

Abstract
We describe here three patients with the Alzheimer's Disease (AD) whose behavioral symptoms were improved remarkably as a result of the turmeric treatment, which is the traditional Indian medicine. Their cognitive decline and Behavioral and Psychological Symptoms of Dementia (BPSD) were very severe. All three patients exhibited irritability, agitation, anxiety, and apathy, two patients suffer from urinary incontinence and wonderings. They were prescribed turmeric powder capsules and started recovering from these symptoms without any adverse reaction in the clinical symptom and laboratory data. After 12 weeks of the treatment, total score of the Neuro-Psychiatric Inventory-brief questionnaire decreased significantly in both acuity of symptoms and burden of caregivers. In one case, the Mini-Mental State Examination (MMSE) score was up five points, from 12/30 to 17/30. In the other two cases, no significant change was seen in the MMSE; however, they came to recognize their family within 1 year treatment. All cases have been taking turmeric for more than 1 year, re-exacerbation of BPSD was not seen. The present cases suggest a significant improvement of the behavioral symptoms in the AD with the turmeric treatment, leading to probable benefit of the use of turmeric in individuals with the AD with BPSD.
Keywords: Alzheimer's disease, behavioral and psychological symptoms of dementia, curcumin, mini-mental state examination, neuropsychiatric inventory-brief questionnaire, turmeric
Introduction
Alzheimer's disease (AD) is the most common form of dementia and it is characterized by the progressive cognitive impairment. The behavioral and psychological symptoms of the dementia (BPSD) are also commonly seen in patients with AD, such as hallucinations, delusions, apathy, depression, agitation, irritability, and wandering. These symptoms can have serious harmful effects on patients’ Quality of Life (QOL) and are also a burden to caregivers and increasing the costs of care.[1] Therefore, the treatment of BPSD is as important as that of core symptom such as memory disturbance and disorientation. Acetylcholinesterase (AChE) inhibitors and N-Methyl-d-Aspartate (NMDA) receptor uncompetitive antagonist (memantin hydrochloride) are commonly used for the treatment of AD. They are effective in core symptoms and BPSD treatment;[2–4] however, the effects are not completely satisfactory. They can cause adverse effects such as nausea, extra-pyramidal symptoms, drowsiness, and the other symptoms.
Neuropathologically, AD is characterized by the presence of senile plaques, neurofibrillary tangles, persistent neuronal loss, although, the neurotoxic mechanisms have not been completely elucidated. It is clear that both oxidative stress and inflammation play a key role in the illness. Recent reports have suggested therapeutic potential of curcumin in the pathophysiology of AD, because of its antioxidant, anti-inflammatory, and anti-amyloid effects.[5–11] Curcumin is a polyphenolic molecule extracted from turmeric, the spice consisting of the powdered rhizome of the plant Curcuma longa Linn. Turmeric contains about 5% curcumin, which gives the spice its yellow color and is used widely as yellow food coloring. It has also a medical history that date back 5000 years. It has been extensively used to treat various ailments for centuries in Ayurveda, the traditional Indian system of medicine, such as arthritis, gastric ulcer, jaundice, fever, liver disease, urinary tract disease, skin disease, and as a “blood purifier.”[12] Many pharmacological studies have been conducted to describe the multiple biological actions of curcumin. Curcumin has also demonstrated neuroprotective effects in animal models of not only AD;[13] however, also Parkinson's disease,[14–16] depression,[17–19] epilepsy,[20] and so on. Epidemiological studies in India, a country where turmeric consumption is widespread, suggest that it has one of the lowest prevalence rates of AD in the world.[21,22] In spite of the high efficacy and safety, curcumin has not yet been approved as a therapeutic agent. Here, we present three cases with the AD whose behavioral symptoms and ability perform Activities of Daily Living (ADL) were improved by turmeric treatment without any adverse effects.
Case Reports
Case 1
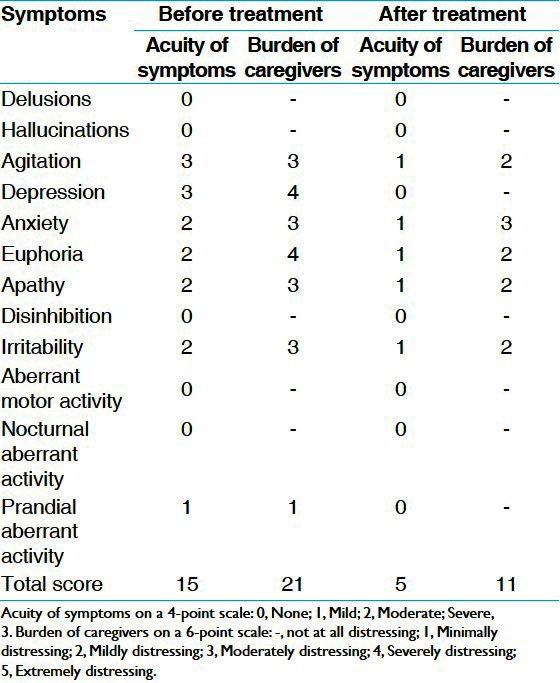
The patient was an 83-year-old female who developed progressive dementia. She had started to exhibit disturbances of short-term memory and orientation, when she was 76 years old. There was no past history of diabetes mellitus, hypertension, dyslipidemia, and head injury. The medical family history was unremarkable. She also had difficulty in learning new information. Gradually, her daily activity was disturbed. She had increasing difficulty in getting dressed, cooking, and coordination household tasks. She wandered aimlessly around the house, had incontinence of urine. She had some psychobehavioral changes, such as apathy, anxiety, agitation, and irritability. She required the presence of caregiver, though she was prescribed AChE inhibitor (donepezil 10 mg) and Yokukansan, which is a traditional Japanese medicine (Kampo). When she was 83 years old, she scored on 1/30 her Mini-Mental State Examination (MMSE), which was used for evaluation of cognitive functions. Her physical examination was largely normal. There were no pyramidal or extra-pyramidal signs. Findings on laboratory tests were normal. Cerebral Magnetic Resonance Imaging (MRI) demonstrated symmetrical bilateral temporal atrophy. After turmeric 764 mg/day (curcumin 100 mg/day) treatment for 12 weeks, both scores of acuity of symptoms and burden of caregivers were decreased by the Japanese version of neuropsychiatric inventory-brief questionnaire (NPI-Q) [Table 1, Figures 1 and 2]. Among the NPI-Q subscales, her agitation, apathy, anxiety, and irritability were relieved. She began to tell about the need to urinate. Furthermore, she came to join in the laughter watching TV comedy program, began to sing some songs and do knitting, which she used to do. After taking turmeric for more than 1 year, she came to recognize her family, and seem to remind her late husband and she lives a peaceful life without a significant BPSD.
Table 1.
Change in the score of the Neuropsychiatric Inventory-Brief Questionnaire before and after turmeric treatment in patient with Alzheimer's disease (Case 1)
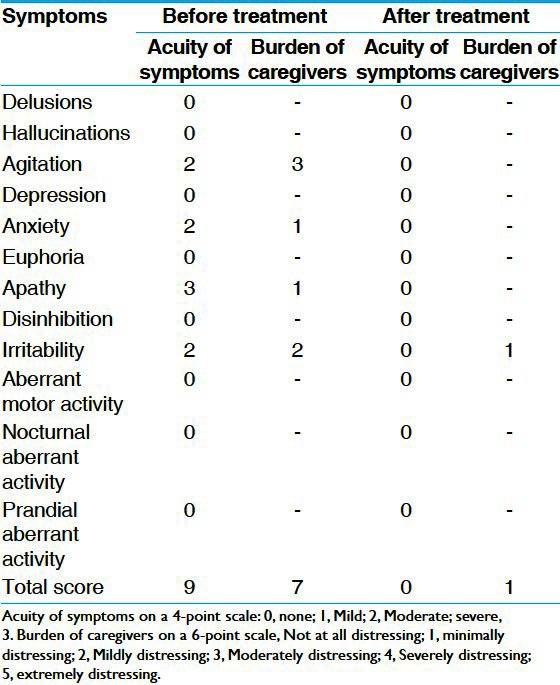
Figure 1.
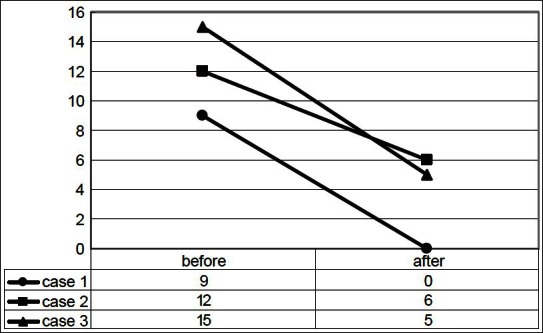
Change in the total score of acuity of symptoms on the neuropsychiatric inventory-brief questionnaire before and after turmeric treatment of three patients with Alzheimer's disease
Figure 2.
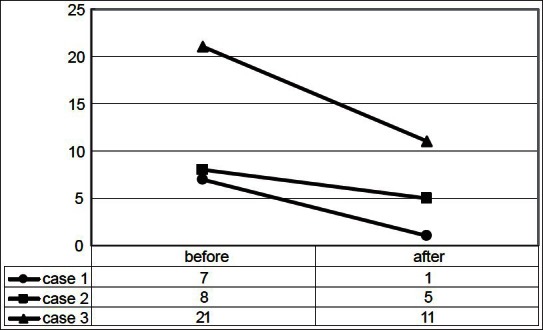
Change in the total score of burden of caregivers on the neuropsychiatric inventory-brief questionnaire before and after turmeric treatment of three patients with Alzheimer's disease
Case 2
An 84-year-old female presented at our hospital with the purpose of taking medical advice for progressive dementia. Her symptoms were forgetfulness, disorientation to place and time, hallucination, delusion, agitation, irritability, depression, apathy, confabulation, wandering, and incontinence of urine, which developed several years prior to presentation. She had a history of hypertension. There was no family history of dementia. She was a non-smoker and drank little alcohol. Her physical examination and her laboratory data, including hematograms, biochemistry, and urinalysis were largely normal. At the time of her initial visit, her cognitive decline was already very severe and her MMSE score was 0/30. On cerebral MRI revealed moderate bilateral temporal atrophy with the mild ventricular dilation. AChE inhibitor (donepezil) could not use because of the side-effects. Her BPSD, including agitation, irritability, and anxiety was not improved, though she was prescribed Yokukansan and atypical antipsychotic drugs. We began to administer turmeric 764 mg/day (curcumin 100 mg/day) to her. She gradually calmed down. Her BPSD, which were hallucination, delusion, depression, agitation, apathy, anxiety, and irritability, were relieved. She stopped urinating outside the front door. She came to put on her clothes properly, and distinguish her family from staffs of the care center. After 12 weeks, judging from the Japanese version of NPI-Q, both acuity of BPSD and burden of caregivers were relieved [Table 2, Figures 1 and 2]. She has been taking turmeric for more than 1 year; she lives in a peacefully serene manner with her family.
Table 2.
Change in the score of the Neuropsychiatric Inventory-Brief Questionnaire before and after turmeric treatment in patient with Alzheimer's disease (Case 2)
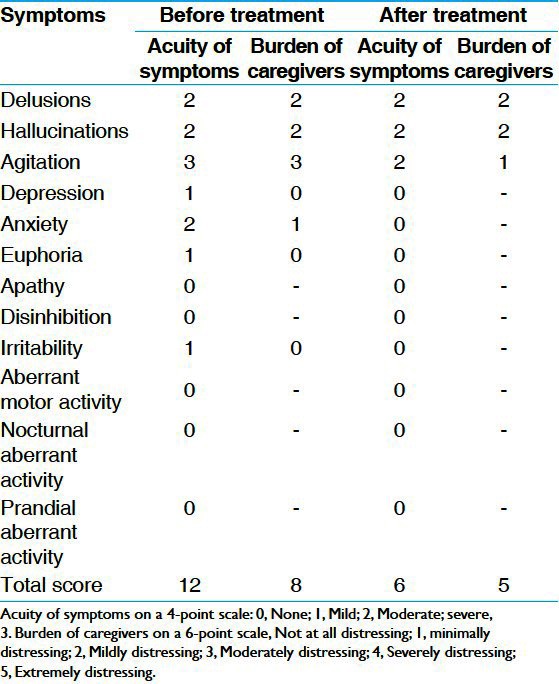
Case 3
A 79-year-old male patient presented at our hospital accompanied by his wife. She reported that the short-term memory loss gradually developed over several years, though he was already prescribed AChE inhibitor (donepezil 5 mg) by his previous doctor for 3 years. He wanted to stay at home, and lived an idle life. He stopped painting in oils, which he used to do for his hobby. He had a history of hypertension being treated with losartan potassium. The medical family history was insignificant. His physical examination was normal. Routine blood tests were normal, including thyroid function, serum vitamin B1, B12, and folic acid. Cerebral MRI demonstrated mild bilateral temporal atrophy with mild ischemic changes in deep white matter. Single-Photon Emission Computed Tomography showed typical AD pattern, which means perfusion in the temporal, parietal, and posterior cingulated is significantly decreased. His MMSE score was 12/30, with poor orientation to place and time, calculation, concentration, recall, transcription of the figure, spontaneous writing, and verbal fluency. His BPSD was agitation, depression, apathy, anxiety, euphoria, aberrant eating behavior, and irritability. Turmeric 764 mg/day (curcumin 100 mg/day) treatment for 12 weeks relieved the patient's BPDS, especially agitation, irritability, and depression. Both scores of acuity of symptoms and burden of the caregivers were decreased in the Japanese version of the NPI-Q [Table 3, Figures 1 and 2]. His MMSE score was up five points, 17/30, improving calculation, concentration, transcription of the figure, and spontaneous writing. He has been taking turmeric for more than 1 year; he lives calmly with his wife.
Table 3.
Change in the score of the Neuropsychiatric Inventory-Brief Questionnaire before and after turmeric treatment in patient with Alzheimer's disease (Case 3)
Discussion
Here, we reported three cases of the AD whose BPSD were a significantly improved by the turmeric treatment, evaluated by the NPI-Q. The NPI-Q is a brief, reliable, and the clinical rating instrument that evaluates the neuronpsychiatric symptoms in demented patients and associated caregiver distress, and the effects of pharmacological treatment on these symptoms and caregivers’ distress.[23] Therefore, in this study, we evaluate using the NPI-Q confirmed that turmeric treatment improved the behavioral symptoms associated with AD. The present study found that the turmeric was effective for the treatment of several BPSD, including delusions, hallucination, apathy, agitation, anxiety, irritability, and depression. In all cases, total score of the NPI-Q decreased significantly in both acuity of symptoms and burden of caregivers. Clinical improvements were gradually observed within 12 weeks of turmeric administration. And their caregivers were released from the associated distress. In case 1 and case 3 patients, donepezil was being administered for several years before starting the turmeric treatment, and the effect of donepezil on BPSD may therefore already had reached a stable state. Turmeric did further decrease the NPI-Q score, already decreased by donepezil.
BPSD can impair the QOL in the patient and also their caregiver. There is a positive correlation between severity of BPSD and care burden, and treatment of BPSD is as important as that of core symptoms.[24] AChE inhibitors,[2,4] NMDA receptor uncompetitive antagonist (memantin),[3] and antipsychotic drugs are effective in BPSD treatment; however, the effects are not completely satisfactory. In particular, antipsychotic drugs can cause adverse effects such as drug-induced extrapyramidal symptoms, drowsiness, gait disturbance, and other symptoms and can result in a decrease on patients’ ADL and QOL. In contrast, there were no adverse effects or significant change in laboratory data in our cases during the turmeric treatment. Based on these results, turmeric treatment in AD is safer than other pharmacological treatments and useful for patients, and that it can possibly reduce the doses of antipsychotics required for the treatment of BPSD.
BPSD occur in 50-90% of AD patient, and an imbalance between the different neurotransmitters, such as serotonin, dopamine, glutamine, acetylcholine, and norepinephrine are related to the pathophysiology of BPSD in AD.[25,26] Curcumin, a major active component of turmeric possesses some interesting properties. Curcumin modulate the levels of norepinephrine, dopamine, and serotonin in the brain,[18,19] and inhibit of Mono-Amine Oxidase (MAO)-A and MAO-B enzyme, the enzyme that decomposes dopamine and serotonin.[18] Dopamine is involved in pleasure, emotion, and regulating locomotion while serotonin has a major role to play in neurovegetative functions of the body, such as appetite, sleep, memory and learning, temperature regulation, mood, behavior, cardiovascular functions, muscle contraction, and endocrine regulation. Norepinephrine is a neurotransmitter involved in attentiveness, emotions, sleeping, dreaming, and learning. We speculate that turmeric significantly reduces behavioral symptoms of AD patients by modifying these neurotransmitters’ dysfunction.
Mounting reports have suggested preventive and/or therapeutic potential of cur cumin and other products from turmeric in the pathophysiology of AD, such as the Amydoid-β (Aβ) cascade, tau phosphorylation, neuroinflammation, or oxidative stress. Several studies have shown that the curcumin are powerful antioxidants, and possess strong anti-inflammatory activity.[7,27] In vitro studies have shown that curcumin attenuates inflammatory response of brain microglial cells,[28] and inhibits the formation of Aβ oligomers and fibrils.[10,11] Aβ oligomers are highly toxic, and viewed as playing an important role in AD pathology.[29,30] In vivo study shows that curcumin can reverse neuritic abnormalities resulting from Aβ production.[8] In transgenic mice model of AD studies, curcumin prevents neuronal damage in the brain,[31] and directly binds small Aβ species to block aggregation and fibril formation.[11] Another study using a transgenic mouse has shown that dietary curcumin significantly lowered oxidized proteins and interleukin-1β, a proinflammatory cytokine in the neuroinflammatory cascades involved in neuritic plaque formation in the brain.[9] And this study also showed that with the curcumin treatment, the astrocytic marker Glial Fibrillary Acidic Protein (GFAP) was reduced, and insoluble and soluble Aβ and plaque burden were significantly decreased by 43-50%.
For the treatment of AD, AChE inhibitors and NMDA receptor uncompetitive antagonist (memantin) are commonly used. Curcumin possess pronounced AChE inhibitory activity in the frontal cortex and hippocampus of AD in experimental animals,[32] and protect against NMDA-induced toxicity in vitro study.[33] Furthermore, curcumin has been reported to increase choline acetyl transferase (ChAT) activity, a synthesizing enzyme for acetylcholine, in the hippocampus of AD model rat.[34] It has been reported that curcumin can be effective in preventing and suppressing cognitive impairment on the grounds that it possess antioxidative, anti-neuroinflammatory effects, and modulate cholinergic system.[35,36] Epidemiological study showed that increased consumption of curry, which usually contain turmeric, is associated with better cognitive performance in non-demented subjects.[37] However, in a clinical trial in China, 34 patients with probable or possible AD randomized to 4 g (10.9 mmol), 1 g (2.7 mmol), 0 g of turmeric once daily showed no significant differences in changes MMSE score or plasma Aβ40 levels between 0 and 6 months.[38] In our report, one patient improved his MMSE score. In the other two cases, their cognitive declines were too severe to take MMSE; however, they came to recognize their family. The improvement of their cognitive function might be due to the activation of the ChAT and the AChE inhibiter, and/or stabilization of the patient's mental status by turmeric.
We conclude that turmeric treatment adding to the routine therapy increase the QOL and ADL of patients and ease caregivers’ burden. This is the first case report demonstrating that turmeric is an effective and safe drug for the treatment of the BPSD in AD patients and that it might impair cognitive function.
Acknowledgments
We would like to gratefully acknowledgment the KANEHIDE BIO Co., LTD., for providing us turmeric.
References
- 1.Beeri MS, Werner P, Davidson M, Noy S. The cost of behavioral and psychological symptoms of dementia (BPSD) in community dwelling Alzheimer's disease patients. Int J Geriatr Psychiatry. 2002;17:403–8. doi: 10.1002/gps.490. [DOI] [PubMed] [Google Scholar]
- 2.Gauthier S, Feldman H, Hecker J, Vellas B, Ames D, Subbiah P, et al. Efficacy of donepezil on behavioral symptoms in patients with moderate to severe Alzheimer's disease. Int Psychogeriatr. 2002;14:389–404. doi: 10.1017/s104161020200858x. [DOI] [PubMed] [Google Scholar]
- 3.Maidment ID, Fox CG, Boustani M, Rodriguez J, Brown RC, Katona CL. Efficacy of memantine on behavioral and psychological symptoms related to dementia: A systematic meta-analysis. Ann Pharmacother. 2008;42:32–8. doi: 10.1345/aph.1K372. [DOI] [PubMed] [Google Scholar]
- 4.Paleacu D, Mazeh D, Mirecki I, Even M, Barak Y. Donepezil for the treatment of behavioral symptoms in patients with Alzheimer's disease. Clin Neuropharmacol. 2002;25:313–7. doi: 10.1097/00002826-200211000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Balasubramanian K. Molecular orbital basis for yellow curry spice curcumin's prevention of Alzheimer's disease. J Agric Food Chem. 2006;54:3512–20. doi: 10.1021/jf0603533. [DOI] [PubMed] [Google Scholar]
- 6.Cole GM, Lim GP, Yang F, Teter B, Begum A, Ma Q, et al. Prevention of Alzheimer's disease: Omega-3 fatty acid and phenolic anti-oxidant interventions. Neurobiol Aging. 2005;26(Suppl 1):133–6. doi: 10.1016/j.neurobiolaging.2005.09.005. [DOI] [PubMed] [Google Scholar]
- 7.Cole GM, Morihara T, Lim GP, Yang F, Begum A, Frautschy SA. NSAID and antioxidant prevention of Alzheimer's disease: Lessons from in vitro and animal models. Ann N Y Acad Sci. 2004;1035:68–84. doi: 10.1196/annals.1332.005. [DOI] [PubMed] [Google Scholar]
- 8.Garcia-Alloza M, Borrelli LA, Rozkalne A, Hyman BT, Bacskai BJ. Curcumin labels amyloid pathology in vivo, disrupts existing plaques, and partially restores distorted neurites in an Alzheimer mouse model. J Neurochem. 2007;102:1095–104. doi: 10.1111/j.1471-4159.2007.04613.x. [DOI] [PubMed] [Google Scholar]
- 9.Lim GP, Chu T, Yang F, Beech W, Frautschy SA, Cole GM. The curry spice curcumin reduces oxidative damage and amyloid pathology in an Alzheimer transgenic mouse. J Neurosci. 2001;21:8370–7. doi: 10.1523/JNEUROSCI.21-21-08370.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ono K, Hasegawa K, Naiki H, Yamada M. Curcumin has potent anti-amyloidogenic effects for Alzheimer's beta-amyloid fibrils in vitro. J Neurosci Res. 2004;75:742–50. doi: 10.1002/jnr.20025. [DOI] [PubMed] [Google Scholar]
- 11.Yang F, Lim GP, Begum AN, Ubeda OJ, Simmons MR, Ambegaokar SS, et al. Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo. J Biol Chem. 2005;280:5892–901. doi: 10.1074/jbc.M404751200. [DOI] [PubMed] [Google Scholar]
- 12.Hatcher H, Planalp R, Cho J, Torti FM, Torti SV. Curcumin: From ancient medicine to current clinical trials. Cell Mol Life Sci. 2008;65:1631–52. doi: 10.1007/s00018-008-7452-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hamaguchi T, Ono K, Yamada M. REVIEW: Curcumin and Alzheimer's disease. CNS Neurosci Ther. 2010;16:285–97. doi: 10.1111/j.1755-5949.2010.00147.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jagatha B, Mythri RB, Vali S, Bharath MM. Curcumin treatment alleviates the effects of glutathione depletion in vitro and in vivo: Therapeutic implications for Parkinson's disease explained via in silico studies. Free Radic Biol Med. 2008;44:907–17. doi: 10.1016/j.freeradbiomed.2007.11.011. [DOI] [PubMed] [Google Scholar]
- 15.Mythri RB, Bharath MM. Curcumin: A potential neuroprotective agent in Parkinson's disease. Curr Pharm Des. 2012;18:91–9. doi: 10.2174/138161212798918995. [DOI] [PubMed] [Google Scholar]
- 16.Rajeswari A, Sabesan M. Inhibition of monoamine oxidase-B by the polyphenolic compound, curcumin and its metabolite tetrahydrocurcumin, in a model of Parkinson's disease induced by MPTP neurodegeneration in mice. Inflammopharmacology. 2008;16:96–9. doi: 10.1007/s10787-007-1614-0. [DOI] [PubMed] [Google Scholar]
- 17.Kulkarni S, Dhir A, Akula KK. Potentials of curcumin as an antidepressant. Scientific World Journal. 2009;9:1233–41. doi: 10.1100/tsw.2009.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kulkarni SK, Bhutani MK, Bishnoi M. Antidepressant activity of curcumin: Involvement of serotonin and dopamine system. Psychopharmacology (Berl) 2008;201:435–42. doi: 10.1007/s00213-008-1300-y. [DOI] [PubMed] [Google Scholar]
- 19.Xu Y, Ku BS, Yao HY, Lin YH, Ma X, Zhang YH, et al. The effects of curcumin on depressive-like behaviors in mice. Eur J Pharmacol. 2005;518:40–6. doi: 10.1016/j.ejphar.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 20.Jyoti A, Sethi P, Sharma D. Curcumin protects against electrobehavioral progression of seizures in the iron-induced experimental model of epileptogenesis. Epilepsy Behav. 2009;14:300–8. doi: 10.1016/j.yebeh.2008.11.011. [DOI] [PubMed] [Google Scholar]
- 21.Chandra V, Pandav R, Dodge HH, Johnston JM, Belle SH, DeKosky ST, et al. Incidence of Alzheimer's disease in a rural community in India: The Indo-US study. Neurology. 2001;57:985–9. doi: 10.1212/wnl.57.6.985. [DOI] [PubMed] [Google Scholar]
- 22.Vas CJ, Pinto C, Panikker D, Noronha S, Deshpande N, Kulkarni L, et al. Prevalence of dementia in an urban Indian population. Int Psychogeriatr. 2001;13:439–50. doi: 10.1017/s1041610201007852. [DOI] [PubMed] [Google Scholar]
- 23.Kaufer DI, Cummings JL, Ketchel P, Smith V, MacMillan A, Shelley T, et al. Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J Neuropsychiatry Clin Neurosci. 2000;12:233–9. doi: 10.1176/jnp.12.2.233. [DOI] [PubMed] [Google Scholar]
- 24.Huang SS, Lee MC, Liao YC, Wang WF, Lai TJ. Caregiver burden associated with behavioral and psychological symptoms of dementia (BPSD) in Taiwanese elderly. Arch Gerontol Geriatr. 2012;55:55–9. doi: 10.1016/j.archger.2011.04.009. [DOI] [PubMed] [Google Scholar]
- 25.Lanari A, Amenta F, Silvestrelli G, Tomassoni D, Parnetti L. Neurotransmitter deficits in behavioural and psychological symptoms of Alzheimer's disease. Mech Ageing Dev. 2006;127:158–65. doi: 10.1016/j.mad.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 26.Lanctôt KL, Herrmann N, Mazzotta P. Role of serotonin in the behavioral and psychological symptoms of dementia. J Neuropsychiatry Clin Neurosci. 2001;13:5–21. doi: 10.1176/jnp.13.1.5. [DOI] [PubMed] [Google Scholar]
- 27.Zhao BL, Li XJ, He RG, Cheng SJ, Xin WJ. Scavenging effect of extracts of green tea and natural antioxidants on active oxygen radicals. Cell Biophys. 1989;14:175–85. doi: 10.1007/BF02797132. [DOI] [PubMed] [Google Scholar]
- 28.Kim HY, Park EJ, Joe EH, Jou I. Curcumin suppresses Janus kinase-STAT inflammatory signaling through activation of Src homology 2 domain-containing tyrosine phosphatase 2 in brain microglia. J Immunol. 2003;171:6072–9. doi: 10.4049/jimmunol.171.11.6072. [DOI] [PubMed] [Google Scholar]
- 29.Selkoe DJ. Alzheimer's disease is a synaptic failure. Science. 2002;298:789–91. doi: 10.1126/science.1074069. [DOI] [PubMed] [Google Scholar]
- 30.Walsh DM, Klyubin I, Fadeeva JV, Cullen WK, Anwyl R, Wolfe MS, et al. Naturally secreted oligomers of amyloid beta protein potently inhibit hippocampal long-term potentiation in vivo. Nature. 2002;416:535–9. doi: 10.1038/416535a. [DOI] [PubMed] [Google Scholar]
- 31.Shukla PK, Khanna VK, Khan MY, Srimal RC. Protective effect of curcumin against lead neurotoxicity in rat. Hum Exp Toxicol. 2003;22:653–8. doi: 10.1191/0960327103ht411oa. [DOI] [PubMed] [Google Scholar]
- 32.Ahmed T, Gilani AH. Inhibitory effect of curcuminoids on acetylcholinesterase activity and attenuation of scopolamine-induced amnesia may explain medicinal use of turmeric in Alzheimer's disease. Pharmacol Biochem Behav. 2009;91:554–9. doi: 10.1016/j.pbb.2008.09.010. [DOI] [PubMed] [Google Scholar]
- 33.Matteucci A, Cammarota R, Paradisi S, Varano M, Balduzzi M, Leo L, et al. Curcumin protects against NMDA-induced toxicity: A possible role for NR2A subunit. Invest Ophthalmol Vis Sci. 2011;52:1070–7. doi: 10.1167/iovs.10-5966. [DOI] [PubMed] [Google Scholar]
- 34.Ishrat T, Hoda MN, Khan MB, Yousuf S, Ahmad M, Khan MM, et al. Amelioration of cognitive deficits and neurodegeneration by curcumin in rat model of sporadic dementia of Alzheimer's type (SDAT) Eur Neuropsychopharmacol. 2009;19:636–47. doi: 10.1016/j.euroneuro.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 35.Awasthi H, Tota S, Hanif K, Nath C, Shukla R. Protective effect of curcumin against intracerebral streptozotocin induced impairment in memory and cerebral blood flow. Life Sci. 2010;86:87–94. doi: 10.1016/j.lfs.2009.11.007. [DOI] [PubMed] [Google Scholar]
- 36.Yadav RS, Chandravanshi LP, Shukla RK, Sankhwar ML, Ansari RW, Shukla PK, et al. Neuroprotective efficacy of curcumin in arsenic induced cholinergic dysfunctions in rats. Neurotoxicology. 2011;32:760–8. doi: 10.1016/j.neuro.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 37.Ng TP, Chiam PC, Lee T, Chua HC, Lim L, Kua EH. Curry consumption and cognitive function in the elderly. Am J Epidemiol. 2006;164:898–906. doi: 10.1093/aje/kwj267. [DOI] [PubMed] [Google Scholar]
- 38.Baum L, Lam CW, Cheung SK, Kwok T, Lui V, Tsoh J, et al. Six-month randomized, placebo-controlled, double-blind, pilot clinical trial of curcumin in patients with Alzheimer disease. J Clin Psychopharmacol. 2008;28:110–3. doi: 10.1097/jcp.0b013e318160862c. [DOI] [PubMed] [Google Scholar]