

Abstract
Background:
The anterior cruciate ligament (ACL) is one of the major knee structures. It consists of anteromedial bundle (AMB) and posterolateral bundle (PLB). Rupture of the ACL is one of the most prevalent traumas among athletes. There are two ways to reconstruct the rupture; Single–bundle and double–bundle (DB) reconstruction. Precise study on bundles anatomy, the exact number of attachments and knee flexion angle with an appropriate place of bundles and also choosing the best angle for the grafts are so important in successful reconstructing of the bundles. In this research, the general attempt was to assess anatomy and the act of the ACL is and bundles in Iranian population.
Methods:
We obtained twelve fresh-frozen cadaver knees (two females, ten males). The average age of them was 30 years; they were mostly between 27 and 34 years old. Initially, skin, muscles, and patellar and articular capsule were removed. Then, bundle attachments, knee movements in flexion angle, extension and stiffness of both bundles were evaluated. Thereafter, on 0, 30, 60, 90, 120, and 180° angle knee flexion the bundles degree stiffness evaluated in different directions. During the process, to measure bundles size, digital camera for photography, oblique for measuring the angles, and micrometer were utilized. From all next of kin written consent testimonial form was obtained.
Results:
In all knees, two bundles were identified as distinct. AMB attachment location in the anterior region observed as semi-lunate and in one case, it was rounded. In all cases, two bundles of full knee extension were paralleled, and the AMB was anterior to the PLB; with increasing flexion angle, femoral attachment location of AMB was in back direction and femoral attachment location of PLB moved toward the front direction. Two bundles were in the most amount of cross state, which the angle was 90°. From the stiffness point of view in all 6 samples, the PLB had the most tension in extension state, and the AMB had the most tension in 120° flexion.
Conclusion:
In the current study, we realized that the ACL is a DB ligament in Iranian population. The AMB in full extension has the least stiffness and in 90° flexion has the most; the PLB also in full knee extension and in 160° flexion has the most and least stiffness, respectively.
Keywords: Anterior cruciate ligament, positions, athletes
INTRODUCTION
Anterior cruciate ligament (ACL) is one of the frequent sites of injury in sport,[1] which have been managed by surgical procedure preferably.[2–4] The purpose of ACL reconstruction techniques is the renovation of native anatomy and function of ligament.[5,6] Single bundle ACL reconstruction is one of the established surgical methods, although, 30% of patients have not returned to normal level of function[2] and osteoarthritic changes were developed in 60-90% of them in long-term follow-up,[7–9] which increase the attentions toward double bundle (DB) reconstruction method. A technique resulted in more native anatomy.[10] It was shown that in DB ACL reconstruction, the rotational instability of the knee was restricted by posterolateral bundle (PLB).[11–14] Different factors determine outcome of DB ACL reconstruction such as graft materials, graft fixation, initial graft tensioning, and especially the tibial and femoral tunnel positions of both the anteromedial bundle (AMB) and PLB.[15] As a result, complete information about the normal arrangement of ligament is critical for appropriate anatomic tunnel placement for the two bundles.[16] The normal anatomy or ACL have been studied during recent years, although, there are some controversies among them, especially number of bundles. While Odensten and Gillquist described one bundle,[17,18] Girgis et al. and Arnoczky presented two bundles,[19–21] the anteromedial and the PLBs. The variation of biomechanic of ACL in different studies can be related to factors such as age,[22] gender,[23,24] ethical background[25] and so on. So, anatomical knowledge about normal ACL ligament is necessary in our population to increase restoration of normal function during operation.
In order to, address this we described the anatomy of bundles, the femoral and tibial attachment sites, anatomical position as well as the tension pattern of each bundle in cadaver.
METHODS
We obtained twelve fresh-frozen cadaver knees (two females, ten males). The average age of them was 30 years; they were mostly between 27 and 34 years old. ACL torn knees, history of previous surgery, injury, and degenerative disease to the knees were excluded from the study. There were six left and six right knees. Ethical approval of this study was obtained from the Ethics Committee of Tehran University of Medical Science. Skin, muscles, patella, and the joint capsule were observed and documents were recorded then except the ACL, PCL, medial, and lateral meniscus and the collateral ligaments, all soft tissues were removed. Identifying the AM and PL bundle were done according to tension pattern of them during joint motion, AMB was tighten during flexion, and the PLB was tighten during extension. The two bundles were remarked by wrapping a string. After that the PCL ligament was excised and to expose the femoral attachment of the ACL the medial femoral condyle was removed with a spots Tension pattern and anatomical position change of each bundle were evaluated at 0, 30, 60, 90, 120, and 180° of knee flexion.
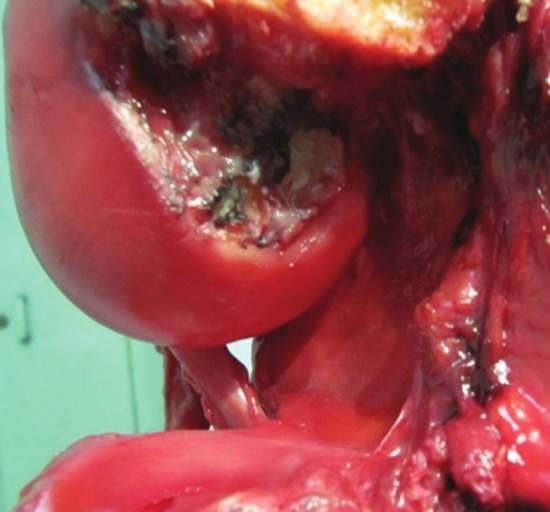
Following that, femoral and tibial attachment sites were marked with ink. After removal of the AM and PL bundle, the center of the femoral insertion site of each bundle was also marked. The anatomical position of femoral and tibial insertion site of two bundles was described three planes (sagital, frontal, transvers). We determined the angle formed between a horizontal line and a line connecting the center of the femoral insertion of each bundle at 90 knee flexion and full extension. Then, the length and width of the length of the ACL tibial insertion was measured as the distance between the anterior and the posterior edge of the tibial insertion and the width was measured at its widest part between tibial condyle [Figure 1]. The length and the width of the insertion on the femur were measured in maximal flexion of the knee joint. The length of the femoral insertion was measured from the most proximal to the most distal point of ACL insertion in the direction of posterior femoral cortex [Figure 2]. The width of the femoral insertion was measured as the greatest perpendicular distance between the line of femoral insertion length and the beginning of the joint surface at the point of outer femoral condyle's greatest convexity. Attachments were measured by digital photographs or micrometer. The length of the AMB of the ACL was measured from the anterior edge of the tibial insertion to the medial part of femoral insertion along frontal portion of the AMB. The length of PLB was measured from the posterior edge of tibial insertion to the lateral part of femoral insertion, along back portion of the PLB were measured by a standard micrometer. The ranges along with the mean of our measurements were reported.
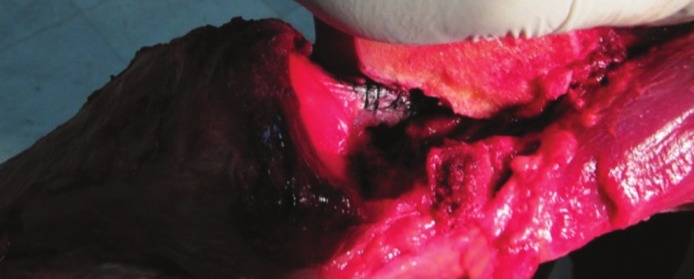
Figure 1.
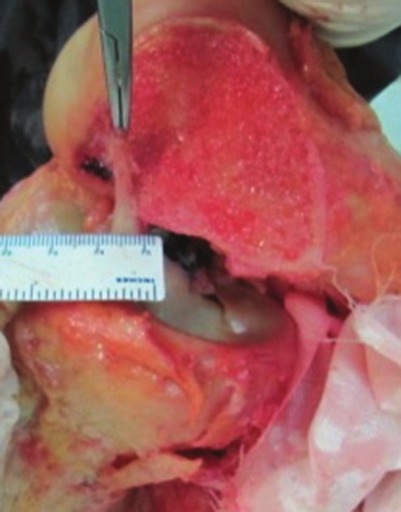
Measurement the width of the PL bundle on tibial insertion
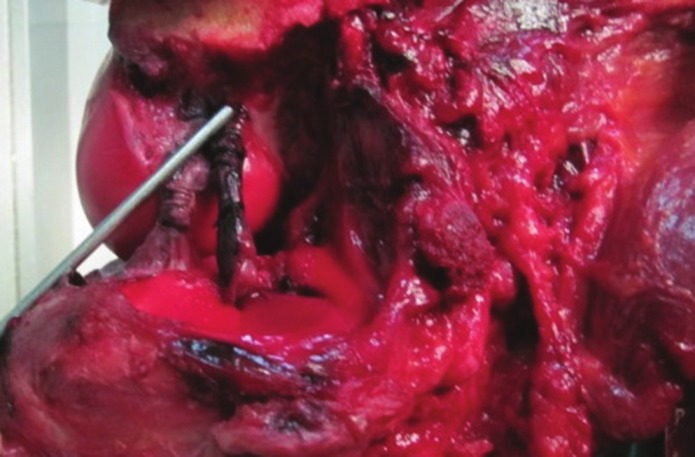
Figure 2.

measurement the lenght of the AM bundle
RESULTS
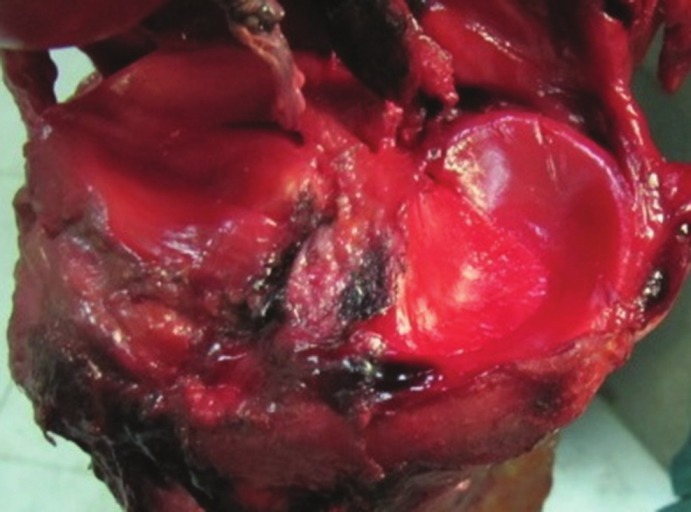
In all cadavers we verified two separate anatomical bundles in ACL ligament, an observation in accordance to some previous studies. The femoral insertion area of the AM bundle was ovally shape at the posterior-inferior part of the inner surface of the lateral condyle with attachment area of 63.83 mm2 [Figure 3].
Figure 3.
The femoral insertion area of the AM bundle
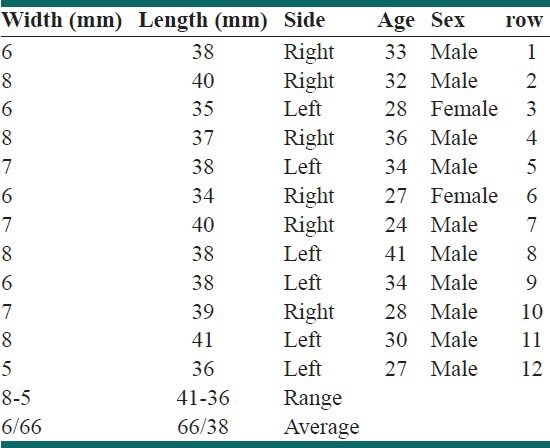
The PL bundle was located in anterior aspect of AM attachment site with semilunar shape except one cadaver with round shape attachment. The insertion site of PL bundle was about 49 mm2. The tibial insertion area of the AM bundle with semilunar shape in ten cadavers and oval in two cadavers was originated from anteromedian of tibial plateau and medial to the tibial spine with attachment area of 63.87 mm2. The PL bundle area was also located at the anteromedian of tibial plateau but lateral to the tibial spine with attachment site of 51 mm2. In fact, the tibial spine separated the tibial origin of these two bundles [Figure 4]. The length and width of AM and PL bundles were reported in Table 1.
Figure 4.
the tibial origin of AL and PL bundles
Table 1.
Anteromedial bundle size
The anatomical position change of two bundles was evaluated from full extension to 120° of knee flexion [Table 2]. AM and PL was parallel in the sagittal plane with full extended knee and the AM bundle was located in the anterior proximal aspect of the PL bundle, however, the bundles twisted around each other with increasing degrees of knee flexion and femoral insertion site of AM and PL bundles were displaced to posterior and anterior respectively [Figures 5 and 6].
Table 2.
Postero lateral bundle size
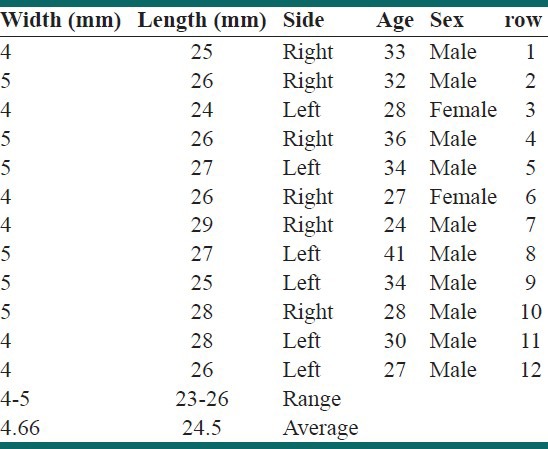
Figure 5.
The bundles was parallel with full extended knee
Figure 6.
The bundles twisted with knee flexion
Tension pattern observation of the AM and PL bundle were revealed AM bundle was tighten as the knee was flexed toward 120, and PL bundle was tighten at full extension.
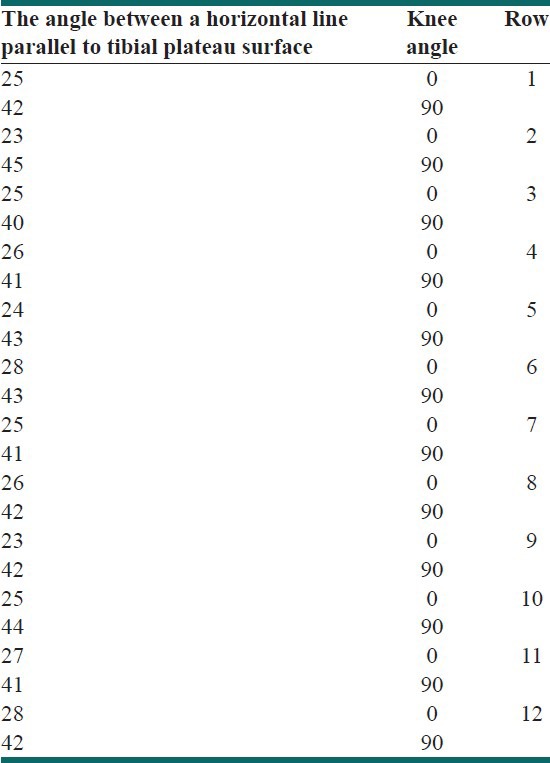
The angle between a orizontal line parallel to tibial plateau surface and a line connecting the center of the femoral insertion of each bundle at 90 knee flexion and full extension is demonstrated in Table 3.
Table 3.
The angle between a horizontal line parallel to tibial plateau surface
DISCUSSION
In all cadavers we distinguished two separate bundles in the ACL ligament, anteromedial and posterolateral bundle, which was consistent with some previous studies.[20,26] As revealed in literature, the Odensten et al. and Heming et al. described one structure[17,18] and Aims et al. and Hollis et al. found three bundles in ACL anatomy.[27,28]
One of the essential factors predicting success in DB ACL reconstruction technique is graft tunnel placement,[29] which requires accurate description of the bundle attachment on femur and tibia.[30] In our study, the femoral attachment of AM bundle was in the posterior-inferior part of the inner surface of the lateral condyle and PL bundle in anterior aspect of it. The posterior part of the inner surface of the lateral condyle has been described by some previous studies as the femoral ACL origin.[17,19,20] Hefzy and Zavras[31,32] have revealed that minor change in the femoral insertion site of ligament had resulted in the length and tensioning patterns difference of the ACL. The tibial insertion area of the AM and PL bundles were anteromedian of tibial plateau where tibial spine separated their origins. Tibial attachment area of AM and PL were 63.87 mm2 and 51 mm2 in our samples, which were in range of other studies, 56 mm2[33] to136 mm2[34] for AM and 52 mm2[24] to 93 mm2[34] for the PL bundle. Furthermore, Femoral attachment area of AM and PL were 63.83 mm2 and 49 mm2 in our samples, which were in range of other studies, 44 mm2[23] to120 mm2[35] for AM and 40 mm2[23] to 103 mm2[34] for the PL bundle.
In other observation, AM and PL was parallel in the sagittal plane with full extended knee and the AM bundle was located in the anterior proximal aspect of the PL bundle, however, the bundles twisted around each other with increasing degrees of knee flexion toward 90° and femoral insertion site of AM and PL bundles were displaced to posterior and anterior respectively. Hollis et al.,[28] Duthon et al.,[36] Takashi et al.[25] and Steckel et al.[2] approved the parallel and twisted orientation in full extension and 90° flexion respectively.[12] Another study showed the PL bundle lies behind the AM bundle in an anteroposterior direction.[37–39] Moreover, it was revealed that the femoral origin of the PL bundle is posterior and inferior of the AM bundle when knee is extended, although, in flexion it placed anterior the origin of AM bundle on the lateral femoral condyle.[37] Considering this position is essential especially in arthroscopic surgery in which the knee is flexed.
The initial tension of grafts significantly affected the values of each graft tension at each knee flexion in DB ACL reconstruction, although there is no consensus regarding bundle-tensioning protocols.[36,37]
CONCLUSION
In our survey, tension pattern study of the AM and PL bundle demonstrated AM bundle tighten as the knee was flexed toward 120°, and PL bundle was tighten at full extension. In accordance to our findings, in previous studies the AM bundle tightened at 90° knee flexion and the PL bundle tightened in the full extended knee[2,28,34,37] or about 0-15° flexion.[13] In biomechanical evaluation of ACL by Takai et al.[36] and Hollis et al.[28] 3.3 mm and 3.6 mm increasing of AM bundle length were reported in 90° knee flexion in order and in both study decreasing of PL bundle length was shown in full extension knee which indicate that the tension of bundles should be considered in DB ACL reconstruction.
The average angle between the tibial plateau surface and a line connecting the center of the femoral insertion of each bundle at 90 knee flexion and full extension was 42.33 and 25.16° respectively. The only study in literature review was measured the angle between a horizontal line and the line connecting the center of the femoral insertion of the AM and PL bundle in the sagittal plane in 0, 30, 60, 90, 120, and 150° which was 55.2, 79.2, 105.7, 136.8, 170.2, and 205.8 in order.[2]
During recent years surgeons are more interested in DB reconstruction of ACL to restore the normal function of ligament [5,34,36] so, knowledge of ACL anatomy is essential to the success of double-tunnel reconstructions. As there is wide variety in anatomical structure of ligament in different population,[22] study of our population was one of the priority, which assists to better outcome of our surgeries. Although, some limitations are noticeable in our study such as small sample size, lack of enough female cadaver to compare the effect of sex in ACL anatomy. More surveys are needed to elaborate more details of ACL anatomy in future.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;3:216–31. doi: 10.1097/00003086-197501000-00033. [DOI] [PubMed] [Google Scholar]
- 2.Birrer RB, Birrer CD. Medical injuries. In: Springfield IL, Charles C, editors. Medical Injuries in the Martial Arts. Washington: Thomas Publisher; 1981. pp. 23–65. [Google Scholar]
- 3.Shen W, Jordan S, Fu F. Review article: Anatomic double bundle anterior cruciate ligament reconstruction. J Orthop Surg (Hong Kong) 2007;15:216–21. doi: 10.1177/230949900701500219. [DOI] [PubMed] [Google Scholar]
- 4.Matsumoto H, Suda Y, Otani T, Niki Y, Seedhom BB, Fujikawa K. Roles of the anterior cruciate ligament and the medial collateral ligament in preventing valgus instability. J Orthop Sci. 2001;6:28–32. doi: 10.1007/s007760170021. [DOI] [PubMed] [Google Scholar]
- 5.Ryder SH, Johnson RJ, Beynnon BD, Ettlinger CF. Prevention of ACL injuries. J Sports Rehabil. 1997;6:80–9. [Google Scholar]
- 6.Brown CH, Jr, Carson EW. Revision anterior cruciate ligament surgery. Clin Sports Med. 1999;18:109–71. doi: 10.1016/s0278-5919(05)70133-2. [DOI] [PubMed] [Google Scholar]
- 7.Beynnon BD, Johnson RJ, Fleming BC, Peura GD, Renstrom PA, Nichols CE, et al. The effect of functional knee bracing on the anterior cruciate ligament in the weightbearing and nonweightbearing knee. Am J Sports Med. 1997;25:353–9. doi: 10.1177/036354659702500314. [DOI] [PubMed] [Google Scholar]
- 8.Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH. In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res. 1997;15:285–93. doi: 10.1002/jor.1100150219. [DOI] [PubMed] [Google Scholar]
- 9.Fu FH, Lo MY, Lo MS, Pombo MW, Singleton R. Pittsburgh, PA: University of Pittsburgh; 2004. Anatomic double- bundle, Anatomic Double-Bundle ACL Reconstruction Patient Information Handout/ Frequently Asked Questions; pp. 45–124. [Google Scholar]
- 10.Gerich TG, Lattermann C, Fremerey RW, Zeichen J, Lobenhoffer HP. One-versus two-incision technique for anterior cruciate ligament reconstruction with patellar tendon graft. Results on early rehabilitation and stability. Knee Surg Sports Traumatol Arthrosc. 1997;5:213–6. doi: 10.1007/s001670050052. [DOI] [PubMed] [Google Scholar]
- 11.Odensten M, Gillquist J. Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone Joint Surg Am. 1985;67:257–62. [PubMed] [Google Scholar]
- 12.Arnoczky SP. Anatomy of the anterior cruciate ligament. Clin Orthop Relat Res. 1983;5:19–25. [PubMed] [Google Scholar]
- 13.Amis AA, Dawkins GP. Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J Bone Joint Surg Br. 1991;73:260–7. doi: 10.1302/0301-620X.73B2.2005151. [DOI] [PubMed] [Google Scholar]
- 14.Hollis JM, Takai S, Adams DJ, Horibe S, Woo SL. The effects of knee motion and external loading on the length of the anterior cruciate ligament (ACL): A kinematic study. J Biomech Eng. 1991;113:208–14. doi: 10.1115/1.2891236. [DOI] [PubMed] [Google Scholar]
- 15.Johnson DL. Knee injuries plaguing young female athletes. 2007 [Google Scholar]
- 16.Sanchis-Alfonso V, Subías-López A, Monteagudo-Castro C, Rosello-Sastre E. Healing of the patellar tendon donor defect created after central-third patellar tendon autograft harvest. A long-term histological evaluation in the lamb model. Knee Surg Sports Traumatol Arthrosc. 1999;7:340–8. doi: 10.1007/s001670050177. [DOI] [PubMed] [Google Scholar]
- 17.Muneta T, Takakuda K, Yamamoto H. Intercondylar notch width and its relation to the configuration and cross-sectional area of the anterior cruciate ligament. A cadaveric knee study. Am J Sports Med. 1997;25:69–72. doi: 10.1177/036354659702500113. [DOI] [PubMed] [Google Scholar]
- 18.Hara K, Kubo T, Suginoshita T, Shimizu C, Hirasawa Y. Reconstruction of the anterior cruciate ligament using a double bundle. Arthroscopy. 2000;16:860–4. doi: 10.1053/jars.2000.7679. [DOI] [PubMed] [Google Scholar]
- 19.Yasuda K, Kondo E, Ichiyama H, Kitamura N, Tanabe Y, Tohyama H, et al. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20:1015–25. doi: 10.1016/j.arthro.2004.08.010. [DOI] [PubMed] [Google Scholar]
- 20.Cha PS, Brucker PU, West RV, Zelle BA, Yagi M, Kurosaka M, et al. Arthroscopic double-bundle anterior cruciate ligament reconstruction: An anatomic approach. Arthroscopy. 2005;21:1275. doi: 10.1016/j.arthro.2005.07.018. [DOI] [PubMed] [Google Scholar]
- 21.Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: An anatomic study. Arthroscopy. 2007;23:1218–25. doi: 10.1016/j.arthro.2007.09.008. [DOI] [PubMed] [Google Scholar]
- 22.Fu FH, Shen W, Starman JS, Okeke N, Irrgang JJ. Primary anatomic double-bundle anterior cruciate ligament reconstruction: A preliminary 2-year prospective study. Am J Sports Med. 2008;36:1263–74. doi: 10.1177/0363546508314428. [DOI] [PubMed] [Google Scholar]
- 23.Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE. Distribution of in situ forces in the anterior cruciate ligament in response to rotatory loads. J Orthop Res. 2004;22:85–9. doi: 10.1016/S0736-0266(03)00133-5. [DOI] [PubMed] [Google Scholar]
- 24.Souryal TO, Moore HA, Evans JP. Bilaterality in anterior cruciate ligament injuries: Associated intercondylar notch stenosis. Am J Sports Med. 1988;16:449–54. doi: 10.1177/036354658801600504. [DOI] [PubMed] [Google Scholar]
- 25.Shelbourne KD, Facibene WA, Hunt JJ. Radiographic and intraoperative intercondylar notch width measurements in men and women with unilateral and bilateral anterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 1997;5:229–33. doi: 10.1007/s001670050055. [DOI] [PubMed] [Google Scholar]
- 26.Teitz CC, Lind BK, Sacks BM. Symmetry of the femoral notch width index. Am J Sports Med. 1997;25:687–90. doi: 10.1177/036354659702500517. [DOI] [PubMed] [Google Scholar]
- 27.Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB. Analysis of the intercondylar notch by computed tomography. Am J Sports Med. 1987;15:547–52. doi: 10.1177/036354658701500605. [DOI] [PubMed] [Google Scholar]
- 28.Sommer C, Friederich NF, Müller W. Improperly placed anterior cruciate ligament grafts: Correlation between radiological parameters and clinical results. Knee Surg Sports Traumatol Arthrosc. 2000;8:207–13. doi: 10.1007/s001670000125. [DOI] [PubMed] [Google Scholar]
- 29.Kopf S, Musahl V, Tashman S, Szczodry M, Shen W, Fu FH. A systematic review of the femoral origin and tibial insertion morphology of the ACL. Knee Surg Sports Traumatol Arthrosc. 2009;17:213–9. doi: 10.1007/s00167-008-0709-5. [DOI] [PubMed] [Google Scholar]
- 30.Steckel H, Starman JS, Baums MH, Klinger HM, Schultz W, Fu FH. The double-bundle technique for anterior cruciate ligament reconstruction: A systematic overview. Scand J Med Sci Sports. 2007;17:99–108. doi: 10.1111/j.1600-0838.2006.00600.x. [DOI] [PubMed] [Google Scholar]
- 31.Kennedy JC, Weinberg HW, Wilson AS. The anatomy and function of the anterior cruciate ligament. As determined by clinical and morphological studies. J Bone Joint Surg Am. 1974;56:223–35. [PubMed] [Google Scholar]
- 32.Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006;14:204–13. doi: 10.1007/s00167-005-0679-9. [DOI] [PubMed] [Google Scholar]
- 33.Takai S, Woo SL, Livesay GA, Adams DJ, Fu FH. Determination of the in situ loads on the human anterior cruciate ligament. J Orthop Res. 1993;11:686–95. doi: 10.1002/jor.1100110511. [DOI] [PubMed] [Google Scholar]
- 34.Zaffagnini S, Martelli S, Acquaroli F. Computer investigation of ACL orientation during passive range of motion. Comput Biol Med. 2004;34:153–63. doi: 10.1016/S0010-4825(03)00041-6. [DOI] [PubMed] [Google Scholar]
- 35.Zantop T, Wellmann M, Fu FH, Petersen W. Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: Anatomic and radiographic findings. Am J Sports Med. 2008;36:65–72. doi: 10.1177/0363546507308361. [DOI] [PubMed] [Google Scholar]
- 36.Takahashi M, Doi M, Abe M, Suzuki D, Nagano A. Anatomical study of the femoral and tibial insertions of the anteromedial and posterolateral bundles of human anterior cruciate ligament. Am J Sports Med. 2006;34:787–92. doi: 10.1177/0363546505282625. [DOI] [PubMed] [Google Scholar]
- 37.Steckel H, Starman JS, Baums MH, Klinger HM, Schultz W, Fu FH. Anatomy of the anterior cruciate ligament double bundle structure: A macroscopic evaluation. Scand J Med Sci Sports. 2007;17:387–92. doi: 10.1111/j.1600-0838.2006.00579.x. [DOI] [PubMed] [Google Scholar]
- 38.Aremu O, Lawoko S, Dalal K. The influence of individual and contextual socioeconomic status on obstetric care utilization in the Democratic Republic of Congo: A population-based Study. Int J Prev Med. 2012;3:278–85. [PMC free article] [PubMed] [Google Scholar]
- 39.Moshki M, Atarodi BA, Moslem A, Taheri M. Applying an educational-participatory program based on the PRECEDE model for promoting self-esteem and mental health of students in Iran. Int J Prev Med. 2012;3:241–8. [PMC free article] [PubMed] [Google Scholar]