores have not shown significant difference in comparative with exercise group (P value > 0.11).
Conclusions:
Both acupuncture and isometric exercises decrease pain and increase quality of life in patients who suffer from OA.
Keywords: Acupuncture, isometric exercise, osteoarthritis, pain
INTRODUCTION
Osteoarthritis (OA) is the most common disease of synovial joints.[1] The highest outbreak of the disease is in the women and especially after the age 55, and is the cause of 10% of disabilities in elderly.[2,3] Age has been introduced as the strongest risk-factor.[4] Other factors such as obesity, trauma, metabolic disease and type of job have been known as the pre-disposing factors.[5] Most often affected joints include knee, toe, hip, neck spine, and the joints between hand fingers. Knee OA may occur with pain, joint line tenderness, and limitation of motion, muscle weakness, and atrophy around the knee, especially the quadriceps.[6,7] The disease is diagnosed based on the history, physical examination and radiologic image properties such as osteophyte, decreased joint space, and under – cartilage surface sclerosis.[8] In addition, to non-steroidal Anti-inflammatory drugs. No drugs treatment such as weight loss, physiotherapy, acupuncture and exercise are known effective in decreasing the pain and improving the knee function, although, the study result have been varied from the very good effect to the similar function to placebo.[9,10]
Acupuncture has been more accepted during two recent decades beside the modern medicine and as a complementary medicine. It has been observed that putting a needle in trigger points, which have been introduced for 70% of overlapping with pain points, has resulted in reducing the pain in Chinese acupuncture effectiveness helps physicians to better decide in patients treatment compared with traditional method of isometric exercises.[11] For qualitative assessment changes in patient, pain ruler (VAS) and the Persian version of the knee injury and OA outcome score (KOOS) questionnaire was used.[12]
METHODS
This study was a randomized clinical trial (RCT), and statistical analyzer was used to make the study blind. The study was conducted in rehabilitation and physical medicine clinic of Firoozgar hospital affiliated with Tehran University of medical sciences in 1388.
Patients sampling was performed from available patients with knee OA who referred to physical medicine clinic and had the conditions to enter the study and ready to participate.
Initially, the university ethic committee approval was obtained, and patients consent was taken. This study data was recorded in Iran clinical trial registration center with 138811163284N1. The sample size was determined 20 patients in each group considering the previous studies and totally 40 patients with knee OA were selected based on clinical and radiological symptoms according to American college of rheumatology criteria.
The conditions of entering the study and choosing the samples included: Men and Women with knee pain for 6 months or more (having chronic pain, acute exacerbation of pain) – patients age between 40 and 65 years – a normal neurological examination, including a sense of movement and reflex lack of the knee dispersed pain – radiologic signs of OA in knee, having at least one osteophyte in knee Tibio-Femoral joint (Kellgren–Lawrence grade ≥2) – not-taking intra-articular injection since 3 months ago – not-taking oral Nonsteroidal anti-inflammatory (NSAID) since 1 week before entering the study – no history of knee surgery and severe knee trauma – no history of acupuncture treatment – no pregnancy, cancer, and secondary OA.
Exclusion criteria included: Lack of patient regular visit – using NSAID during the study – worsening symptoms and lack of patient willingness to continue the treatment.
Patients were divided randomly into two groups A and B.
Group A were treated with acupuncture every other day and for 12 sessions (4 weeks). In acupuncture group, GB34, SP10, SP9, ST36, ST35, ST34 points and 0.2 mm × 40 mm needles with penetration depth of 10 mm were used for 15 min. Knee Isometric exercises were used in 3 angles, 0° and 45° and 90° of knee flexion, and each contraction for 6 s repeated 6 times in every angle, 2 times a day.
KOOS standardized questionnaire form and VAS was used for assessment. KOOS questionnaire is an international and standardized questionnaire for assessing the therapeutic outcomes of patients with knee OA. There were five choices for each question that answers were scored from 0 to 4 respectively. And the obtained scores were totally calculated in each sub-group and scored from 0 to 100 that 0 was indicative of no-existence of any problem. (Decreased VAS score and increased KOOS score in a sign of recovery). Results obtained in each subgroup are expressed in five KOOS subgroups. In a form of a quantities amount. This questionnaire has been translated to Persian and localized in Iran, and its Persian version has been confirmed from the view point of repeatability in different studies. KOOS questionnaire is one of the most reliable methods of subjective knee assessment, which can be used in the short and long-term intervals, and changes resulted from the treatment can be evaluated in every week, the test – re test reproducibility level of this questionnaire is high (ICC 0.95) (23).
To comply with the ethical issues and also controlling the use of sedative and equalizing the group, 10 Acetaminophen tablets were given to patients to use in the case of severe pain and report the amount of the used drugs in the next session, because patients were inhibited from using other sedative drugs and were excluded from the study in the case of compulsory use. Entering the study was completely voluntary and patient could be excluded at any time.
The study data were entered using the SPSS software programmed numbered 11 and descriptive. Statistics was presented using the frequency distribution table and statistical indices and diagram also, variance analyze test was used for analyzing the data.
RESULTS
The mean age of acupuncture group has been 55/64 (6/75) years and exercise group 50/35 (8/25). There was no statistically significant difference between the mean age of both group (P value 0.11). The comparison of body mass index mean was indicative of both groups similarity (P value 0.23) two male patients participated in acupuncture group, and three male patients in exercise group. The comparison of obtained scores from KOOS questionnaire, before and after the treatment, in both groups are listed in Tables 1 and 2. The comparisons of obtained scores from any component of the KOOS questionnaire between two groups are shown in Tables 3 and 4. The mean VAS in acupuncture group was 7/25 ± 0/91 pre-treatment and 5/3 ± 1/26.
Table 1.
The comparison of resulted scores in knee injury and osteoarthritis outcome score questionnaire components before and after the treatment in acupuncture group
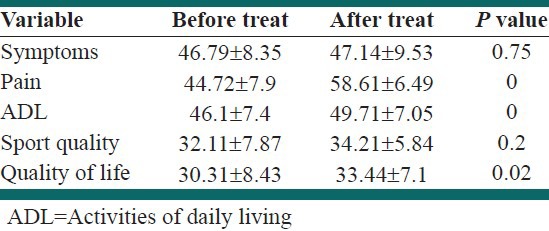
Table 2.
The comparison of resulted scores in knee injury and osteoarthritis outcome score questionnaire components before and after the treatment in isometric exercises group
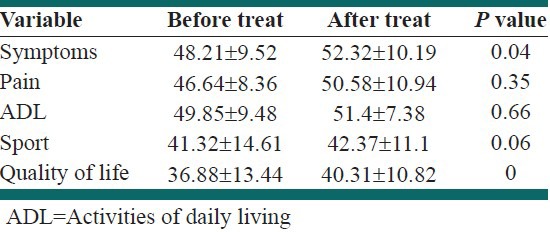
Table 3.
The comparison of the obtained scores from knee injury and osteoarthritis outcome score questionnaire components between two acupuncture and isometric exercises groups 4 weeks before the treatment
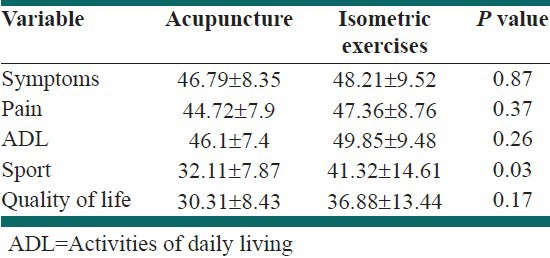
Table 4.
The comparison of obtained scores from knee injury and osteoarthritis outcome score questionnaire components between two acupuncture and isometric exercises groups after 4 weeks of treatment

Unit after the treatment and the comparison of the two means is indicative of a significant decrease in pain intensity (P value < 0.01). Furthermore, the comparison of the VAS mean score before the treatment 7/85 ± 1/35 and before the treatment 5/3 ± 1/26 in exercise group is indicative of a significant decrease in pain intensity (P value <0.01). The comparison of the average pain score changes in both group after the treatment showed no statistically significant difference (P value 0.07).
DISCUSSION
The mean age our patient was consistent with previous studies.[13,14] Age distribution of both under treatment groups was similar. Considering that most important risk-factor has been introduced to be age, it provides the possibility to investigate both groups together and with previous similar studies.[15] Body Mass Index as the second risk-factor was similar in both groups. Both groups of patients were over weighted, which is consistent with the knowledge gained from previous studies. The comparison of both groups reported the similarity of decreased pain. The comparison of KOOS questionnaire scores before and after in each treatment group was indicative of improved quality of life in both groups of patients after the treatment. In exercise group, patients showed improved illness signs after the treatment more than acupuncture group, while decreases pain and improved functional capacity in activities of daily living (ADL) has been more in the group treated with acupuncture. In three similar studies performed to assess the therapeutic effect of acupuncture on OA, the pain changes with the help of VAS pain ruler have been similar to the present study. The investigation of symptoms and life quality in these studies has been performed with the help a questionnaire, which is similar to KOOS questionnaire and the obtained results as our study report the decreased pain, improved joint function and improved daily activities.[15–17] In doctor Imad's study, which compared the effectiveness of acupuncture and Iboprophen in decreasing the pain improved the life quality of patients with OA, decreasing the pain and improving the life quality was similar to acupuncture group of our study.[17] In one study, the therapeutic effect of acupuncture was compared with placebo-acupuncture, and the mentioned study has tried to create a kind of placebo treatment by using points different from main points in acupuncture, however, it cannot be considered as a placebo for sure.[18] To evaluate the exercise in improving OA, the effect of the isometric Exercise therapeutic period by itself or along with electrical stimulation through skin, studies have been conducted, which are indicative of more improvement in most patients under exercise regime to the loose treatment.[19–22] In our study, treating with exercise, and acupuncture have had similar efficacy in improving the patient's life quality. Despite this finding, yet long-term ability of these treatments in reducing pain and improving the life quality of patients is unclear.
Furthermore, due to lack of control group, the effect of passing the time on disease improvement cannot be determined. The better assessment these cases needs RCT with long-term follow-up.
CONCLUSIONS
The results of this study indicate that acupuncture and isometric exercise of knee significantly reduce the pain in knee OA patients, and this decreases pain is more in acupuncture group. Both treatment methods improve daily life activities in patients with knee OA.
ACKNOWLEDGMENTS
We thank and appreciate “research deputy of medical science university” and all of dears who helped us in performing this plan.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: A review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60:91–7. doi: 10.1136/ard.60.2.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Felson DT, Nevitt MC. Epidemiologic studies for osteoarthritis: New versus conventional study design approaches. Rheum Dis Clin North Am. 2004;30:783–97. doi: 10.1016/j.rdc.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 3.Thomas A, Eichenberger G, Kempton C, Pape D, York S, Decker AM, et al. Recommendations for the treatment of knee osteoarthritis, using various therapy techniques, based on categorizations of a literature review. J Geriatr Phys Ther. 2009;32:33–8. doi: 10.1519/00139143-200932010-00007. [DOI] [PubMed] [Google Scholar]
- 4.Lester G. Clinical research in OA – The NIH Osteoarthritis Initiative. J Musculoskelet Neuronal Interact. 2008;8:313–4. [PubMed] [Google Scholar]
- 5.Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med. 2006;2(354):841–8. doi: 10.1056/NEJMcp051726. [DOI] [PubMed] [Google Scholar]
- 6.Steultjens MP, Dekker J, van Baar ME, Oostendorp RA, Bijlsma JW. Muscle strength, pain and disability in patients with osteoarthritis. Clin Rehabil. 2001;15:331–41. doi: 10.1191/026921501673178408. [DOI] [PubMed] [Google Scholar]
- 7.Slemenda C, Brandt KD, Heilman DK, Mazzuca S, Braunstein EM, Katz BP, et al. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med. 1997;127:97–104. doi: 10.7326/0003-4819-127-2-199707150-00001. [DOI] [PubMed] [Google Scholar]
- 8.Sayre EC, Jordan JM, Cibere J, Murphy L, Schwartz TA, Helmick CG, et al. Quantifying the association of radiographic osteoarthritis in knee or hip joints with other knees or hips: The Johnston County Osteoarthritis Project. J Rheumatol. 2010;37:1260–5. doi: 10.3899/jrheum.091154. [DOI] [PubMed] [Google Scholar]
- 9.Maurer BT, Stern AG, Kinossian B, Cook KD, Schumacher HR., Jr Osteoarthritis of the knee: Isokinetic quadriceps exercise versus an educational intervention. Arch Phys Med Rehabil. 1999;80:1293–9. doi: 10.1016/s0003-9993(99)90032-1. [DOI] [PubMed] [Google Scholar]
- 10.Jordan KM, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT) Ann Rheum Dis. 2003;62:1145–55. doi: 10.1136/ard.2003.011742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Melzack R, Stillwell DM, Fox EJ. Trigger points and acupuncture points for pain: Correlations and implications. Pain. 1977;3:3–23. doi: 10.1016/0304-3959(77)90032-X. [DOI] [PubMed] [Google Scholar]
- 12.Sarayi pour S, Salavati M, Akhbari B. Translation of KOOS questionnaire to farsi. Reproducibility and validity in Iranian population. J Rehabil Res. 2007;28:23–34. [Google Scholar]
- 13.Emad MR, Amanollahi A. Comparison of pain reduction between acupuncture and ibuprofen in treatment of knee osteoarthritis. Science Gift. 2007;48:12–8. [Google Scholar]
- 14.Jamtvedt G, Dahm KT, Christie A, Moe RH, Haavardsholm E, Holm I, et al. Physical therapy interventions for patients with osteoarthritis of the knee: An overview of systematic reviews. Phys Ther. 2008;88:123–36. doi: 10.2522/ptj.20070043. [DOI] [PubMed] [Google Scholar]
- 15.Tukmachi E, Jubb R, Dempsey E, Jones P. The effect of acupuncture on the symptoms of knee osteoarthritis: An open randomised controlled study. Acupunct Med. 2004;22:14–22. doi: 10.1136/aim.22.1.14. [DOI] [PubMed] [Google Scholar]
- 16.Itoh K, Hirota S, Katsumi Y, Ochi H, Kitakoji H. A pilot study on using acupuncture and transcutaneous electrical nerve stimulation (TENS) to treat knee osteoarthritis (OA) Chin Med. 2008;3:2. doi: 10.1186/1749-8546-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: A randomized, controlled trial. Ann Intern Med. 2004;141:901–10. doi: 10.7326/0003-4819-141-12-200412210-00006. [DOI] [PubMed] [Google Scholar]
- 18.Jubb RW, Tukmachi ES, Jones PW, Dempsey E, Waterhouse L, Brailsford S. A blinded randomised trial of acupuncture (manual and electroacupuncture) compared with a non-penetrating sham for the symptoms of osteoarthritis of the knee. Acupunct Med. 2008;26:69–78. doi: 10.1136/aim.26.2.69. [DOI] [PubMed] [Google Scholar]
- 19.Topp R, Woolley S, Hornyak J, 3rd, Khuder S, Kahaleh B. The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch Phys Med Rehabil. 2002;83:1187–95. doi: 10.1053/apmr.2002.33988. [DOI] [PubMed] [Google Scholar]
- 20.Cheing GL, Hui-Chan CW. Would the addition of TENS to exercise training produce better physical performance outcomes in people with knee osteoarthritis than either intervention alone? Clin Rehabil. 2004;18:487–97. doi: 10.1191/0269215504cr760oa. [DOI] [PubMed] [Google Scholar]
- 21.Gholipour A, Abolghasemi Sh, Gholinia K, Taheri S. Token Reinforcement therapeutic approach is more effective than exercise for controlling negative symptoms of schizophrenic patients: A randomized controlled trial. Int J Prev Med. 2012;3:466–70. [PMC free article] [PubMed] [Google Scholar]
- 22.Gheissari A, Javanmard SH, Shirzadi R, Amini M, Khalili N. The effects of blocking Angiotensin receptors on early stages of diabetic nephropathy. Int J Prev Med. 2012;3:477–82. [PMC free article] [PubMed] [Google Scholar]