

Abstract
AIMS:
The direct involvement of clinical pharmacists in patient care is an ever-evolving role in the pharmacy profession. Studies have demonstrated that discharge counseling performed by a clinical pharmacist improves patients’ knowledge of their medications. The aim of this article is to evaluate the effect of patients’ educational level and previous counseling on medication knowledge among patients visiting King Abdulaziz Medical City, a tertiary care center.
METHODS:
The effect of the education level and previous counseling on medication knowledge was assessed in 90 patients in both inpatient and outpatient settings at King Abdul Aziz Medical City during a 5-week period using a questionnaire that contains items to assess patients’ medication knowledge and the pharmacists’ performance during counseling.
RESULTS:
The average age of the participants was 52.9 ± 17.6 years. The participants’ education level was not significantly associated with gender; however, it was significantly associated with age, P < 0.05. A higher educational level was found to positively affect the aspects of medication knowledge that were assessed in this study (P < 0.05): 35.8-56.9% of the non-educated patients showed good to excellent recognition of medications, knowledge of their indications, and knowledge of dosage schedule compared to 76.2-90.5% for the more educated participants. Furthermore, 13.6%, 38.1%, and 70.0% of the non-educated group, the below high school group and high school education or above group, respectively, demonstrated good to excellent knowledge of their medications’ side effects. Previous counseling was also positively linked to medication knowledge (P < 0.05). Here, 87.8-97.6% of the patients who received previous counseling showed good to excellent recognition of medications, knowledge of their indications, and better knowledge of dosage schedule compared to 37.2-43.2% for those who did not. Finally, 52.9% of the patients who received previous counseling showed good to excellent knowledge of medication side effects compared to only 12.5% for those who did not.
CONCLUSIONS:
The education level of the patient and previous counseling are positively linked to medication knowledge. Knowledge of the medications’ side effects proved to be the most difficult task for the participants in this study, requiring the highest level of education, and was improved by previous counseling.
Keywords: Discharge counseling, educational level, medication knowledge, patient counseling
The direct involvement of clinical pharmacists in patient care is an ever-evolving role in the pharmacy profession. A systematic review by Kaboli et al., (2006) discussing the involvement of clinical pharmacists in inpatient medical care showed that inpatient services by clinical pharmacists have resulted in improved care without evidence of harm.[1] Among the many roles that a pharmacist can play in a healthcare setting is patient counseling which has been linked to many positive heath care outcomes. Patient counseling helps in identifying processes that can help in preventing drug-related problems.[2] Schnipper et al., (2006) have also reported that medication review, patient counseling, and telephone follow-up by a pharmacist were associated with a lower rate of preventable adverse drug effects 30 days post-hospital discharge. In addition, medication knowledge has been shown to be directly proportional to the educational level of the patients.[3] For example, Marks et al., (2010) found that the Medication Knowledge Score (MKS) was affected positively by younger age, higher educational level, and female gender.[4] Trevino et al., (2005) have also shown that medication knowledge is positively correlated with education.[5] However, Kerzman et al., (2005) have reported contradictory findings stating that there is no significant effect of age, gender or educational level on medication knowledge of patients.[6] Nevertheless, most evidence indicates a benefit to identifying patients with limited health literacy and offering them tailored medication counseling that fits their needs.[7]
The aim of this article is to evaluate the effect of patients’ educational level and previous counseling on medication knowledge among patients visiting King Abdulaziz Medical City (KAMC), a tertiary care center.
Methods
This study was conducted by patient counseling pharmacists at KAMC, which is a tertiary care center located in Riyadh, Saudi Arabia. The study used a convenience sample that included hospitalized and ambulatory patients over a period of 5 weeks.
The study was approved by the Institutional Review Board (IRB) of King Abdulaziz Medical City at the National Guard Health Affair, Riyadh, Saudi Arabia. A verbal approval to participate was sought from patients by the counseling pharmacist in order to include them in the study. Of 100 patients that were approached, 90 agreed to be included in the study.
The pharmacist obtained data during one-on-one interviews with the patients. The patient counseling form used in the interviews included two sections. The first section elicited demographic information, age, gender, and educational level and included a question about receiving previous counseling. The second section included four questions that were concerned with the patient's medication knowledge:
Does the patient recognize his/her medications?
Does the patient know the indication(s) of his/her medications?
Does the patient know the dosage schedule of his/her medications? and finally,
Does the patient know the major side effects of his/her medications?
The answers to these questions were rated by a 4-point Likert scale: 1 = Excellent, 2 = Good, 3 = Acceptable, and 4 = Bad. Excellent means that the patient has recalled all the required information, Good means that the patient has recalled the majority of the required information, Acceptable means that the patient has recalled some of the required information and Bad means that the patient recalled very little or none of the required information. These questions have been used, in various forms, in previous studies.[4,8,9] The questions in the specific form that is used in the current study have not been validated.
Association between variables was statistically analyzed using the cross-tabulation (Chi square) method implemented in Statistical Package for the Social Sciences (SPSS) v20 (IBM, USA). A P < 0.05 was considered significant.
Results
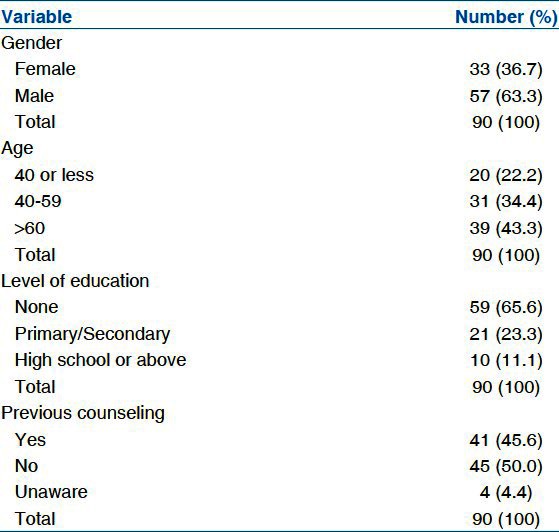
The sample characteristics are shown in Table 1. One hundred patients were approached, all of whom could communicate verbally and had no signs of dementia. Of the 100 approached, 90 patients agreed to participate in the study and completed the interview giving a response rate of 90%. The patients were categorized according to age groups into three categories: <40 years (22.2%), 40-59 years (34.4%), and ≥60 years (43.3%) with an overall average age of 52.9 ± 17.6 years. The participants were 63.3% males and 36.7% females. The patients were categorized according to the level of education into three categories: None (65.6%), below high school (23.3%), and high school or above (11.1%). Finally, 45.6% of the patients indicated that they had received previous counseling compared to 50.0% and 4.4% of the patients who indicated that they did not receive previous counseling or they cannot remember, respectively.
Table 1.
Characteristics of the sample
The association between the education levels of patients with other demographics was analyzed and the results are summarized in Table 2. There was no significant association between the education level of the patients and gender. However, the patients’ educational level was found to be significantly associated with age, P < 0.05. In this regard, 40.7% of the non-educated participants were <60 years of age, while 80.9% of the patients with less than high school education were <60 years of age and all those with high school education or above were <60 years of age. With regard to medication knowledge, the patients’ education level was significantly associated with all four aspects of medication knowledge (P < 0.05), i.e., medication recognition, medications’ indication, dosage schedule, and the medications’ major side effects. Only 35.8% of the non-educated patients showed good to excellent recognition of their medications compared to 90% and 90.5% for the other two more educated groups. Similarly, 47.5% of the non-educated groups showed good to excellent knowledge of the indications of their medication compared to 80% and 81.0% for the other two more educated groups. The trend continues with the knowledge of dosage schedule as 56.9% of the non-educated group showed good to excellent knowledge of their medication schedule compared to 76.2% and 80.0% of the other two more educated groups. In case of the knowledge of the medications’ side effects, patients showed more dramatic stratifications. Here, only 13.6% of the non-educated group demonstrated good to excellent knowledge, while 38.1% of the group whose education is below high school and 70.0% of the patients who have high school education or above demonstrated good to excellent knowledge of their medications’ side effects.
Table 2.
Cross tabulation of the level of education and pervious counseling vs. medication knowledge
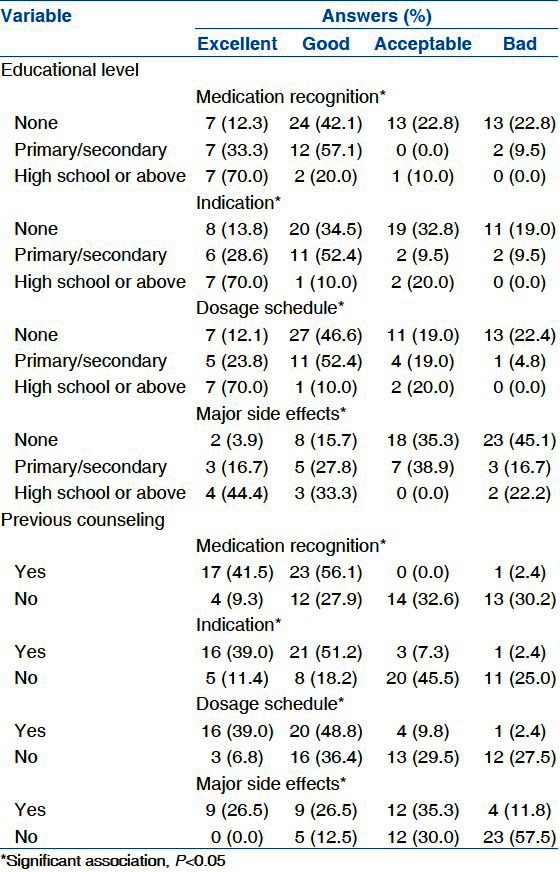
Like the education level, previous counseling was significantly associated with medication recognition, indications, schedule and side effects (P < 0.05), [Table 2]. Here, 97.6% of the patients who received previous counseling showed good to excellent recognition of their medications compared to 37.2% for those who did not. Similarly, 90.2% of the patients who received previous counseling showed good to excellent knowledge of the indications of their medication compared to 29.5% for those who did not. Excellent to good knowledge of medication schedule was demonstrated by 87.8% of the patients who received previous counseling compared to 43.2% for those who did not. The least level of knowledge was related to medication side effects as 52.9% of the patients who received previous counseling demonstrated good to excellent knowledge compared to 12.5% for those who did not.
Finally, there was a significant association between the education level of the patients and receiving previous counseling (P < 0.05). Here, 62.7% of the non-educated group did not receive previous counseling compared only to 27.8% and 30.0%for the other two educational groups.
Discussion
Most of the participants in this study were non-educated which may be due, in part, to the fact that most of the participants were ≥60 years of age as older age was significantly associated with lower level of education. In addition, the World Bank statistics about Saudi Arabia state the literacy rate of people who are 65 years and above is 25.9% (2004) and for youth, age 15-24 years it is 97.8% (2010).[10] Unlike age, patients’ gender has no significant association with their educational level. These results agree with the 2005-2010 United Nations International Children's Emergency Fund (UNICEF) data about Saudi Arabia which shows that distribution of gender is even in the two K-12 education levels (primary and secondary).[11] On the other hand, the Saudi Central Department for Statistics and Information reported that up to the year 2009, the number of post-secondary female graduates (i.e., above high school education) are 43.0% males compared to 57.0% females.[12] This difference did not appear in this study, most likely because the sample size of females was very low.
The results show that the higher the level of education, the better is the patient's knowledge about his/her medication. This conclusion is in agreement with the results of other studies that have investigated the association between education and patient's medication knowledge using different tools such as the MKS developed by Marks et al., (2010)[4] and an adaptive questionnaire developed by Okuyan et al., (2012).[13] The agreement of the results of this study with the results obtained by different tools supports the validity of this study's results and its simple questionnaire.
Although it was not surprising to see the significant association between the level of education and the four aspects of patient knowledge investigated in this study, the trend of this association was interesting. While 67.1%, 59.6%, and 65.2% of the total sample showed good to excellent medication recognition, knowledge of indication, and knowledge of dosage schedule, respectively, only 31.2% of the sample demonstrated good to excellent knowledge of the medications’ side effects. These results when coupled with fact that only 13.6% of the “non-educated group”, 38.1% of “below high school education group”, and 70.0% of the “high school education or above group” demonstrated good to excellent knowledge of their medications’ side effects, lead to the conclusion that this particular aspect of medication knowledge requires a higher education level. The lower level of knowledge of medication side effects compared to other aspects of medication knowledge has been previously reported in literature by Modig et al., (2008) who found that 60% of the elderly patients knew the indication for their medications while only 6% knew the risks, side effects, or interactions related to their medications.[14] Furthermore, it has been reported that 55.8%, 93.4%, 78.8%, and 11.7% of the patients were able to state their correct drug names, dosages, indications, and at least one side effect, respectively.[4]
Previous counseling can be considered a specific form of health education in which the patient receives information related to his/her medication. At KAMC, the medication-related information that is offered to patients during counseling sessions covers medication recognition, indication, schedule, and side effects. Taking that into consideration, it would be expected that previous counseling should have a positive effect on patients’ medication knowledge as was demonstrated by the results in this study. It has been previously shown that discharge counseling performed by a clinical pharmacist improves the patients’ knowledge of their medications.[15] Accordingly, patient counseling by pharmacists at KAMC can be considered effective as a health education tool. In this context, patient counseling should be considered a continuous process in which the patient is in a process of continuous learning[16] rather than someone who understands every aspect of his or her medication regimen after the first session of counseling.
Most of the non-educated participants indicated that they were not previously counseled and the opposite was true for the other two educational groups. While this association was significant, P < 0.05, its nature cannot be determined from the available data. The effect of previous counseling was found to be parallel to the effect of higher education level, and that might make their effects additive. It will be interesting to investigate the codependency of the effect of these two variables in a future work.
Finally, the main study limitation was the use of a convenience sample, which can lead to under-representation or over-representation of particular groups within the sample. In addition, convenience samples may not be representative of the population, which undermines the generalizability of the results.
Conclusions
Assessment of the association between the level of patients’ education and previous counseling on medication knowledge was performed. It was found that better medication knowledge is associated with higher educational levels and previous counseling by a pharmacist. These results are crucial in designing and implementing a patient-counseling program. A well-tailored counseling program that takes into consideration the patients’ education level might help in enhancing medication knowledge among those with lower educational levels. Furthermore, continuous patient counseling will also lead to better medication knowledge. We propose to develop and assess a well-structured continuous approach to patient counseling aimed at increasing patient's knowledge of their medications, especially side effects, which was the area with weakest response from all participants. This program is expected to be most helpful in patients with low levels of education.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: A systematic review. Arch Intern Med. 2006;166:955–64. doi: 10.1001/archinte.166.9.955. [DOI] [PubMed] [Google Scholar]
- 2.Karapinar-Çarkit F, Borgsteede SD, Zoer J, Smit HJ, Egberts AC, van den Bemt PM. Effect of medication reconciliation with and without patient counseling on the number of pharmaceutical interventions among patients discharged from the hospital. Ann Pharmacother. 2009;43:1001–10. doi: 10.1345/aph.1L597. [DOI] [PubMed] [Google Scholar]
- 3.Ponnusankar S, Surulivelrajan M, Anandamoorthy N, Suresh B. Assessment of impact of medication counseling on patients’ medication knowledge and compliance in an outpatient clinic in South India. Patient Educ Couns. 2004;54:55–60. doi: 10.1016/S0738-3991(03)00193-9. [DOI] [PubMed] [Google Scholar]
- 4.Marks JR, Schectman JM, Groninger H, Plews-Ogan ML. The association of health literacy and socio-demographic factors with medication knowledge. Patient Educ Couns. 2010;78:372–6. doi: 10.1016/j.pec.2009.06.017. [DOI] [PubMed] [Google Scholar]
- 5.Trevino J, Albright T, Wright F, Cigarroa L. Correlates of medication knowledge and adherence: Findings from the residency research network of South Texas. Family Med. 2005;37:712–8. [PubMed] [Google Scholar]
- 6.Kerzman H, Baron-Epel O, Toren O. What do discharged patients know about their medication? Patient Educ Couns. 2005;56:276–82. doi: 10.1016/j.pec.2004.02.019. [DOI] [PubMed] [Google Scholar]
- 7.Ngoh LN. Health literacy: A barrier to pharmacist-patient communication and medication adherence. J Am Pharm Assoc. 2009;49:e132–49. doi: 10.1331/JAPhA.2009.07075. [DOI] [PubMed] [Google Scholar]
- 8.Nnaemeka OR, Kingsley NC. Evaluation of patient's antidiabetic medication counseling provided by pharmacists in a tertiary health care setting in nigeria. Int Res J Pharm. 2012;3:319–23. [Google Scholar]
- 9.Partovi N, Chan W, Nimmo C. Evaluation of a patient education program for solid organ transplant patients. Canadian J Hospital Pharmacy. 1995;48:72–8. [PubMed] [Google Scholar]
- 10.World Bank. Saudi Arabia-All Society Indicators 2004. [Last accessed on February 8, 2013]. Available from: http://wwwquandlcom/society/saudi-arabia-all-society-indicators .
- 11.UNICEF. Saudi Arabia, Statistics 2010. [Last accessed on January 19, 2013]. Available from: http://wwwuniceforg/infobycountry/saudiarabia_statisticshtml .
- 12.Saudi Arabia social statistics, education: Saudi central department for statistics and information. 2009. [Last accessed on January 19, 2013]. Available from: http://www.cdsi.gov.sa/english/index.php?option=com_docman andtask=cat_view&gid=188&Itemid=113 .
- 13.Okuyan B, Sancar M, Izzettin FV. Assessment of medication knowledge and adherence among patients under oral chronic medication treatment in community pharmacy settings. Pharmacoepidemiol Drug Saf. 2013;22:209–14. doi: 10.1002/pds.3275. [DOI] [PubMed] [Google Scholar]
- 14.Modig S, Kristensson J, Ekwall KA, Hallberg RI, Midlöv P. Frail elderly patients in primary care – their medication knowledge and beliefs about prescribed medicines. Eur J Clin Pharmacol. 2009;65:151–5. doi: 10.1007/s00228-008-0581-8. [DOI] [PubMed] [Google Scholar]
- 15.Strobach D, Vetter-Kerkhoff C, Bogner J, Breugst W, Schlöndorff D. Patient medication counseling – patient counseling about discharge medication. Medizinische Klinik (Munich) 2000;95:548–51. doi: 10.1007/pl00002061. [DOI] [PubMed] [Google Scholar]
- 16.Lennerling A, Forsberg A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nur J. 2012;6:41–6. doi: 10.2174/1874434601206010041. [DOI] [PMC free article] [PubMed] [Google Scholar]