

Abstract
Imitation is an early skill thought to play a role in social development, leading some to suggest that teaching imitation to children with autism should lead to improvements in social functioning. This study used a randomized controlled trial to evaluate the effect of a focused imitation intervention on initiation of joint attention and social-emotional functioning in 27 young children with autism. Results indicated the treatment group made significantly more gains in joint attention initiations at post-treatment and follow-up and social-emotional functioning at follow-up than the control group. Although gains in social functioning were associated with treatment, a mediation analysis did not support imitation as the mechanism of action. These findings suggest the intervention improves social functioning in children with ASD.
Keywords: Autism, Imitation, Intervention, Social, Reciprocal Imitation Training
Imitation is an early emerging skill that serves an important cognitive and a social function in typical development (Uzgiris, 1981). Children with autism exhibit significant deficits in imitation (Smith & Bryson, 1994) as well as later emerging social behaviors (APA, 2000), leading to the proposal that an early deficit in imitation could disrupt the development of intersubjectivity and lead to broader social impairments in autism (Rogers & Pennington, 1991). Although it has yet to be established whether imitation deficits are a cause or a consequence of social impairment in autism, a number of studies have found a significant relationship between imitation and other social behaviors in children with autism, including social reciprocity and initiation of joint attention (e.g., McDuffie et al., 2007; Rogers, Hepburn, Stackhouse, & Wehner, 2003). This relationship in combination with research on the role of imitation in typical social development, has led to the suggestion that teaching imitation should lead to broader improvements in social functioning in children with autism (Ingersoll, 2008; McDuffie et al., 2007; Rogers, 1999). Given the pervasive deficits in social behavior in autism, the possibility that a focused imitation intervention could lead to broader gains in social functioning is important to investigate.
Reciprocal Imitation Training (RIT) was developed to teach the social function of imitation to young children with autism (Ingersoll, 2008). RIT uses a blend of naturalistic behavioral and developmental strategies to teach imitation within a social-interactive context. A series of single-subject design studies (Ingersoll, Lewis, & Kroman, 2007; Ingersoll & Schreibman, 2006) and a small randomized controlled trial (n=21) (Ingersoll, 2010) have shown RIT to be efficacious for increasing spontaneous object and gesture imitation in young children with autism. Importantly, one single-subject design study found collateral improvements in coordinated joint attention during RIT intervention sessions for four of five participants (Ingersoll & Schreibman, 2006). To further validate the efficacy of this approach for improving social functioning more broadly in young children with autism, it is necessary to apply the gold standard of a randomized controlled trial and standardized assessments of social functioning. Further, although improvements in coordinated joint attention occurred at the onset of treatment, it could not be established that gains in imitation were responsible for these improvements. Thus, it is important to examine whether improvement in social behaviors are a result of the intervention’s effect on imitation.
The primary goal of study was to investigate whether a focused imitation intervention results in broader gains in social functioning in young children with autism. For this study, we examined both a specific indicator of social functioning, initiation of joint attention, as well as a general indicator of social functioning, parent report of social-emotional skills. A secondary goal was to examine whether improvements in social functioning were a result of the intervention’s effect on the children’s imitation skills.
Methods
Participants
Participants were 29 children with autism between 27 and 47 months. Pre- and post-treatment imitation data from 22 of these children were presented in a previous paper that examined the effect of RIT on imitation (Ingersoll, 2010). One child in the control group withdrew from the study after pre-treatment assessments due to his family’s busy schedule. One child in the treatment group withdrew after 6 sessions due to the excessive commute to the treatment site (>1 hour each way). This yielded a total of 27 children included in the final data analysis. Neither child’s scores on any of the pre-treatment measures were outside of the range of the children who completed the intervention. All children received a clinical diagnosis of autistic disorder (autism) based on DSM-IV-TR criteria from a licensed psychologist and met the cut-off for autism or autism spectrum disorder on the Autism Diagnostic Observation Schedule-Generic (ADOS-G; Lord et al., 2000). See Table 1.
Table 1.
Participant Characteristics
| Group M (SD) | P-Value | ||
|---|---|---|---|
| Treatment (n=14) | Control (n=13) | ||
| Gender (% Male) | 93% | 85% | n.s. |
| Ethnicity (% Minority Status) | 36% | 39% | n.s. |
| Chronological Agea | 39.3 (7.3) | 36.5 (8.0) | n.s. |
| (range) | (22–47) | (26–47)) | |
| Nonverbal Mental Agea (Bayley) | 20.8 (6.6) | 17.9 (7.5) | n.s. |
| (range) | (8–30) | (7–30) | |
| Expressive Language Agea (PLS-4) | 17.3 (5.5) | 16.2 (5.9) | n.s. |
| (range) | (9–23) | (6–23) | |
| Outside Intervention per Weeka | 11.0 (8.1) | 13.2 (8.8) | n.s. |
| (range) | (1.25–25.5) | (.25–25) | |
months
hours
Design and Procedure
Children were administered standardized assessments of cognitive, language, and social functioning at pre-treatment. Children were matched within three months on expressive language age on the Preschool Language Scale, 4th Edition (PLS-4; Zimmerman, Steiner, & Pond, 2002) and randomly assigned to the treatment (n=14) or control group (n=13) using a coin flip. Children in the treatment group received 3 hours per week of RIT for 10 weeks and children in the control group received treatment as usual in the community. All children continued to receive their existing educational programming throughout the study. Programming involved a variety of interventions, including special education/early intervention services, speech-language pathology services, occupational therapy, in-home applied behavior analysis. There were no differences between groups in number of hours or type of outside therapy received.
Dependent Measures
Two social measures were administered at pre-treatment, post-treatment, and 2- to 3-month follow-up to determine the effect of RIT on social development. The Early Social Communication Scales (ESCS; Seibert, Hogan, & Mundy, 1982) uses a series of activities and adult prompts to examine the child’s ability to engage in social interaction with the examiner. The ESCS was administered by masters’ level clinicians. With a few exceptions, the same examiner administered the ESCS for each child at all three time points. The children’s total number of lower and higher level joint attention initiation bids was used as measure of initiation of joint attention (IJA). Reliability was calculated by two independent raters on 25% of the observations using percent agreement [(smaller number/larger number) X 100), yielding agreement of 80% (range 40–100%).
The Social-Emotional Scale of the Bayley Scales of Infant Development, 3rd Edition (Bayley, 2005) was administered only at pre-treatment and follow-up. The Social-Emotional Scale is a standardized parent-report measure of social and emotional development that was adapted from the Greenspan Social-Emotional Growth Chart (Greenspan, 2004). It assesses acquisition of social and emotional milestones in young children, including self-regulation and interest in the world, communicating needs, engaging others and establishing relationships, using emotions in an interactive, purposeful manner, and using emotional signals or gestures to solve problems (Bayley, 2005). The score for one child in the control group was missing for this assessment at follow-up.
Two imitation measures were administered at pre- and post-treatment and were used in the mediation analysis1. The Motor Imitation Scale (MIS; (Stone, Ousley, & Littleford, 1997) included 8 object and 8 gesture imitation tasks administered in a structured setting. The Unstructured Imitation Assessment (Ingersoll, 2010) included 10 object and 10 gesture imitation tasks administered in a social context. Responses for both measures were scored on a 3-point scale: a “2” was recorded if the child produced an exact imitation, a “1” was recorded if the child produced an emerging response (e.g., the child attempted to manipulate the toy in the correct manner, but failed to complete the act exactly as modeled), and a “0” was recorded if the child failed to imitate. For each action, only the best trial was recorded. Scores could range from 0–32 for the MIS and 0–40 for the UIA. Reliability was calculated by two independent raters on 25% of the observations. Cohen’s Kappa collapsed across items and participants was .93 for the MIS and .84 for the UIA.
Treatment
Children in the treatment group received RIT targeting object and gesture imitation2 one hour per day, three days per week for 10 weeks. Treatment was conducted in a small room with pairs of identical play materials. RIT uses several naturalistic techniques to teach imitation during social interaction with a responsive partner. To promote reciprocity, the therapist contingently imitated the child’s verbal and nonverbal behavior, described the child’s actions using simplified language, and expanded the child’s utterances. To teach imitation, the therapist modeled an action, either with an object or a gesture, once a minute on average. Actions were modeled up to three times, paired with a verbal marker describing the action. If the child did not imitate the action within 10 seconds of the third model, the therapist physically prompted the child to complete the action. The therapist praised the child for imitation and returned to using contingent imitation and describing the child’s play. Other social behavior, including initiation of joint attention, was not prompted or systematically reinforced.
Therapist Training and Fidelity of Implementation
All therapy was conducted by undergraduate and graduate-level research assistants. Each child worked with at least three different therapists throughout treatment to promote generalization. Therapists were trained to 90% correct implementation in RIT through didactic presentation, observation of the intervention techniques, and feedback from experienced masters’ level clinicians during their first several sessions. Fidelity of implementation was scored on 10% of the sessions using the RIT Fidelity Form (Ingersoll & Lalonde, 2010). Fidelity of implementation was high across sessions (mean=4.7 out of 5; range=3.3–5.0).
Results
Primary Data Analysis
The children’s performance on each measure was compared for the two groups using a mixed model ANOVA with time (pre, post, follow-up) as the within group variable and group (treatment vs. control) as the between group variable. There was a main effect of group, F(1,25)=4.90, p<.05, ηp2=.16 on joint attention initiations on the ESCS, such that the treatment group had a higher frequency of joint attention initiations than the control group. This main effect was driven by a significant time by group interaction, F(2,50)=3.78, p<.05, ηp2=.13 such that treatment group made more gains in joint attention initiations than the control group over time. Post hoc comparisons of the simple effects showed that the treatment group made significantly more joint attention initiations at follow-up than pre-treatment (p<.05). The treatment group also made significantly more joint attention initiations than the control group at post-treatment (p<.05) and follow-up (p<.05). See Figure 1.
Figure 1.

Initiation of Joint Attention on the ESCS at Pre-Treatment, Post-Treatment, and Follow-up by Group. Error bars represent standard error.
There was a significant main effect of time, F(1,24)=30.28, p<.01, ηp2=.56 for the Social-Emotional Scale, such that parents rated their children higher at follow-up than pre-treatment. There was also a significant time X group interaction, F(1,24)=6.20, p=.02, ηp2=.21, indicating that the treatment group made substantially more gains on this measure at follow-up than the control group. Post-hoc tests of simple effects suggested that both the treatment (p<.001) and the control group (p<.05) had higher scores on the Social-Emotional Scale at follow-up than pre-treatment. See Figure 2.
Figure 2.
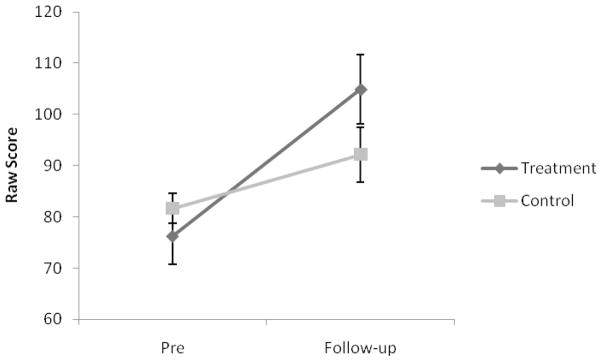
Social-Emotional Functioning on the Social-Emotional Scale at Pre-Treatment and Follow-up by Group. Error bars represent standard error.
Secondary Data Analysis
To examine whether changes in imitation were responsible for improvement in social functioning, a mediation analysis was conducted using the Sobel test described by Baron and Kenny (1986). We converted the two social measures to z-scores and combined them to produce a single measure of social functioning at pre-treatment and follow-up. We created a change score by subtracting the pre-treatment from the follow-up score. We conducted the same procedure with our imitation measures to produce an overall measure of change in imitation from pre- to post-treatment. Statistical mediation can be said to occur if: 1) the treatment is related to change in the outcome (social functioning); 2) the treatment has an effect on the proposed mediator (imitation); 3) the mediator is related to therapeutic change; 4) The relation between the intervention and therapeutic change is reduced after statistically controlling for the proposed mediator (Kazdin & Nock, 2003). Although the first three criteria of mediation were met, the fourth criterion was not, z=-.81, n.s., leading us to retain the null hypothesis3.
Discussion
This study examined the effect of a focused imitation intervention on social functioning in young children with autism. Children in the treatment group made significantly greater gains in their initiation of joint attention at post-treatment and follow-up than the control group. Further, the children in the treatment group made greater gains in social-emotional functioning at follow-up than the control group. These findings replicate and extend our previous findings of collateral improvements in social behavior as a result of RIT (Ingersoll & Schreibman, 2006) using a more controlled design and standardized measures of social functioning.
Although we found evidence for an effect of the treatment on social functioning, the hypothesized mechanism of this effect, improvement in imitation, was not supported by the mediation analysis. One possibility is that we were underpowered to detect an effect of mediation due to our relatively small sample. However, an alternative explanation is that the intervention was responsible for gains in social functioning via some other mechanism. RIT targets the two components of imitation that are involved in reciprocal imitation: Imitation production and imitation recognition. There is limited research on imitation recognition in children with autism. What has been done suggests that there is some evidence that they can recognize when their actions are being imitated as indicated by social signaling, as well as increased attention to and “testing” of the examiner (Nadel, 2002). However, children with autism appear to be less responsive to being imitated than typical children or children with developmental delay (Lewy & Dawson, 1992), and, unlike typical infants, do not tend to show an understanding of the imitator’s intention to imitate (Nadel, 2002). These findings suggest a possible impairment in imitation recognition in young children with autism. There is also evidence that prolonged imitation of their behavior can increase social responsiveness and coordinated joint attention in children with autism, suggesting that imitation recognition is responsive to intervention (Escalona, Field, Nadel, & Lundy, 2002; Tiegerman & Primavera, 1984). In our previous single-case study, we found gains in coordinated joint attention in the first phase of treatment which involved only contingent imitation and linguistic mapping (Ingersoll & Schreibman, 2006), suggesting that the beneficial effect of RIT on social behavior may be due, at least in part, to the intervention’s effect on imitation recognition. Research that can examine this possibility is necessary.
This possibility leads us to question whether direct instruction in imitation production is necessary to achieve gains in social functioning. Several findings lead us to conclude that it is. First, previous research has shown only short-term benefits of contingent imitation; its removal resulted in a return to baseline rates of eye gaze (Dawson & Galpert, 1990) and attention to therapist (Harris, Handleman, & Fong, 1987). In our study, gains in joint attention skills were found on a separate behavioral measure administered outside of the treatment context (i.e., not during contingent imitation) both at post-treatment and at a two- to three-month follow-up. Second, treatment gains were also found on a parent report measure that assesses a wider range of social skills than those identified in previous studies of contingent imitation. Both of these findings suggest that other aspects of the intervention were important for supporting continued social development (Ingersoll & Schreibman, 2006). Third, (Nadel & Peze, 1993) found that contingent imitation alone did not teach role switching in children with autism. In typical development, it is this alternation between being the imitator and the imitatee that conveys social interest in a partner (Nadel, 2002; Uzgiris, 1981) and lays the foundation for more sophisticated social exchanges (Eckerman, Davis, & Didow, 1989). Future dismantling research is needed to determine the active treatment components, both for teaching imitation, the primary target of the intervention, as well as social interaction.
There are several limitations to this study that should be acknowledged. The therapists, examiners, and parents were not blind to the children’s group assignment and the control group did not receive an active treatment. These aspects may have affected the expectancies of the parents or examiners. In addition, all of the children continued to receive their existing educational programs, which involved various combinations of special education/early intervention, speech, occupational therapy, and in–home ABA. Although the groups did not differ in the type and amount of services received per parent report, it is unclear which specific skills and treatment strategies were being used. Thus, it is possible that the groups did differ in some important ways on these variables or that the services that the treatment group received interacted with the intervention in this study, enhancing child response. Finally, this study only followed participants for two to three months post-treatment. It is hoped that the gains observed in social functioning in the treatment group would continue over time; however, additional research regarding the longer term efficacy of this approach for improving social functioning is needed.
In sum, our findings suggest that that a low-intensity, focused intervention targeting imitation can significantly improve autism-specific deficits in social functioning that sustain (or continue to improve) two to three months after program completion. It also adds to the growing body of literature which suggests that short-term focused interventions can lead to broader improvement in developmental skills in children with autism (Kasari, Paparella, Freeman, & Jahromi, 2008). In this study, gains in social functioning could not be attributed to the intervention’s effect on the children’s imitation; rather, social improvements were likely result of the intervention’s effect on some other behavior, possibly imitation recognition. Research on the longer term effects of the intervention on wider range of social behavior is needed.
Acknowledgments
This study was funded by a treatment grant from Autism Speaks (#ASCN5020). I would like to thank the families who participated in this research. I am also grateful to Nikki Bonter and the many research assistants who helped with data collection.
Footnotes
Outcome data based on the imitation measures were reported elsewhere (Ingersoll, 2010).
Gestures were not targeted for 3 children due to their low developmental age (<15 months).
Given our small sample size, we also used the bootstrapping multivariate extension of the Sobel test developed by (Preacher & Hayes, 2004) to test for mediation. The results were unchanged.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington: American Psychiatric Association; 2000. text revision. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of personality and social psychology. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bayley N. Bayley Scales of Infant and Toddler Development. 3. San Antonio, TX: Psychological Corporation; 2005. [Google Scholar]
- Dawson G, Galpert L. Mothers’ use of imitative play for facilitating social responsiveness and toy play in young autistic children. Development and psychopathology. 1990;2(15):1–162. [Google Scholar]
- Eckerman CO, Davis CC, Didow SM. Toddlers’ emerging ways of achieving social coordinations with a peer. Child Development. 1989;60(2):440–453. [PubMed] [Google Scholar]
- Escalona A, Field T, Nadel J, Lundy B. Brief report: Imitation effects on children with autism. Journal of Autism and Developmental Disorders. 2002;32(2):141–144. doi: 10.1023/a:1014896707002. [DOI] [PubMed] [Google Scholar]
- Greenspan SI. Greenspan social-emotional growth chart: A screening questionnaire for infants and young children. PsychCorp 2004 [Google Scholar]
- Harris SL, Handleman JS, Fong PL. Imitation of Self-Stimulation. Child & family behavior therapy. 1987;9(1):1–21. [Google Scholar]
- Ingersoll B. The social role of imitation in autism: Implications for the treatment of imitation deficits. Infants & Young Children. 2008;21(2):107–119. [Google Scholar]
- Ingersoll B, Lewis E, Kroman E. Teaching the imitation and spontaneous use of descriptive gestures in young children with autism using a naturalistic behavioral intervention. Journal of Autism and Developmental Disorders. 2007;37(8):1446–1456. doi: 10.1007/s10803-006-0221-z. [DOI] [PubMed] [Google Scholar]
- Ingersoll B, Schreibman L. Teaching reciprocal imitation skills to young children with autism using a naturalistic behavioral approach: effects on language, pretend play, and joint attention. Journal of Autism and Developmental Disorders. 2006;36(4):487–505. doi: 10.1007/s10803-006-0089-y. [DOI] [PubMed] [Google Scholar]
- Ingersoll B. Brief Report: Pilot randomized controlled trial of Reciprocal Imitation Training for teaching elicited and spontaneous imitation to children with autism. Journal of Autism and Developmental Disorders. 2010;40:1154–1160. doi: 10.1007/s10803-010-0966-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Paparella T, Freeman S, Jahromi LB. Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology. 2008;76(1):125–137. doi: 10.1037/0022-006X.76.1.125. [DOI] [PubMed] [Google Scholar]
- Kazdin AE, Nock MK. Delineating mechanisms of change in child and adolescent therapy: Methodological issues and research recommendations. Journal of Child Psychology and Psychiatry. 2003;44(8):1116–1129. doi: 10.1111/1469-7610.00195. [DOI] [PubMed] [Google Scholar]
- Lewy AL, Dawson G. Social stimulation and joint attention in young autistic children. Journal of Abnormal Child Psychology. 1992;20(6):555–566. doi: 10.1007/BF00911240. [DOI] [PubMed] [Google Scholar]
- Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, DiLavore PC, Pickles A, et al. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders. 2000;30(3):205–223. [PubMed] [Google Scholar]
- McDuffie A, Turner L, Stone W, Yoder P, Wolery M, Ulman T. Developmental correlates of different types of motor imitation in young children with autism spectrum disorders. Journal of autism and developmental disorders. 2007;37(3):401–412. doi: 10.1007/s10803-006-0175-1. [DOI] [PubMed] [Google Scholar]
- Nadel J. Imitation and imitation recognition: Functional use in preverbal infants and nonverbal children with autism. In: Meltzoff AN, Prinz W, editors. The imitative mind: development, evolution and brain bases. Cambridge, UK: Cambridge University Press; 2002. pp. 42–32. [Google Scholar]
- Nadel J, Peze A. What makes immediate imitation communicative in toddlers and autistic children. In: Nadel J, Camaioni L, editors. New perspectives in early communicative development. New York: Routledge; 1993. pp. 139–156. [Google Scholar]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments, & Computers. 2004;36(4):717. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- Rogers SJ. An examination of the imitation deficit in autism. In: Nadel J, Butterworth G, editors. Imitation in infancy. Cambridge: Cambridge University Press; 1999. pp. 254–279. [Google Scholar]
- Rogers SJ, Pennington BF. A theoretical approach to the deficits in infantile autism. Development and Psychopathology. 1991;3(2):137–162. [Google Scholar]
- Seibert JM, Hogan AE, Mundy PC. Assessing interactional competencies: The early social-communication scales. Infant Mental Health Journal. 1982;3(4):244–245. [Google Scholar]
- Smith IM, Bryson SE. Imitation and action in autism: A critical review. Psychological Bulletin. 1994;116:259–259. doi: 10.1037/0033-2909.116.2.259. [DOI] [PubMed] [Google Scholar]
- Stone WL, Ousley OY, Littleford CD. Motor imitation in young children with autism: What’s the object? Journal of Abnormal Child Psychology. 1997;25(6):475–485. doi: 10.1023/a:1022685731726. [DOI] [PubMed] [Google Scholar]
- Tiegerman E, Primavera LH. Imitating the autistic child: Facilitating communicative gaze behavior. Journal of Autism and Developmental Disorders. 1984;14(1):27–38. doi: 10.1007/BF02408553. [DOI] [PubMed] [Google Scholar]
- Uzgiris IC. Two Functions of Imitation During Infancy. International Journal of Behavioral Development. 1981;4(1):1–12. [Google Scholar]
- Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scale. 4. San Antonio, TX: The Psychological Corporation; 2002. [Google Scholar]