

Dear Editor,
The skin is a relatively uncommon site for distant metastatic deposits, compared with organ such as liver, bone, and lung. The most common sources of cutaneous metastases are: Breast, skin tumors, lung, colon, stomach, upper aerodigestive tract, uterus, and kidney.[1]
We describe the case of a 65-year-old patient, male, presented with a non-tender nodule, exophytic, rounded, of parenchymatous consistency, at the right rima oris, of around 2 cm in diameter, pinkish-purple colored, translucent lined by multiple telangiectasia [Figure 1].
Figure 1.

A nodule upper right of rima oris
The patient was operated 2 years before for poorly-differentiated carcinoma at the rectum with multiple secondary lesions. The histological examination showed a solid pattern with nidus aspects of the pseudoglandular type [Figure 2], revealed as a neuroendocrine carcinoma.
Figure 2.
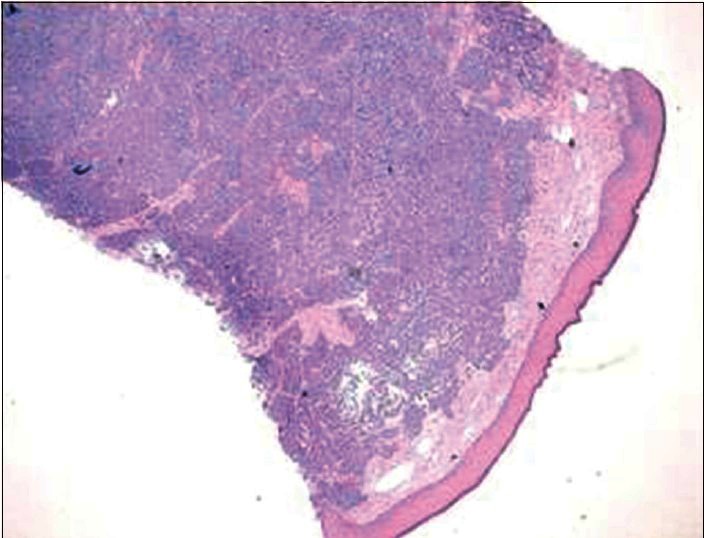
Section of skin with H and E, staining ×20
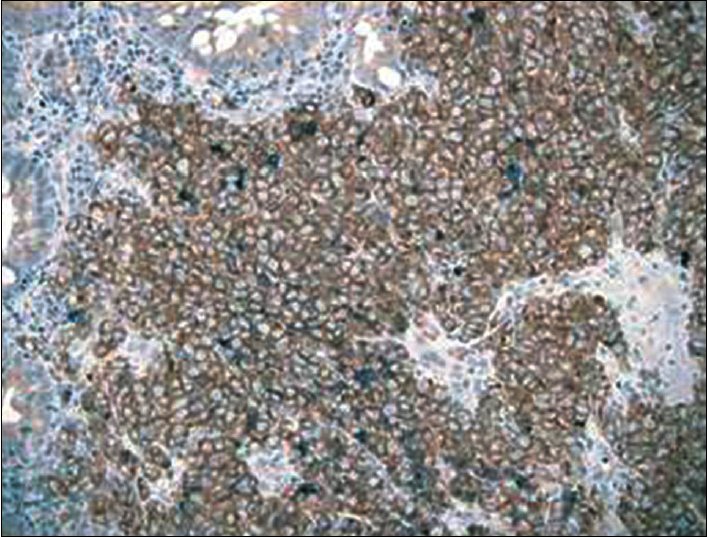
To confirm the neuroendocrine differentiation, immunohistochemical investigations were made with following results: Chromogranin A−, synaptophysin+++, CK7−, CK20−, Neuron-Specific Enolase (NSE) - [Figure 3]. Considering his anamnesis and a diagnosis of a possible skin metastatic lesion, we performed an immunohistochemical analysis of the biopsy samples of the rectal carcinoma. The immunohistochemical panel confirms a strong positivity for synaptophysin and negativity for chromogranin A, CK7, CK20, NSE [Figure 4].
Figure 3.

Detail of the skin neoplasia with synaptophysin staining
Figure 4.
Detail of the rectal neoplasia with synaptophysin staining
Neuroendocrine tumors (NETs) are rare malignant neoplasia, which are more frequent at the intestinal level where they represent, however, less than 1% of tumors.[2–4]
Metastatic neuroendocrine carcinomas to the skin are infrequent and need to be differentiated from primary neuroendocrine skin tumors, in particular, from Merkel cell carcinoma.
In the case presented here, the diagnosis of metastasis seemed likely since the patient had already diffuse metastatic disease at presentation and was confirmed by a comparative immunohistochemical study of both tumors (cutaneous and rectal).
The most common sources of cutaneous metastasis are breast, melanoma, lung, colon, stomach, upper aereodigestive-tract, uterus, and kidney. The most common skin metastasis from a previously uncommon primary tumor originates from the kidney, lung, thyroid, or ovary.[4–6]
Neuroendocrine cell (NEC) carcinomas of the colon and rectum are uncommon, comprising less than 1% of colon and rectal cancer. NEC carcinomas typically stain for the immunohistochemical markers synaptophysin, chromogranin, or neuron-specific enolase. It is well-known that NEC carcinomas of the colon and rectum has very poor prognosis.[7–8]
The synaptophysine is a transmembrane glycoprotein with a molecular weight of 38 kDa and is a specific marker of neuroendocrinal differentiation.
The synaptophysine has been identified in diverse primary neuroendocrine (NE) tumors of both neural and epithelial origin. In literature, there are many studies that confirm that expression of synaptophysin can be maintained during formation of metastases of several types of NE tumors, including medullary thyroid carcinoma, gastrinoma, insulinoma, small (oat) cell carcinoma of the lung, gastrointestinal carcinoid, and neuroblastoma,
Synaptophysin immunohistochemical study is widely used for the positive identification of metastatic NE tumors, notably in differential diagnosis, as in our case report.[9]
We would also like to draw attention to the diagnostic role of skin metastases which, in 7% of cases, according to the literature, may represent the first manifestation of an occult carcinoma, but coincide with a rapid progression of neoplastic disease.[10]
References
- 1.Cox NH, Coulson IH. Systemic Disease and the Skin. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 8th ed. wiley-Blackwell; 2010. pp. 62–17. [Google Scholar]
- 2.Saclarides TJ, Szeluga D, Staren ED. Neuroendocrine cancer of the colon and rectum: Results of ten-year experience. Dis Colon Rectum. 1994;37:635–42. doi: 10.1007/BF02054405. [DOI] [PubMed] [Google Scholar]
- 3.Vilor M, Tsutsumi Y, Osamura YR, Tokunaga N, Soeda J, Ohta M, et al. Small cell neuroendocrine carcinoma of the rectum. Pathol Int. 1995;45:605–9. doi: 10.1111/j.1440-1827.1995.tb03510.x. [DOI] [PubMed] [Google Scholar]
- 4.Schwatrz RA. Cutaneous metastatic disease. J Am Acad Dermatol. 1995;33:161–82. doi: 10.1016/0190-9622(95)90231-7. [DOI] [PubMed] [Google Scholar]
- 5.Marcoval J, Morena A, Pejri J. Cutaneous infiltration by cancer. J Am Acad Dermatol. 2007;57:577–80. doi: 10.1016/j.jaad.2007.01.034. [DOI] [PubMed] [Google Scholar]
- 6.Weedon D. 2nd ed. London: Churchill livingstone; 2002. Weedon's Skin Pathology; pp. 1045–56. [Google Scholar]
- 7.Grabowski P, Schindler I, Anagnostopoulos I, Foss HD, Riecken EO, Mansmann U, et al. Neuroendocrine differentiation is a relevant prognostic factor in stage III-IV colorectal cancer. Eur J Gastroenterol Hepatol. 2001;13:404–11. doi: 10.1097/00042737-200104000-00018. [DOI] [PubMed] [Google Scholar]
- 8.Miyamoto H, Kurita N, Nishioka M, Ando T, Tashiro T, Hirokawa M, et al. Poorly differentiated neuroendocrine cell carcinoma of the rectum: Report of a case and literal review. J Med Invest. 2006;53:317–20. doi: 10.2152/jmi.53.317. [DOI] [PubMed] [Google Scholar]
- 9.Wiedenmann B, Kuhn C, Schwechheimer K, Waldherr R, Raue F, Brandeis WE, et al. Synaptophysin identified in metastases of neuroendocrine tumors by immunocytochemistry and immunoblotting. Am J Clin Pathol. 1987;88:560–9. doi: 10.1093/ajcp/88.5.560. [DOI] [PubMed] [Google Scholar]
- 10.Grabowski P, Schönfelder J, Ahnert-Hilger G, Foss HD, Heine B, Schindler I, et al. Expression of neuroendocrine markers: A signature of human undifferentiated carcinoma of the colon and rectum. Virchows Arch. 2002;441:256–63. doi: 10.1007/s00428-002-0650-9. [DOI] [PubMed] [Google Scholar]