

Stewart-Treves syndrome is a kind of angiosarcoma associated with chronic lymphedema. It was first reported by Stewart and Treves [1] in 1948. In their study, they reported a series of six patients who had developed angiosarcoma in their lymphedematous extremities after radical mastectomy. The exact mechanism of Stewart-Treves syndrome is not clear. It may be due, however, to the accumulation of protein-rich interstitial fluid in a chronically swollen limb [2]. This fluid alters the local immune environment of the chronically edematous limb and promotes lymphangiogenesis. It also aggravates the locally immunocompromised state to easily presented malignancy. The prognosis of Stewart-Treves syndrome has been regarded as poor due to its aggressiveness. The mean survival period from this disease has been quoted to be seven months, with an approximately 35% overall five-year survival rate [3]. Because of its aggressiveness and poor prognosis, early detection and surgical management are considered the key factors in the survival of patients.
In this article, a rare case of Stewart-Treves syndrome in the lower extremities that was misdiagnosed as a pressure ulcer is reported. A 72-year-old female was referred to the authors' clinic for the management of a protruding purple to black skin lesion with central ulceration, which developed about six months before the patient's presentation, in her right lower leg (Fig. 1). Her physical examination showed that the size of the lesion was about 9 cm×8 cm, and there was a mild pitting edema in her right lower leg. Since the initial development of the lesion, the patient had been treated in the local clinic under the impression of apressure ulcer, but the central ulceration worsened three months before the patient's visit to the authors' clinic. The patient had been a quadriplegic for more than 27 years after a cervical spine injury, and had undergone an operation for open reduction and internal fixation of her right femur shaft fracture 10 years earlier. The initial laboratory findings were not specific. A punch biopsy was performed first, and its result showed merely a poorly differentiated malignant tumor, which was difficult to distinguish as sarcoma or melanoma.
Fig. 1.

Preoperative findings of a 9 cm×8 cm purple to black protruding skin lesion with central ulceration on the upper lateral side of the right lower leg with diffuse edema.
A T2-weighted magnetic resonance image of the right lower extremity showed a 6.7 cm×3.0 cm×8.3 cm enhanced mass with an intermediate signal intensity and with surrounding increased vascularity (Fig. 2). The image also showed diffuse subcutaneous edema on the right lower leg. Positron emission tomography-computed tomography showed a fludeoxyglucose-avid malignant tumor in the upper lateral aspect of the right lower leg with possible extension to the adjacent soft tissue and a unilateral subcutaneous honeycomb-appearance that suggested long-standing lymphedema (Fig. 3). There was no evidence of metastasis.
Fig. 2.

Magnetic resonance imaging of a 6.7 cm×3.0 cm×8.3 cm enhanced irregular mass with an intermediate signal intensity on the T2 weighted image and good development of the vascular structure accompanied by diffuse subcutaneous edema.
Fig. 3.
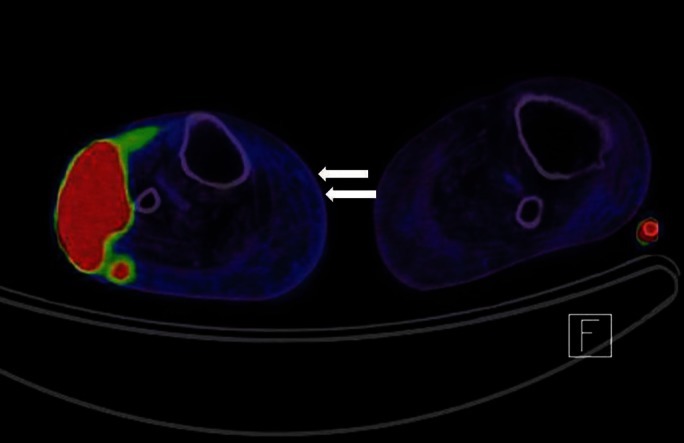
The positron emission tomography-computed tomography of the fludeoxyglucose-avid malignant tumor in the upper lateral aspect of the right lower leg with possible extension to the adjacent soft tissue and a unilateral subcutaneous honeycomb-appearance (white arrows) suggests long-standing lymphedema. There was no evidence of metastasis.
A wide excision was performed with a 3 cm safety margin that included part of the fibular head. The frozen section was margin-free of the tumor, and the defect was covered with a split-thickness skin graft. The histologic examination showed diffuse extravasation of red blood cells with rich vascularity, and the vascular endothelial cells showed severe pleomorphism (Fig. 4A). The immunohistochemistry of CD31, CD34, and vimentin (Fig. 4B) were positive, so the pathologist confirmed the diagnosis of angiosarcoma.
Fig. 4.
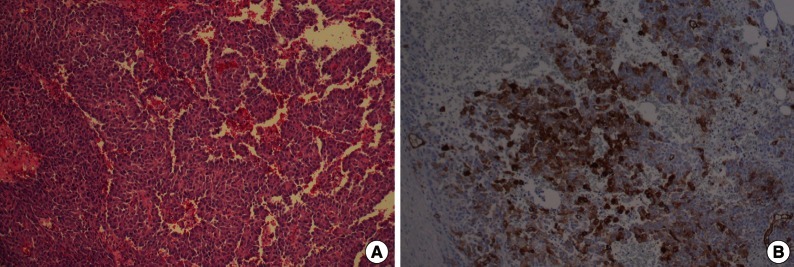
Histologic findings. (A) H&E stain (×40) demonstrated abnormal, pleomorphic, and malignant endothelial cells. (B) Positive immunohistochemistry of vimentin (×100).
The oncology department recommended adjuvant radiotherapy, but the patient refused it because of her poor economic status. She underwent right lower leg amputation above her knee one month after her first operation, and she expired three months later due to pleural metastasis with malignant pleural effusion.
Angiosarcoma is a rare soft tissue malignancy of vascular endothelial cell origin. Angiosarcomas can be classified into several subtypes [3]. Primary cutaneous angiosarcoma occurs on the face and scalp of older patients. Lymphedema-associated angiosarcoma, also known as Stewart-Treves syndrome, is associated with chronic lymphedema. Other angiosarcoma subtypes include radiation-induced angiosarcoma, primary breast angiosarcoma, deep soft-tissue angiosarcoma, and visceral angiosarcoma.
The histopathological appearance of Stewart-Treves syndrome can vary from a well-differentiated lesion to a poorly differentiated one [3]. Low-grade, well-differentiated lesions show irregular vascular channels and cutaneous angiosarcoma with an irregular or sinusoidal vessel pattern. High-grade, poorly differentiated lesions can comprise undifferentiated cells, so they are difficult to differentiate from other malignancies. These tumors can be confirmed via immunohistochemistry and are usually positive for factor-VIII-related antigen, vimentin, CD34, and CD31.
Wide excision is the only known curative treatment option for the localized disease, and there is no known effective therapy for the metastatic disease [4]. Thus, only early diagnosis and prompt radical excision with or without adjuvant radiotherapy can promote survival.
The diagnosis can be delayed, however, because it may show only erythema, swelling, and a papule-like skin lesion initially, and ulceration, hemorrhage, and mass fungation later [3]. Thus, if there is pain, sudden enlargement, or purple-red nodules on the skin of the involved extremity, recognition of their significance and their prompt evaluation by a surgeon are very important.
In conclusion, the authors experienced a case of Stewart-Treves syndrome in the lower leg, which was misdiagnosed initially and therefore, the treatment of which was delayed. It was reported herein because an atypical skin lesion in a chronically edematous limb can be malignant even if it looks benign, and a high level of suspicion and early management of the lesion are very important in improving the potential for patient survival.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Stewart FW, Treves N. Lymphangiosarcoma in postmastectomy lymphedema; a report of six cases in elephantiasis chirurgica. Cancer. 1948;1:64–81. doi: 10.1002/1097-0142(194805)1:1<64::aid-cncr2820010105>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 2.McHaffie DR, Kozak KR, Warner TF, et al. Stewart-Treves syndrome of the lower extremity. J Clin Oncol. 2010;28:e351–e352. doi: 10.1200/JCO.2009.26.0406. [DOI] [PubMed] [Google Scholar]
- 3.Young RJ, Brown NJ, Reed MW, et al. Angiosarcoma. Lancet Oncol. 2010;11:983–991. doi: 10.1016/S1470-2045(10)70023-1. [DOI] [PubMed] [Google Scholar]
- 4.Abraham JA, Hornicek FJ, Kaufman AM, et al. Treatment and outcome of 82 patients with angiosarcoma. Ann Surg Oncol. 2007;14:1953–1967. doi: 10.1245/s10434-006-9335-y. [DOI] [PubMed] [Google Scholar]