

Abstract
Background:
This study was designed to identify the incidence, injury patterns, and actual medical costs of occupational-related falls in Qatar, in order to provide a reference for establishing fall prevention guidelines and recommendations.
Settings and Design:
Retrospective database registry review in Level 1 Trauma Center at Tertiary Hospital in Qatar.
Materials and Methods:
During a 12-month period between November 1st 2007 and October 31st 2008, construction workers who fell from height were enrolled. A database was designed to characterize demographics, injury severity score (ISS), total hospital length of stay, resource utilization, and cost of care.
Statistical Analysis:
Data were presented as proportions, mean ± standard deviation or median and range as appropriate. In addition, case fatality rate and cost analysis were obtained from the Biostatistics and finance departments of the same hospital.
Results:
There were 315 fall-related injuries, of which 298 were workplace related. The majority (97%) were male immigrants with mean age of 33 ± 11 years. The most common injuries were to the spine, head, and chest. Mean ISS was 16.4 ± 10. There was total of 29 deaths (17 pre-hospital and 12 in-hospital deaths) for a case fatality rate of 8.6%. Mean cost of care (rounded figures) included pre-hospital services Emergency Medical Services (EMS), trauma resuscitation room, radiology and imaging, operating room, intensive care unit care, hospital ward care, rehabilitation services, and total cost (123, 82, 105, 130, 496, 3048,434, and 4418 thousand United States Dollars (USD), respectively). Mean cost of care per admitted patient was approximately 16,000 USD.
Conclusions:
Falling from height at a construction site is a common cause of trauma that poses a significant financial burden on the health care system. Injury prevention efforts are warranted along with strict regulation and enforcement of occupational laws.
Keywords: Cost of care, falls from height, Qatar, workplace
INTRODUCTION
The incidence of fall-related injuries at construction sites is almost approaching motor vehicle collisions and is a leading cause of death and lasting impairment among patients in Qatar.[1]
Analyses of occupational injuries in other countries have shown that falling from a height is a leading cause of death and serious injury in young males within the workforce. A study of occupational fatalities in Taiwan from 1996 to 1999 showed falls to be the most fatal type of workplace accident, causing 38.2% of fatal injuries among men and 39.2% of fatalities among women. The fatality rate for men was 2.8 per 100,000 workers, and construction workers had the highest incidence of fatal falls compared to other industries.[2] The British Health and Safety Commission estimated the rate of fatal falls in the construction industry at 3.4 per 100,000 workers in 2007-2008. Although there is a decrease in fatalities from previous years, the construction industry still has more fatal falls than any other industry with 31% of all fatal injuries.[3]
Because little is known about the frequency or economic impact of fall-related injuries in developing countries, this study was undertaken to identify the injury burden and the financial losses due to these preventable work-related accidents in the rapidly transforming state of Qatar.
MATERIALS AND METHODS
Data were retrospectively reviewed from the trauma registry at Hamad General Hospital, the only level 1 trauma center in Qatar, for a period of 1 year from November 1, 2007 through October 31, 2008. All patients who sustained workplace-related falls that required hospital admission were included. Although the height of fall in the database was not specified, most patients were reported by the trauma team to have fallen from a height of 3 m or greater. Patients who had fallen and were evaluated in the hospital and discharged from the emergency Department were excluded from this study. Data provided by the mortuary for the same 1-year period were also included for purpose of estimating workplace-related fall causing death.
Children < 14 years and women who sustained non-occupational falls were excluded.
We collected the following information from the trauma registry: patients’ sex, age, nationality, Emergency Medical Services (EMS) utilization, injury severity score (ISS), intensive care unit (ICU) and hospital length of stay, rehabilitation length of stay, resource utilization, and mortality. An injury was defined as a positive finding on clinical exam or imaging modalities such as X-ray, computed tomography (CT) scan, or magnetic resonance imaging, these tests were done according to physician discretion. The incidence of various injury patterns, cost of care, and case fatality rate of the study group was determined.
Data from the Labor Force Sample Survey compiled by the Statistics Authority in 2008 were used to estimate the incidence of falls and fatality rate among construction workers in Qatar. This comprehensive survey estimated the size of the country's workforce and characterized it by age, sex, nationality, employment status, educational status, and economic activity. According to the this survey, there were 343434 construction workers in Qatar who were at risk of having a work-related fall injury in 2008.[4]
The finance department at Hamad Medical Center provided hospital costs for various diagnostic tests, operative procedures, hospitalization, and rehabilitation for patients based on their admission diagnosis. Cost per patient was calculated using the data published by our hospital in 2007.[5] These figures included conservative estimates of the hospital cost for all aspects of patient care, including personnel and physical facilities costs. Cost of care could only be determined for patients seen by the trauma service and not for patients brought in by EMS to the mortuary. The cost of care for patients who were evaluated, treated, and discharged from the emergency department could not be calculated as data for these patients were not tracked by the healthcare corporation. Cost of care for patients in the study group was based on pre-hospital EMS utilization, trauma room resuscitation, radiological imaging, ICU length of stay, hospital ward length of stay, number and type of operative interventions, and rehabilitation length of stay.
Data were presented as proportions, mean ± standard deviation or median and range as appropriate. In addition to the case fatality rate and cost analysis through finance department of the same hospital.
RESULTS
Injury burden of falls
There were 315 patients identified from the registry who sustained injuries due to fall from a height during a 1-year period. We excluded 17 non-occupational fall-related injured cases (14 children < 14 years and three women), in addition to another 17 pre-hospital deaths (which were included only in the mortality analysis, as there is no full information regarding their death circumstances), yielding a total of 281 cases. The ages of patients ranged from 17 to 76 with a mean age of 33 ± 11 years and a median age of 32 years. Overall ISS scores ranged from 2 to 66 with a mean ISS of 16.4 ± 10 and a median ISS of 10 [Table 1]. Of the total injured patients in the study group, 293 were expatriate workers. Nepalese, Indians, and Egyptians constituted the majority (55%) of cases.
Table 1.
Patient demography and outcome
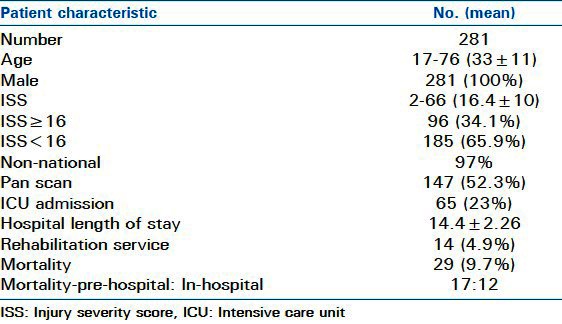
There were total of 29 deaths in the study group for a case fatality rate of 9.7% (17 pre-hospital deaths and 12 in-hospital deaths). All the study subjects who died were mainly expatriate workers. Injuries by location are described in Figure 1. The most common injuries were spine (any combination of cervical, thoracic, and/or lumbar spine injury), head, and chest. The mean length of stay for patients admitted to the trauma service during the study period was 14.4 ± 2.26 days, with a median length of stay of 8 days.
Figure 1.
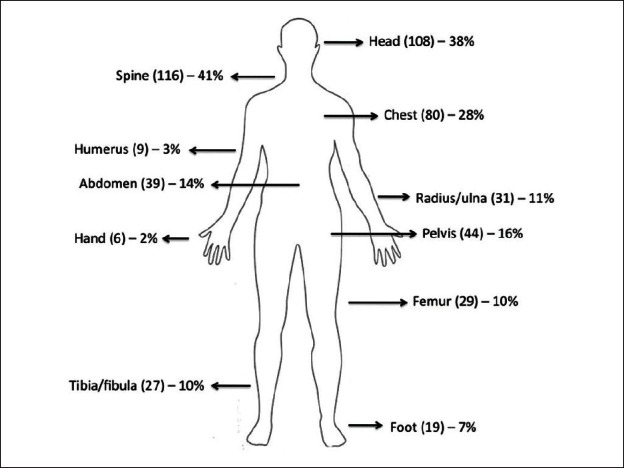
Injuries by body region
The incidence of fall injuries evaluated by the trauma service team at Hamad General Hospital during the study period was 298/343,434 or 86.7 per 100,000 workers. The death rate for construction workers due to fall injuries was 29/343,434 or 8.44 per 100,000 workers. Hospital costs for patient care are shown in Figure 2. The total cost in US dollars during the 1-year period was $4,421,507 with a mean cost of $15,735 per patient; as a reference to this number, each day in the ICU costs about $1500. Knowing that Hamad Hospital is governmental funded body, this amount poses a significant impact on the health financial system in Qatar.
Figure 2.
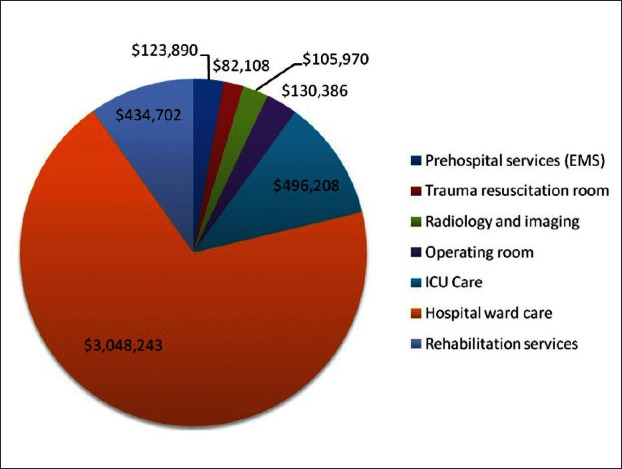
Hospital costs for patient care
DISCUSSION
There is limited information regarding the facts and figures of fall-related injuries in the developing countries like Qatar with its rapid socioeconomic changes and construction boom. Moreover, little is known regarding the risk, safety precautions, training, and experience of fall-related injuries among expatriate workforce. Our results demonstrate a high incidence and fatality rate of fall-related injuries, resulting in high cost of health care.
As Hamad General Hospital has the only level 1 trauma center in the state of Qatar, it receives the most seriously injured patients. The number of patients transported to other smaller private hospitals was unknown, but we would expect them to have low severity of injuries. Moreover, it may be the case that people who fall at work without obvious injury or without losing consciousness do not seek medical care at hospitals. Also, patients who were treated and discharged by the emergency department were not recorded by the trauma registry and therefore, not studied. This makes the incidence of occupation-related fall injuries underestimated.
A prior study by the Primary Health Care Department in Qatar found that fall from a height is the most common cause of work-related injury, affecting 75% of expatriate, male construction workers.[6] It also demonstrated that these patients had significant hospital lengths of stay. Hamad General Hospital is a public hospital and therefore these work-related injuries pose a significant financial burden on the government expenditure. Other costs, such as the cost to replace these workers or costs associated with death or disability from injury were not considered. Also, pre-hospital and hospital costs for the 17 patients who were brought in dead by EMS directly to the mortuary were not included in the cost analysis. Thus, the estimated cost in this report is likely an underestimate of the true cost of work-related falls.
The case fatality rate of falls is approximately 8.6% which is higher than rates described among developed nations. An Australian study describing falls over a 3-year period reported a case fatality rate of around 4.6%, which is higher than data reported previously in Australia. However, contrary to our findings, most of their deaths were falls at home and not in the workplace.[7] Data from the USA determined the case fatality rate for falls from a height to be 3.3% among elderly patients more than 75 years of age, and which was the highest case fatality rate reported among all age groups.[8] The case fatality for subjects aged 21-35 years (similar to the age group of our study population) in the US study was 1%, which was considerably lower than in our subjects.[7] Our study included only patients who were seen by the trauma service team requiring admission. They appear to be more severely injured than those reported by the earlier studies and this may in part explain unfavorable prognosis in Qatar compared to western countries. The incidence of fall injuries in our study group was 86.7/100,000 workers with a death rate of 8.67/100,000 workers. According to the United States Bureau of Labor Statistics, the rate of fatal injuries for workers in the USA in 2007 was 3.7/100,000 workers.[9] Though work-related fall injuries are generally viewed as preventable, an effective fall prevention program in Qatar will not only save lives but possibly can reduce the financial burden on healthcare expenditure of the country. This needs more investigation to study the actual cost of any fall prevention program in Qatar. It should be noted that when many of these expatriate workers with debilitating injuries are medically stable, they often return back to their home country, creating a burden to their family members who must care for their activities of daily living.
In this study, there were a high number of injuries affecting head and spine, and a comparatively low number of injuries to the lower extremities. This suggests that injured workers are falling mainly on their heads. The implementation of helmets or other protective headgear and safety barriers or restraint devices for construction workers at risk of falling may lead to significant reduction of injuries.
Surprisingly, there is not much literature available to support injury prevention programs in the workplace.[10] Despite this lack of evidence, prevention programs are instituted at construction worksites in the hopes of reducing the likelihood of injuries. For an effective program to be instituted in Qatar, risk factors need to be determined which are responsible for the high case fatality associated with workplace-related fall injuries. Some hypothesized causes for the high morbidity and mortality from falls include:
Lack of construction work experience among migrant workers
Language barriers for migrant workers
Lack of training programs for fall prevention prior to employment
Lack of physical safety features at construction sites, such as guardrails, warning signs, or safety equipment
Lack of motivation for companies to improve safety in the workplace
Lack of legislative oversight at construction sites.
Unfortunately, there is limited evidence that a multifaceted injury prevention program can be effective in reducing work-related injuries.[11] Nonetheless, efforts that have been implemented in other countries include primary prevention measures such as fixed barriers (handrails and guardrails), surface opening protections (hole coverings), crawling boards/planks, and strong roofing materials. Secondary protection measures would include fall arrest systems (safety harnesses) and fall containment systems (safety nets).[12] Work sites should be audited to assure that the implemented safety measures are being utilized and data on fall injury patients seen by the trauma service should continue to be maintained to track case fatality rates. This report provides a reference point for how much the injury cost and potentially providing a basis for discussion of how significant the problem is with the government. Any proposed interventions will not be free; however, the anticipated savings of cost possibly will offset the cost of a fall prevention program over time.[13]
Surveillance of occupation-related fall injuries should continue in Qatar to improve the safety at workplace. From the administrative point of view, Cabinet Resolution No (16) in 2011 has been issued and established the National Committee of Occupational Health and Safety at the Ministry of Labor. The Committee comprise of representatives from various ministries to propose a national policy and system for occupational health and safety devise, revise the occupational health and safety rules and regulations, and propose the mechanisms in respect of enforcing compliance with health and safety rules and regulations.
CONCLUSION
Falls from height at construction sites are a common cause of trauma, leading to high mortality and pose a financial burden on the healthcare system in Qatar. Injury prevention efforts directed at reducing the risk of falls from construction sites are needed to minimize both the fall-related injuries and possibly costs. For most effective safety measures, an evidence-based determination of the risk factors and safety measures for occupation-related falls should be implemented.
ACKNOWLEDGMENT
We would like to thank Mr. Mohammed Ali, Head of Costing for his great efforts in calculating the cost of service at Hamad Medical Corporation. This study was approved by Medical Research Center, Institutional Review Board (IRB #8229/08), HMC, Qatar. This study was presented at the Annual Meeting, Trauma Association of Canada, May 6, 2010, Halifax, Nova Scotia.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.El-Faramawy A, El-Menyar A, Zarour A, Maull K, Riebe J, Kumar K, et al. Presentation and outcome of traumatic spinal fractures. J Emerg Trauma Shock. 2012;4:316–20. doi: 10.4103/0974-2700.102381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lin YH, Chen CY, Luo JL. Gender and age distribution of occupational fatalities in Taiwan. Accid Anal Prev. 2008;40:1604–10. doi: 10.1016/j.aap.2008.04.008. [DOI] [PubMed] [Google Scholar]
- 3.Health and Safety Executive. Work-related injuries and ill health in construction: Injuries, 2009. [Last accessed on 2009 Mar 25]. Available from: http://www.hse.gov.uk/statistics/industry/construction/injuries.htm .
- 4.Statistics Authority. Labor force sample survey, 2009, State of Qatar. [Last accessed on 2009 Mar]. Available from: http://www.qsa.gov.qa/eng/surveys/labour_force_survey_jul_2009.xls .
- 5.Hamad Medical Corporation Finance Department. Cost of services provided at HMC. (1st ed) 2007 [Google Scholar]
- 6.James B. Fall from height is most common work injury. Gulf Times. 2008. [Last accessed on 2009 Mar 4]. Available from: http://www.gulf-times.com/site/topics/article.asp?cu_no=2&item_no=252885&version=1&template_id=36&parent_id=16 .
- 7.Kent A, Pearce A. Review of morbidity and mortality associated with falls from heights among patients presenting to a major trauma centre. Emerg Med Australas. 2006;18:23–30. doi: 10.1111/j.1742-6723.2006.00800.x. [DOI] [PubMed] [Google Scholar]
- 8.Diggs BS, Lenfesty B, Arthur M, Hedges JR, Newgard CD, Mullins RJ. The incidence and burden of ladder, structure, and scaffolding falls. Acad Emerg Med. 2005;12:267–70. doi: 10.1197/j.aem.2004.10.028. [DOI] [PubMed] [Google Scholar]
- 9.U.S. Bureau of Labor Statistics. U.S. Department of Labor, Current Population Survey, Census of Fatal Occupational Injuries, U.S. Bureau of the Census, and US Department of Defense. 2008. [Last accessed on 2009 Apr 2]. Available from: http://www.bls.gov/iif/oshcfoi1.htm#2007 .
- 10.Van der Molen HF, Lehtola MM, Lappalainen J, Hoonakker PL, Hsiao H, Haslam R, et al. Interventions for preventing injuries in the construction industry. Cochrane Database Syst Rev. 2007:CD006251. doi: 10.1002/14651858.CD006251.pub2. [DOI] [PubMed] [Google Scholar]
- 11.Lehtola MM, van der Molen HF, Lappalainen J, Hoonakker PL, Hsiao H, Haslam RA, et al. The effectiveness of interventions for preventing injuries in the construction industry: A systematic review. Am J Prev Med. 2008;35:77–85. doi: 10.1016/j.amepre.2008.03.030. [DOI] [PubMed] [Google Scholar]
- 12.Chi CF, Chang TC, Ting HI. Accident patterns and prevention measures for fatal occupational falls in the construction industry. Appl Ergon. 2005;36:391–400. doi: 10.1016/j.apergo.2004.09.011. [DOI] [PubMed] [Google Scholar]
- 13.Hoonakker P, Loushine T, Carayon P, Kallman J, Kapp A, Smith MJ. The effect of safety initiatives on safety performance: A longitudinal study. Appl Ergon. 2005;36:461–9. doi: 10.1016/j.apergo.2004.07.006. [DOI] [PubMed] [Google Scholar]