

Abstract
Ghrita (ghee) is the foremost substance of Indian cuisine from centuries. Ayurvedic classics described eight kinds of ghee from eight different animal milk, among them ghee made from cow milk is said to be the superior and ghee of ewe milk is said to be the inferior and also detrimental to heart. The present study was undertaken to evaluate chronic administration of cow ghee (Go Ghrita) and ghee of ewe milk (Avika Ghrita) to experimental animals. Experiment was carried out on Wistar strain albino rats and study was done at two dose levels. The test drugs were administered orally for 45 consecutive days. Parameters, such as gross behavior, body weight, weight of important organs, total fecal fat content, electrocardiogram, serum biochemical parameters, and histopathology of different organs were studied. Both the test drugs did not alter the gross behavior, body weight, weight of organs, and cytoarchitecture of different organs to significant extent. Avika Ghrita at a low dose significantly decreased triglyceride content, significantly prolonged QTc and at both dose levels it significantly shortened the PR interval. This study shows chronic administration of Avika Ghrita and Go Ghrita has no marked differences between them except the QTc prolongation in Avika Ghrita. This may be the basis for the classics to categorize Avika Ghrita as Ahridya.
Keywords: Ahridya, albino rats, Avika Ghrita, cholesterol, ghee, Go Ghrita
Introduction
Ahara (diet), Nidra (sleep), and Brahmacharya (chastity or self-restriction in the use of sense organs) have been considered as three subpillars of life. Food is at leading place among these three because of its prime importance in life-sustaining substances. Sukha (health) or Dukha (disease) depends on Hita (good) or Ahita (awful) effects of food taken by the person. According to Maharshi Kashyapa there is no medicine like Ahara (food) on the earth.[1] This is a clear indication of medicinal use of diet articles. In spite of all these good qualities and importance, the same Ahara (food) can cause various kinds of serious disorders in the body. This is why Maharshi Charaka said that the body as well as the disease is the product of Ahara (food).[2] Ghrita (ghee) is the foremost substance of Indian cuisine from centuries. Any region might be spotted out where Ghrita is not used as daily routine diet article. Regardless of warnings from modern medical science, Indian population uses Ghrita in their regular diet. Ghrita can be made from the milk of different animals. Ayurvedic classical texts described eight kinds of ghee from eight different animal milk and ghee made from cow milk is said to be superior among them,[3] whereas ghee of ewe milk is said to be inferior.[4] Maharsi Caraka has mentioned it as Ahridya (detrimental to heart).[5] In the present era, due to less production and high-priced, adulteration of Ghrita is very common. To counteract this problem, dairy industry is expanding its area for products made from the milk other than cow and buffalo for satisfying the demand of ghee. Milk of ewe is one of them which is planned to use for production of ghee. When there is clear reference available regarding Ahridya (detrimental to heart) effect of Avika Ghrita (ghee of ewe milk) in almost all the classical texts, it is the need of the hour to evaluate it scientifically. Till date no pharmacological data is available regarding this aspect. Hence the present study was undertaken to evaluate chronic administration of Go Ghrita and Avika Ghrita to experimental animals and their effect on various ponderal, biochemical, histopathological, and electro-physiological parameters.
Materials and Methods
Animals
Thirty Wistar strain albino rats of either sex weighing between 160 ± 30 g were selected from animal house attached to the pharmacology laboratory. Animals were maintained on Amrut brand pellets obtained from Pranava Agro Industries, Pune, India, and exposed to ambient temperature, humidity and natural day and night cycles. The experiment was carried out between 8:00 am to 12:00 noon hours of the day. The experimental protocol was submitted to the Institutional Animal Ethics Committee, and approval was obtained for conducting the experiment (Approval number – IAEC/3/07-10/MD 04).
Test drugs
The test drugs Go Ghrita and Avika Ghrita were prepared by adopting standard ghee preparation methods.[6]
Dose fixation
The human dose of Ghrita as practiced traditionally is approximately 10 g per person. Accordingly the dose was calculated by extrapolating the human dose to animals (900 mg/kg) based on the body surface area ratio by referring to the standard table of Paget and Barnes.[7] The study was carried out at two dose levels, that is, therapeutically equivalent dose (900 mg/kg) and maximum dose, that is, population taking Ghrita as a daily diet article in a large quantity (4140 mg/kg).
Experimental design
The selected animals were kept on acclimatization for 7 days and thereafter they were grouped randomly into 5 groups of 6 animals in each group. The first group served as normal control and second and third groups were administered with Avika Ghrita at 900 mg/kg and 4140 mg/kg doses, respectively. The fourth and fifth groups were administered with Go Ghrita at 900 mg/kg and 4140 mg/kg doses, respectively. Test drugs were administered orally once a day for 45 consecutive days.
The effect on gross behavior was observed once in a week by exposing individually on open arena. The total fecal fat content was estimated at 0, 15, 30, and 45th day. Electrocardiogram (ECG) recording was done on the 43rd day of drug administration after anesthetizing the animals with diethyl ether. ECG was recorded by using a portable ECG machine (Cardiofax, Medicaid Systems, Chandigarh, India). Only the four standard (limb) leads were attached to four extremities of the animals, and the chest leads were not used. The speed of the ECG machine was set to 50 mm/s.
On the 46th day the blood was obtained from the retro-orbital puncture under light ether anesthesia using capillary tubes. The body weight was noted and they were sacrificed by excess dose of ether. Blood samples were collected for assessing different types of biochemical parameters, such as blood urea level,[8] serum creatinine,[9] serum total cholesterol,[10] serum High Density Lipoprotein (HDL) cholesterol,[11] serum triglyceride,[12] serum total protein,[13] serum albumin,[14] serum globulin, serum alkaline phosphatase,[15] Serum Glutamic Oxaloacetic Transminase (SGOT),[16] Serum Glutamic Pyruvic Transminase (SGPT),[17] serum bilirubin (Total and Direct).[18] The important organs, such as heart, liver, aorta, kidney, testis, uterus, and ovary were dissected out, weighed (except aorta) and all organs were fixed in 10% formalin solution. The histopathological slides were prepared by referring the standard procedure.[19] The slides were viewed under binocular research Carl–Zeiss's microscope (Germany) to note down the changes in the microscopic features of the tissues.
Statistical analysis
The obtained data have been presented as Mean ± SEM (Standard Error of Mean), difference between the groups was statistically determined by unpaired Student's t test and analysis of variance (ANOVA) followed by Dunnett's t test for all the treated groups with the level of significance set at P < 0.05. The level of significance was noted and interpreted accordingly.
Results
The gross behavior in rats shows mild hyperactivity in higher doses of Avika Ghrita administered group in comparison to initial values as well as control group. In both the doses of Go Ghrita administered group also mild hyperactivity was observed in comparison with the respective initial values and control group.
In the control group normal progressive gain in body weight was observed. Similarly in both Go Ghrita and Avika Ghrita at both dose-treated groups gain in body weight was observed; however, the observed increase in body weight was found to be statistically insignificant [Table 1]. Regarding the organ weight, out of five organs studied none of the organ weight was significantly affected by the administration of test dugs for 45 days [Table 2].
Table 1.
Effect on body weight

Table 2.
Effect on organ weight

The effect of test drugs on the total fecal fat content is provided in Table 3. Both the test drugs at both dose levels markedly increased the total fecal fat content. However only the observed increase of total fecal fat content of Low Dose of Avika Ghrita (AGLD) and High Dose of Go Ghrita (GGHD) treated groups were found to be statistically significant in comparison with the control group.
Table 3.
Effect on total fecal fat content

In total 13 biochemical parameters, none of the parameters was affected to a significant extent except triglyceride content of AGLD treated group, which was significantly decreased in comparison with the control group [Table 4].
Table 4.
Effect on serum biochemical parameters
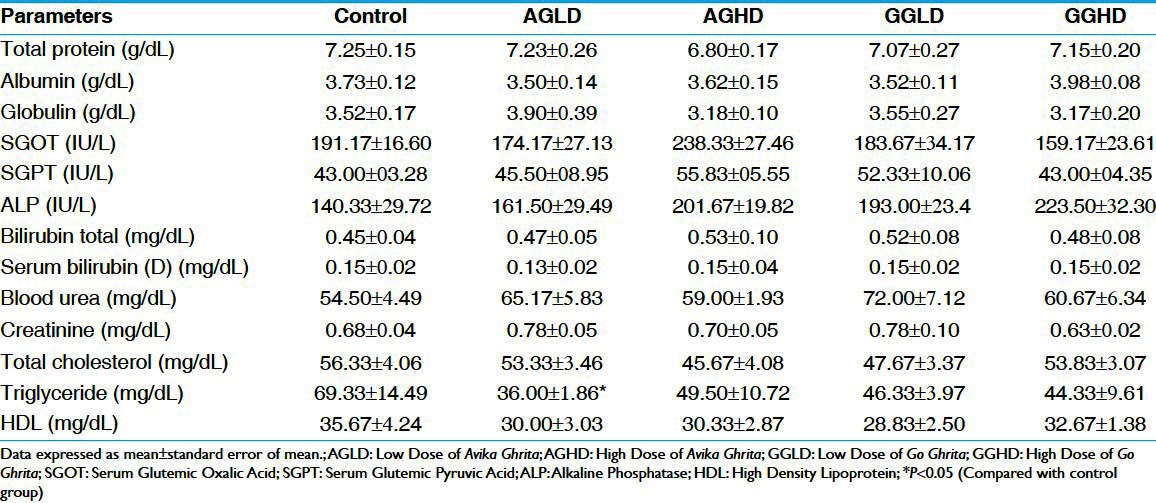
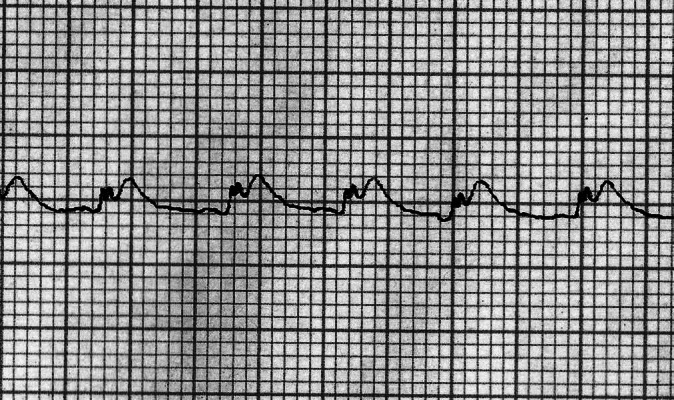
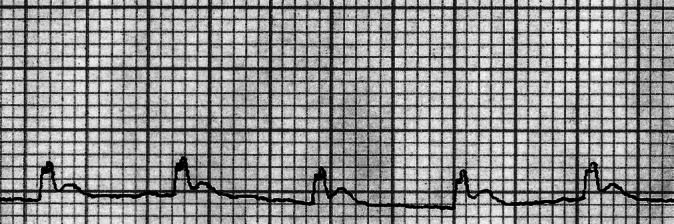
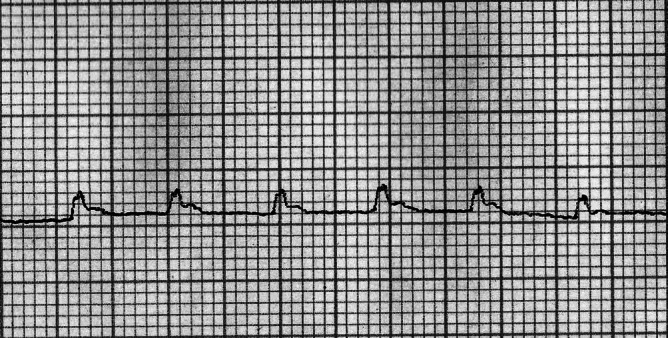
Among the six electro-physiological parameters recorded, Avika Ghrita at both dose levels significantly shortened the PR interval and significantly prolonged QTc at the low-dose level [Table 5, Figures 1, 2]. Treatment with Go Ghrita at both the dose levels did not affect any of the parameters to a significant extent [Figures 3, 4].
Table 5.
Effect on electrocardiography of heart
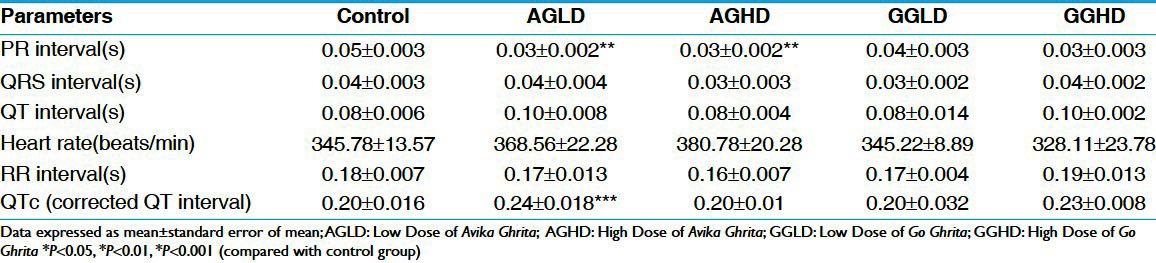
Figure 1.
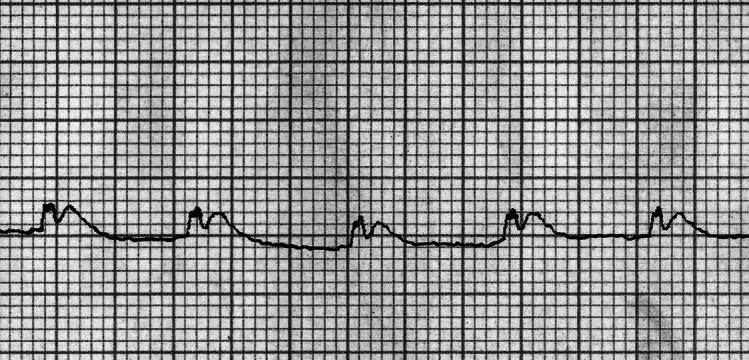
ECG of AGLD, low dose of Avika Ghrita; suggestive of shortened PRinterval
Figure 2.
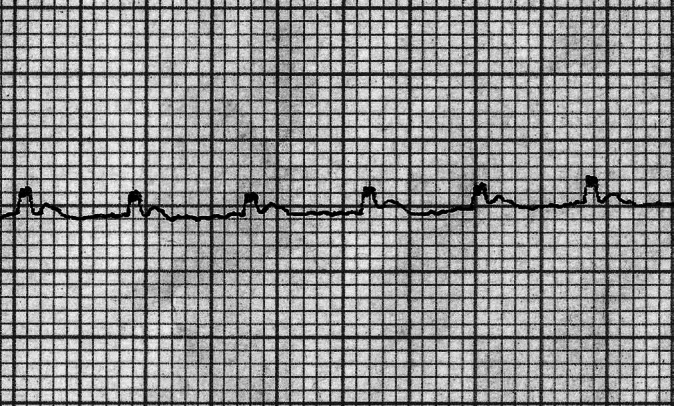
AGHD, high dose of Avika Ghrita; suggestive of shortened PRinterval
Figure 3.
GGLD, low dose of Go Ghrita
Figure 4.
GGHD, high dose of Go Ghrita
Examination of sections of all the seven organs from the control group exhibited normal cytoarchitecture. Examination of sections from Avika Ghrita and Go Ghrita at both dose level treated groups also showed almost normal cytoarchitecture except for mild fatty changes in one or two sections of the liver from these treated groups.
Discussion
Ghee is the elixir for daily life in human beings. In routine dietetics, ghee is advised either in pure form or medicated or mixed with food articles. However, being animal fat, it is the most averted substance by the physicians of modern medicine due to its property of increasing serum cholesterol. On the contrary, according to Ayurveda, Ghrita is a most favored substance, not only as an important medicine in the management of disease but also as an important food ingredient in daily diet. The present study was undertaken to address this controversy by administering it for longer duration at both low and high dose levels to know their effect on various ponderal, biochemical, histopathological, and eleletro-physiological parameters. Further, to know why Acharyas told that Avika Ghrita is inferior and Ahridya, whether it is really having any such deleterious effects or not, this formulation was selected for a comparative study with Go Ghrita. The study was conducted at two doses, namely, low and high dose levels keeping the fact that the dose is used for both therapeutic purpose (clinical dose) and as diet.
As expected, in the control group normal progressive gain in body weight was observed. However, in all the treated groups the observed weight gain was comparatively less. There can be many reasons for the decrease in the body weight. One of them may be interference with the absorption of essential nutrients from the gastrointestinal tract. The second reason may be the increase in the metabolic rate unlinking it from energy formation mechanism (e.g., uncoupling of oxidative phosphorylation) and the third reason may be stimulation of the satiety center in the hypothalamus.
A moderate to significant increase in the fecal fat content was observed in all the four groups. This is obviously due to higher consumptions of ghee part of which might not have been absorbed. Since there was no difference between the two types of ghee it has no bearing on the outcome of the discussion.
Fats or ghee have an inherent property of increasing the serum triglyceride and cholesterol, but in the present study no such thing happened in spite of using quite high level of ghee consumption for a pretty long period of 45 days. On the contrary significant lowering of serum triglyceride observed in AGLD administered group and insignificantly in all other groups may be indicative of interference with the triglyceride formation and utilization in the body. The decrease may be due to interference with the fat absorption in the jejuno-duodenal junction or higher incorporation to Very Low Density Lipoprotein (VLDL) or higher utilization by the tissue.
In comparison with the ECG of control group [Figure 5], PR interval was found to be shortened in Avika Ghrita administered groups [Figure 1, 2]. This interval represents the time the impulse takes to reach the ventricles from the sinus node. Sympathetic activity increase shall lead to decrease and parasympathetic activity increase leads to prolongation of this interval.[20] The PR interval decrease may be indicative of faster transmission of impulse form the atria to the ventricles. It is not known whether any sympathetic stimulation is involved or not.
Figure 5.
ECG of control group
In humans and large animals, QT interval varies strongly and inversely with heart rate. Consequently, in clinical practice and human pharmacologic studies it is typical to correct the measured QT interval for heart rate to obtain measures of QT interval, which are heart rate independent (QTc).[21] A significant prolongation of QTc was observed in AGLD administered group whereas only insignificant prolongation was observed in GGHD administered group [Figures 1, 4]. This shows that both the doses of ghee have cardiac activity modulating potential; however, how exactly it is produced and its implication for clinical conditions needs to be carefully verified.
The mention of Ahridya for Avika Ghrita in classics may be based on the observation of interference with the cardiac function at least in some patients, however, Go Ghrita at higher dose level also has some potential and needs further careful analysis. Furthermore, there were no marked differences between Avika and Go Ghrita. The one remarkable difference could be the observation of QTc prolongation. This may be the basis for the classics to categorize it as Ahridya.
Conclusion
Both Avika and Go Ghrita have the potential to produce both desirable and undesirable effects. Among the desirable effects is non-observation of hyperlipidemia in spite of giving good amount of fat, which is supposed to be of saturated type. The adverse effects are cardiac changes as per the ECG observations. Hence it can be suggested that a person with cardiac and renal problems should better avoid both the ghee.
References
- 1.Maharshi Kashyapa. In: Kashyap Samhita, Khil Sthana 4/5. 5th ed. Shri Satyapal Bhishagacharya., editor. Varanasi: Chaukhambha Sanskrit Sansthana; 1998. p. 249. [Google Scholar]
- 2.Agnivesha . In: Charaka, Dridhabala, Charaka Samhita, Sutra Sthana, Vividha Shitapitiya Adhyaya 28/45. 5th ed. Vaidya Jadavaji Trikamji Acharya., editor. Varanasi: Chaukhamba Surbharti Prakasana; 2008. p. 181. [Google Scholar]
- 3.Vagbhatta . In: Ashtang Hridaya, Sutra Sthana, 5/39. Reprinted ed. Harishastri Paradkar Vaidya., editor. New Delhi: Rashtriya Sanskrit Samsthana; 2002. pp. 73–4. [Google Scholar]
- 4.Ibidem. Ashtang Hridaya, Sutra Sthana, 5/42. :74. [Google Scholar]
- 5.Agnivesha . In: Charaka, Dridhabala, Charaka Samhita, Sutra Sthana, Yajja Purushiya Adhyaya 25/40. 5th ed. Vaidya Jadavaji Trikamji Acharya., editor. Varanasi: Chaukhamba Surbharti Prakasana; 2008. p. 131. [Google Scholar]
- 6.Sharangadhara, Sharangadhara Samhita, Vidyasagar PS., editors. Varanasi: Choukhambha Orientalia; 1983. p. 137, 214. [Google Scholar]
- 7.Paget GE, Barnes JM. Evaluation of drug activities. In: Laurence DR, Bacharach AL, editors. Pharmacometrics. Vol. 1. New York: Academic Press; 1964. p. 161. [Google Scholar]
- 8.Tiffany TD, Janseen JM, Burtis CA, Overton JB, Scott TD. Enzymatic kinetic rate and end point analysis of substrate by use of a GeMSAEC fast analyzer. Clin Chem. 1972;18:829–40. [PubMed] [Google Scholar]
- 9.Slot C. Plasma creatinine determination. A new and specific Jaffe reaction method. Scand J Clin Lab Invest. 1965;17:381–7. doi: 10.3109/00365516509077065. [DOI] [PubMed] [Google Scholar]
- 10.Roschlau P, Bernt E, Gruber W. Enzymatishe Bestimmung des Cesamt-Cholesterins in Serum Z. Clin Chem Clin Biochem. 1974;12:226. [PubMed] [Google Scholar]
- 11.Nauk M, Wiebe D, Warnick G. Rifai, Warnick, Dominiczak, editors. Measurement of High-Density-Lipoprotein Cholesterol. 221-244. Handbook of Lipoprotein testing. (2nd edn) 1970 Quantitative determination of HDL in serum by turbidimetric immunoassay. [Google Scholar]
- 12.Tietz NW, editor. 3rd ed. Philadelphia: WB Saunders; 1995. Clinical guide to laboratory tests; p. 76. [Google Scholar]
- 13.Tietz NW, editor. Philadelphia: WB Saunders; 1986. Text book of Clinical Chemistry; p. 579. [Google Scholar]
- 14.Doumas BT, Arends RL, Pinto PC. Vol. 7. Chicago: Academic Press; 1972. Standard Methods of Clinical Chemistry; pp. 175–89. [Google Scholar]
- 15.Wasif Saif M, Alexander D, Wicox CM. Serum Alkaline Phosphatase Level as a Prognostic Tool in Colorectal Cancer: A Study of 105 patients. J Appl Res. 2005;5:88–95. [PMC free article] [PubMed] [Google Scholar]
- 16.Tietz NW. 3rd ed. Philadelphia, PA: WB Saunders; 1995. Clinical guide to laboratory tests; p. 76. [Google Scholar]
- 17.Burtis CA, Ashwood ER, editors. 3rd ed. Philadelphia: WB Saunders; 1999. Tietz textbook of Clinical Chemisry; p. 1136. [Google Scholar]
- 18.Pearlman FC, Lee RT. Detection and measurement of total bilirubin in serum, with use of surfactants as solubilizing agents. Clin Chem. 1974;20:447–53. [PubMed] [Google Scholar]
- 19.Raghuramulu N, Nair KM, Kalyanasundaram S. Hyderabad, India: National Institute of Nutrition (NIN); 1983. A Manual of Laboratory Techniques; pp. 246–53. [Google Scholar]
- 20.Zipes DP, Miyazaki T. The autonomic nervous system and the heart: Basis for understanding interactions and effects on arrhythmia development. In: Zipes DP, Jalife J, editors. Cardiac Electrophysiology: From Cell to Bedside. Philadelphia: WB Saunders; 1990. pp. 312–30. [Google Scholar]
- 21.Van de Water A, Verheyen J, Xhonneux R, Reneman RS. An improved method to correct the QT interval of the electrocardiogram for changes in heart rate. J Pharmacol Methods. 1989;22:207–17. doi: 10.1016/0160-5402(89)90015-6. [DOI] [PubMed] [Google Scholar]