

Macrodystrophia lipomatosa is a rare cause of congenital gigantism of the limbs; it manifests as disproportionate overgrowth of one or several digits or may even involve the entire limb [1]. This disease is characterized by progressive enlargement of the fibrofatty tissue. There are some case reports on macrodystrophia lipomatosa, but they are limited to cases involving the entire unilateral upper/lower extremities. We present another case of this anomaly limited to the unilateral thumb, index finger, and thenar area, and we highlight the clinical features, differential diagnoses, and the treatment protocol that we followed for this patient.
A 14-year-old boy was referred to us because of excessive growth of his left hand that had enlarged gradually since birth. He had undergone two operations to debulk the lesion. There was no family history suggestive of any other illnesses, and the rest of the patient's history was unremarkable.
The thumb, index finger, and thenar area of the left hand were unusually large, with increases in both the length and thickness of the subcutaneous tissue (Fig. 1). The patient had difficulty in opposing his fingers due to a severely deformed left thumb and index finger. There was no evidence of pitting edema or bruit. He denied pain and other sensory changes. Other physical examinations showed no abnormality.
Fig. 1.

Preoperative photograph. Preoperative photograph showing enlargement of the left thumb and index finger.
Plain radiographs of the patient's left hand revealed a marked increase in the thickness of the soft tissues, and the length and diameter of the corresponding metacarpals and phalanges were also increased. The remaining three ulnar digits appeared normal.
Magnetic resonance imaging (MRI) revealed characteristics of macrodystrophia lipomatosa such as enlargement and marked proliferation of the adipose tissues of the left hand, especially the radial aspect. MRI also demonstrated excessive fibrofatty tissue around the affected digits. This tissue has the same signal characteristics as fat on MRI, that is, low signal intensity T1- and T2-weighted sequences. Furthermore, the density of the excessive adipose tissue seemed to be identical to that of normal subcutaneous fat tissue (Fig. 2).
Fig. 2.

Preoperative magnetic resonance image (MRI). The fibroadipose tissue showing hyperintensity on T1-weighted MRI image. The density of the excessive adipose tissue is identical to that of normal subcutaneous fat tissue.
Based on these imaging findings, the patient was diagnosed with macrodystrophia lipomatosa, and we decided to perform a debulking operation of the thumb and amputation of the index finger at the mid-level of the mid-phalangeal bone (Fig. 3).
Fig. 3.

Postoperative photograph. Postoperative photograph of the operated finger at the 2-month follow-up.
The histopathology showed the presence of abundant fatty tissue infiltrating the dermal connective tissue and a proliferation of subcutaneous nerves. It also showed fine, mesh-like fibrous tissue (Fig. 4). A definite diagnosis of macrodystrophia lipomatosa was made based on these findings.
Fig. 4.
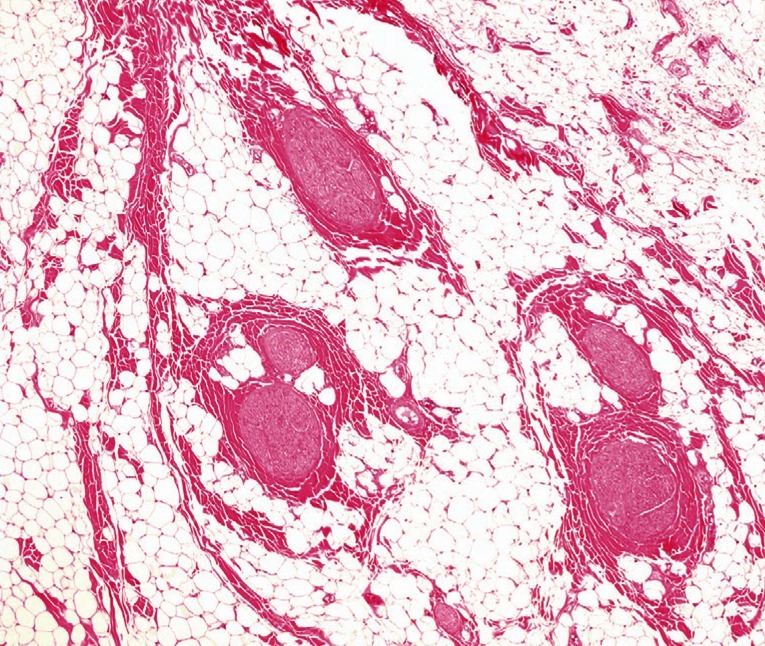
Histopathologic finding shows an overgrowth of fatty tissue within the fibrous tissue and the substance of the nerve (H&E, ×100).
The wound healed without any complications, but with some degree of sensory loss in the first web space. The patient is now able to pick up objects using his left hand with less effort (Fig. 5), but we are considering performing an additional debulking operation to improve the function and appearance of the hand.
Fig. 5.

Postoperative opposing photographs. Opposing difficulty improved postoperatively. The patient could pick up objects more readily than before.
Macrodystrophia lipomatosa is a rare form of non-hereditary congenital localized gigantism characterized by progressive overgrowth of mesenchymal elements with a disproportionate increase in the amount of fibroadipose tissue. It is usually recognized in the neonatal period, but generally only starts to cause problems as the child grows. This abnormality occurs most frequently where the median nerve is distributed in the upper extremities and the plantar nerve in the lower extremities. Usually, one or more digits of the unilateral limb are affected. The patient had a lesion at the unilateral upper extremity along the median nerve that had an increase in size disproportionate to the rest of his body.
There may be functional problems, such as difficulty in grasping or gait, but surgical consultation is usually sought for cosmetic rather than mechanical reasons. This patient had difficulty in picking up objects mainly due to a severely deformed index finger, but the main concern of the patient and his parents was cosmesis.
Imaging studies play an important role in the diagnosis of this disease as they allow characterization of the nature of the hypertrophied tissue. Plain radiographs can demonstrate the abnormalities of soft tissues and bony elements. Characteristic radiolucencies are indicative of the fatty nature of the soft tissue. The fibroadipose tissue appears hyperintense on both T1- and T2-weighted MRI images, and the density of the excessive adipose tissue is identical to that of normal subcutaneous fat tissue. Soler et al. [2] proposed that MRI should be used to detect fibroadipose tissue masses with proportional enlargement of other mesenchymal tissues as the diagnostic method of choice for macrodystrophia lipomatosa.
Histopathological findings show an abundant increase in adipose tissue scattered in a fine, mesh-like fibrous tissue [3]. Underlying subcutaneous tissues, nerve sheaths, muscles, periosteum, and even bone marrow can also be involved. Despite many histopathological changes, the exact pathogenesis is obscure, but the proposed mechanisms include lipomatous degeneration, disturbed fetal circulation, imbalances in growth inhibiting factors, and errors in segmentation [4].
Differential diagnosis commonly includes neurofibromatosis type I, hemangiomatosis, lymphangiomatosis, Klippel-Trenaunay-Weber syndrome, fibrolipomatosis hamartoma of a nerve, and Proteus syndrome. Among these, the disease that is the most difficult to differentially diagnose from macrodystrophia lipomatosa is neurofibromatosis. Neurofibromatosis can be diagnosed by a positive family history and certain characteristic cutaneous manifestations such as café-au-lait spots on the skin and soft tissue nodules. Furthermore, because bony overgrowth and fat deposition in subcutaneous tissues, tendons, muscles, and nerves with macrodactyly are specific diagnostic features of macrodystrophia lipomatosa, it can be differentiated from other diseases that can show similar clinical features.
Surgical intervention is the treatment of choice for macrodystrophia lipomatosa. The main surgical principle in treating these lesions is to improve the cosmetic appearance while preserving the neurologic function as much as possible. Through judicious and planned multiple debulking operations and partial amputations, good results can be achieved. However, surgery should be delayed until the patient's growth is complete if the deformity is not very serious and if no nervous system symptoms are present.
Complications associated with overzealous debulking procedures can lead to nerve injury; the reported incidence ranges from 30% to 50%. A localized recurrence rate of 33% to 60% makes the management of macrodystrophia lipomatosa demanding [5]. In our case, we achieved a satisfactory outcome in terms of functional recovery and the aesthetic results using debulking and amputation. However, we will continue to follow this patient to evaluate whether the symptoms regress to a static lesion or not.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Goldman AB, Kaye JJ. Macrodystrophia lipomatosa: radiographic diagnosis. AJR Am J Roentgenol. 1977;128:101–105. doi: 10.2214/ajr.128.1.101. [DOI] [PubMed] [Google Scholar]
- 2.Soler R, Rodriguez E, Bargiela A, et al. MR findings of macrodystrophia lipomatosa. Clin Imaging. 1997;21:135–137. doi: 10.1016/0899-7071(95)00095-x. [DOI] [PubMed] [Google Scholar]
- 3.Gupta SK, Sharma OP, Sharma SV, et al. Macrodystrophia lipomatosa: radiographic observations. Br J Radiol. 1992;65:769–773. doi: 10.1259/0007-1285-65-777-769. [DOI] [PubMed] [Google Scholar]
- 4.Rohilla S, Jain N, Sharma R, et al. Macrodystrophia lipomatosa involving multiple nerves. J Orthop Traumatol. 2012;13:41–45. doi: 10.1007/s10195-011-0159-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brodwater BK, Major NM, Goldner RD, et al. Macrodystrophia lipomatosa with associated fibrolipomatous hamartoma of the median nerve. Pediatr Surg Int. 2000;16:216–218. doi: 10.1007/s003830050728. [DOI] [PubMed] [Google Scholar]