

Abstract
The biology and outcome of adult t(4;11)(q21;q23)/MLL-AFF1 acute lymphoblastic leukemia are poorly understood. We describe the outcome and delineate prognostic factors and optimal post-remission therapy in 85 consecutive patients (median age 38 years) treated uniformly in the prospective trial UKALLXII/ECOG2993. The immunophenotype of this leukemia was pro-B (CD10NEG). Immaturity was further suggested by high expression of the stem-cell antigens, CD133 and CD135, although CD34 expression was significantly lower than in t(4;11)-negative patients. Complete remission was achieved in 77 (93%) patients but only 35% survived 5 years (95% CI: 25–45%); the relapse rate was 45% (95% CI: 33–58%). Thirty-one patients underwent allogeneic transplantation in first remission (15 sibling donors and 16 unrelated donors): with 5-year survival rates of 56% and 67% respectively, only 2/31 patients relapsed. This compares with a 24% survival rate and 59% relapse rate in 46 patients who received post-remission chemotherapy. A major determinant of outcome was age with 71% of patients aged <25 years surviving. Younger patients had lower relapse rates (19%) but most received allografts in first complete remission. In conclusion, multivariate analysis did not demonstrate an advantage of allografting over chemotherapy but only five younger patients received chemotherapy. Prospective trials are required to determine whether poor outcomes in older patients can be improved by reduced-intensity conditioning allografts. NCT00002514 www.clinicaltrials.gov
Introduction
The therapy of adults with acute lymphoblastic leukemia (ALL) remains inadequate.1,2 Certain groups with adverse prognostic factors have a particularly poor outcome. The UKALLXII/ECOG2993 study was the most extensive cytogenetic analysis of adult ALL performed to date3,4 but there was no specific, detailed analysis of t(4;11)(q21;q23)/MLL-AFF1 which accounts for 8–10% of B-cell precursor (BCP) ALL in patients over the age of 20 years.5 Most major cooperative groups have regarded this subset of patients as having a poor prognosis but no group has had a sufficiently large dataset to examine the biological factors affecting outcome and whether allografting in first remission might be associated with an improved outcome. Furthermore, previous studies had too few patients to examine the relevance of age in clinical decision-making.
The MLL gene, located on the long arm of chromosome 11, has been found to be rearranged with over 70 partner genes in ALL, acute myeloid leukemia and therapy-related leukemia.6 The most common translocation involving this gene in ALL is t(4;11)(q21;q23)5 which is the second most common translocation in adult ALL overall. The age-specific incidence of this translocation is unique and shows a bimodal distribution, occurring in 40–50% of infants with ALL, 2–3% of children and adolescents but ~10% of adults over 20 years old.5 The very high incidence in infants, especially among those under 6 months of age, suggests that the latency period for this subtype of leukemia can be very short.7 Studies have shown that in these cases the gene fusion arises prenatally.8 While infants and adults with t(4;11) have a poor outcome compared to other patients of a similar age, there is some evidence to suggest that children and adolescents with this translocation may have a marginally better relative outcome.3,7,9 Genomic studies have so far revealed very few additional copy number alterations in this subtype of leukemia especially among infants.10–12 Overall, somatic sequence mutations are also relatively rare in MLL-rearranged childhood ALL but RAS pathway gene mutations do appear to play a role in a significant minority of patients.13–15 In contrast, methylation changes in MLL-rearranged infant and childhood ALL are widespread and distinctive.16 Integrative epigenomic analysis of a subset of adults with MLL rearrangements in the ECOG2993 trial recently showed that these leukemias feature prominent cytosine hypomethylation, which was linked with MLL fusion protein binding.17 The prognostic impact of secondary genetic and epigenetic alterations has yet to be fully elucidated in infant and childhood t(4;11)-positive ALL and has rarely been investigated in adult ALL.
Our study describes the largest cohort of adults with t(4;11)-positive ALL so far treated uniformly in a single prospective randomized trial. This report focuses on the clinical features, cytogenetic and molecular changes, immunophenotype and outcome of these patients.
Design and Methods
Identification of patients
A total of 85 adult patients with BCP-ALL and t(4;11) were registered in the UKALLXII/ECOG 2993 study in the United Kingdom (UK) (n=57) or United States of America (USA) (n=28) between 1993 and 2006. Over 1900 patients in total were entered into this study. The number of patients with Philadelphia-negative BCP-ALL tested for t(4;11) was 913, which results in an incidence of 85/913 (9.3%).
Immunophenotyping
Central immunophenotyping was performed in the ECOG Leukemia Translational Studies Laboratory for ECOG2993 patients. Similar studies were not performed on patients in the UKALLXII study. Between 1993 and 1998, flow cytometry was done on a FACScan flow cytometer (Lysys II software), and from 1999 on a FACSCalibur flow cytometer (CellQuest software) (all from Becton-Dickinson, San Jose, CA, USA). Lymphoblasts were gated by three-color flow cytometry based on antigen expression of the leukemic cells. B-lymphoid antigens included intracytoplasmic and surface CD22, CD19, CD10, CD24 and CD20. Myeloid antigens included myeloperoxidase, CD117, CD33, CD13, CD65(s), CD15(s), CD11b and CD14. Lineage-uncommitted antigens CD45, CD38, CD56, HLA-DR, and TdT (Supertechs) were also analyzed. Stem-cell antigens tested included CD34, CD117, CD135, CD133, CD105, CD123 and CD109. Antigen data are presented as percent positive leukemic blast cells or as the mean fluorescence intensity ratio of staining after binding of the various antibodies (MFI) and that of unstained cells, as described elsewhere.4
Cytogenetic, fluorescence in situ hybridization, multiplex ligation-dependent probe amplification and molecular genetic investigations
Cytogenetic and fluorescence in situ hybridization (FISH) analysis of pre-treatment bone marrow or peripheral blood samples was performed locally, reviewed centrally, and collated retrospectively using standard definitions as previously described.3 Central screening for MLL-AFF1 was performed for ECOG2993 patients by the Leukemia Translational Studies Laboratory using reverse transcriptase polymerase chain reaction (RT-PCR) and standard primers as previously described.18 Among the 85 t(4;11)-positive patients presented the abnormality was detected by a combination of techniques: cytogenetics and FISH (n=30), cytogenetics only (n=23); cytogenetics and RT-PCR (n=21), RT-PCR only (n=8), and all three techniques (n=3). The presence of additional copy-number alterations was determined by multiplex ligation-dependent probe amplification (MLPA) in 34 patients using the SALSA MLPA kit P335-A1 (MRC Holland, Amsterdam, The Netherlands).
Therapy and risk assignment
This study (UKALL XII/ECOG 2993) has been described in detail.1 Briefly, all patients from 15 to 59 years of age with newly diagnosed ALL received identical four-drug induction therapy, including central nervous system prophylaxis and treatment of central nervous system disease, if present at diagnosis. In 2003, the upper age limit of the study was raised to 64 years and eligibility for allograft was raised from 49 to 54 years. Patients with an HLA-matched sibling donor were assigned to receive an allogeneic hematopoietic cell transplant. Unrelated donor transplantation in first complete remission was not part of the protocol. The unrelated donor transplants were T-depleted using various Campath antibodies. Those without an HLA-matched sibling donor, or over the age limit, were eligible to be randomized to receive a single autologous transplant or consolidation/maintenance therapy. Prior to receiving the assigned or randomized therapy, all patients received intensification with three doses of high-dose methotrexate and asparaginase. In this study, patients older than 35 years or those with a high white blood cell (WBC) count at presentation (30×109/L for B-lineage) along with all patients with the Philadelphia chromosome were subsequently classified as high risk. All others [including those with t(4;11)] were classified as standard risk. The study was approved by the relevant Institutional Review Boards of each center and informed consent was obtained in accordance with the Declaration of Helsinki.
Statistics and endpoints
Event-free survival and overall survival were defined as the time from the start of treatment to relapse or death and death, respectively. Patients without an event of interest were censored at the date of last contact. Relapse-free survival and non-relapse mortality were determined for patients who achieved a complete remission and were defined as the time from complete remission to relapse/death censoring patients who died in remission/relapsed, respectively. The median follow-up time for event-free, relapse-free and overall survival was 5.4, 3.8 and 5.3 years, respectively. Event-free, relapse-free and overall survival estimates were calculated using the Kaplan-Meier method. The effect of receiving allogeneic hematopoietic cell transplantation in first remission was assessed using a Cox model with a time-varying covariate (the Mantel-Byar approach).19 Survival in subgroups of patients was compared using univariate, stratified and multivariate Cox models and tests for heterogeneity. The proportional hazard assumption was assessed by visual inspection of the log-log plot. Other comparisons were performed using the χ2, Fisher’s exact test or Wilcoxon rank-sum test, as appropriate. Due to the investigative nature of this analysis, we did not apply a stringent multiple comparisons adjustment. However, all tests were conducted at the 1% significance level. All analyses were performed using Intercooled Stata 11.0 for Windows (Stata Corporation, College Station, Texas, USA).
Results
Clinical characteristics
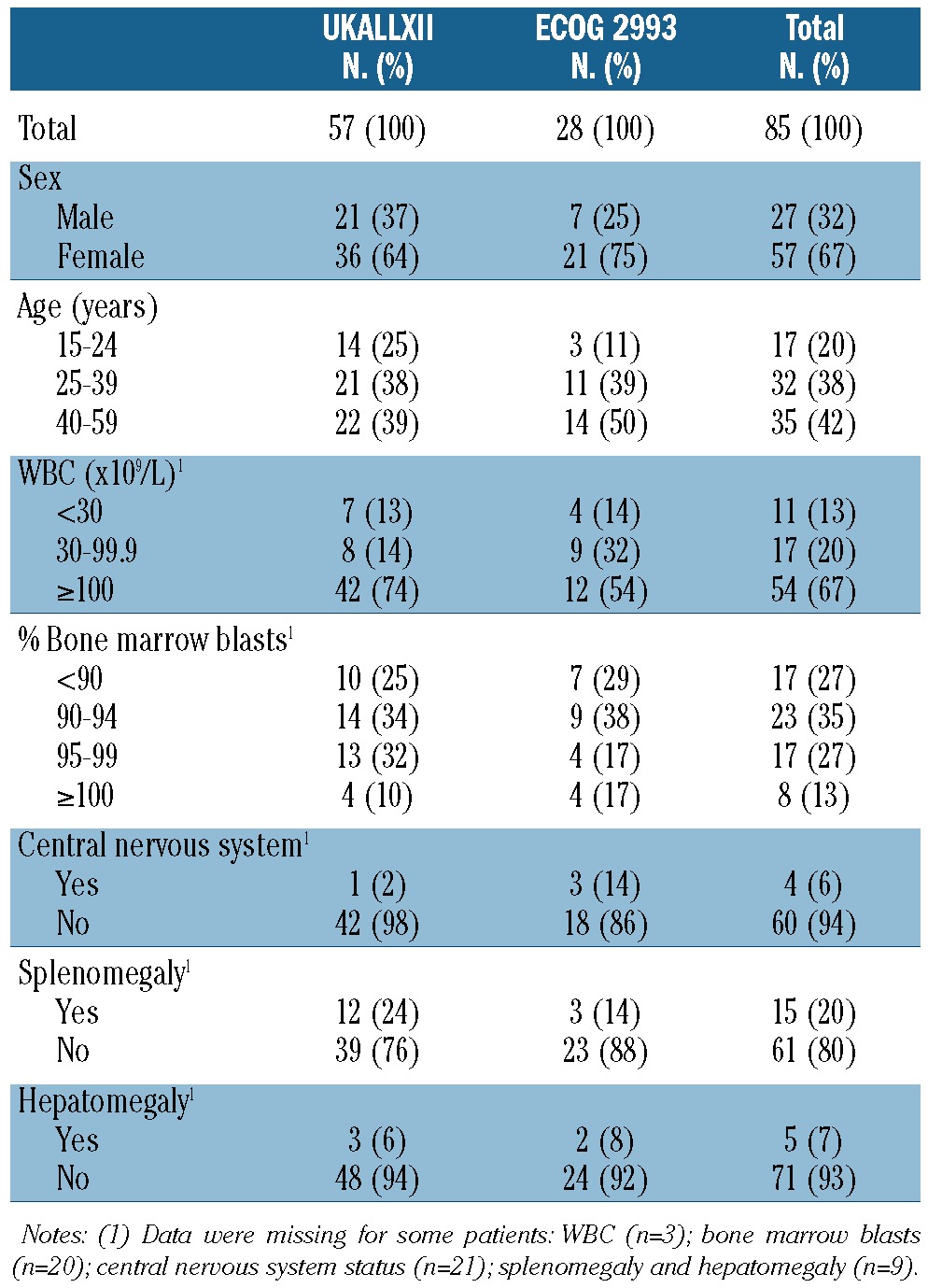
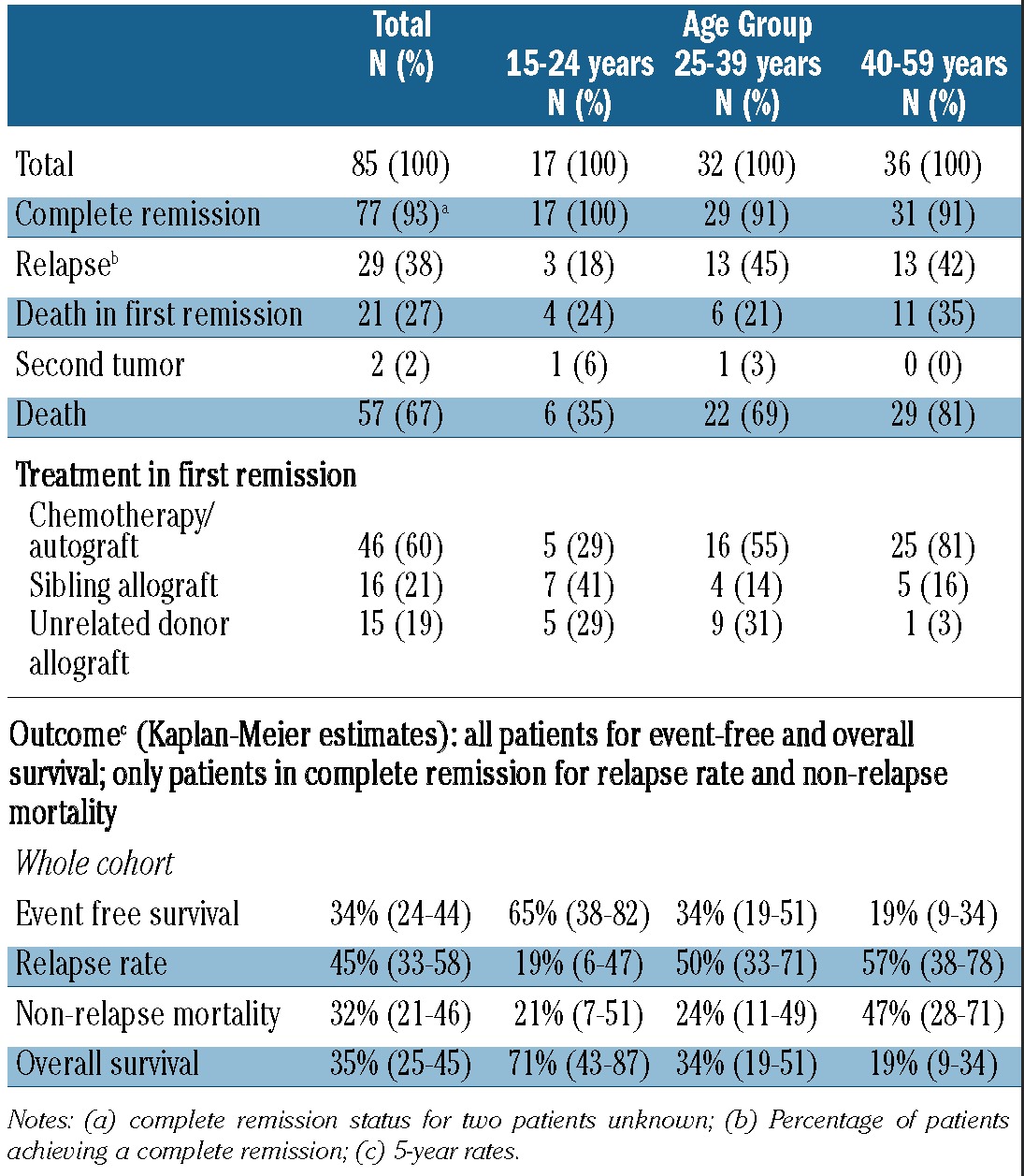
The clinical characteristics of the 85 t(4;11)-positive patients are presented in Table 1. Compared with other BCP-ALL Philadelphia-negative patients in the UKALLXII/ECOG2993 study,3 patients with t(4;11) were more likely to be female, older and have a higher WBC count. The median age of the whole cohort was 38 years (37 years in the UKALLXII patients and 41 years in the ECOG2993 patients). The central nervous system was seen to be involved at diagnosis in 6% of patients.
Table 1.
Demographic and clinical characteristics of 85 adult patients with t(4;11)-positive acute lymphoblastic leukemia.
Immunophenotype
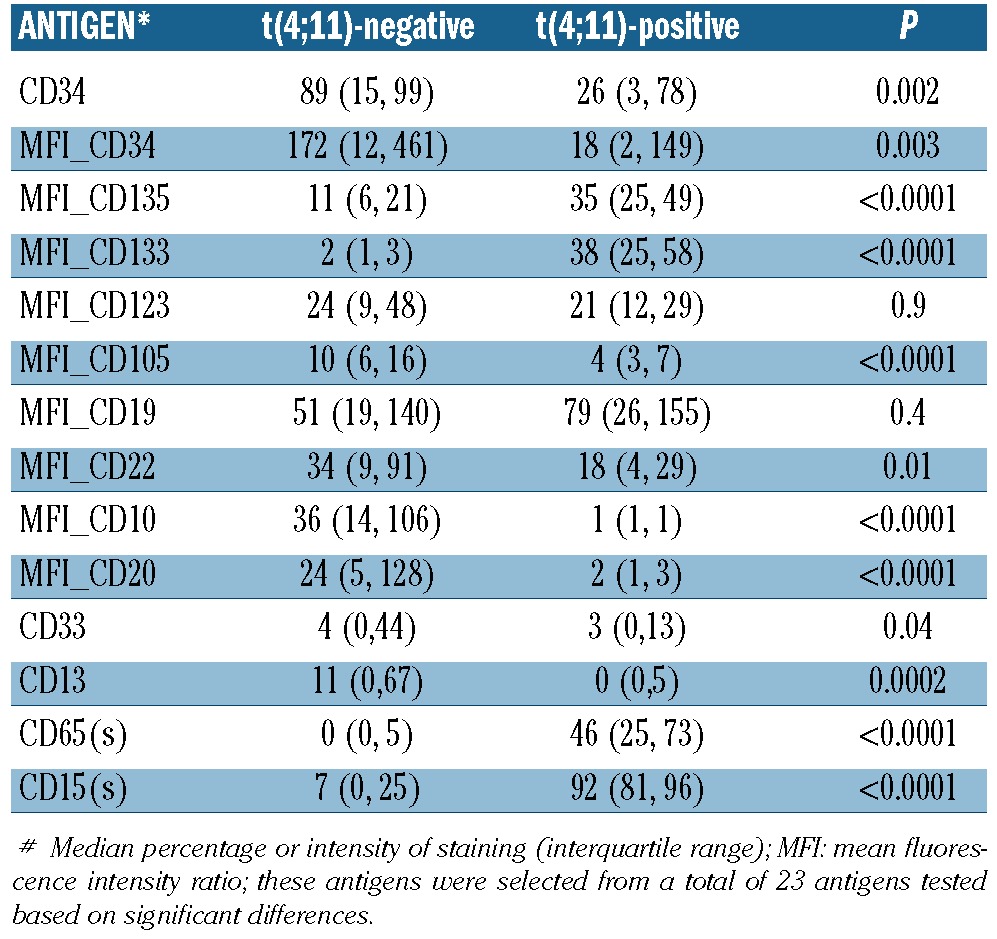
Based on expression of B-lineage maturation antigens,20 22/26 patients tested had a pro-B or pre-pre-B immunophenotype, with expression of surface CD19 and intracytoplasmic CD22 but lacking CD10 expression; one case had early pre-B (CD10POS) and three cases had pre-B (intracytoplasmic μ chainsPOS) ALL. The pro-B phenotype was only seen in 13% of t(4;11)-negative patients in the ECOG2993 trial. The t(4;11)-positive subset had a unique antigen profile when compared to t(4;11)-negative patients (Table 3). None of the cases showed any staining for myeloperoxidase. While the intensity of staining for CD19 (P=0.4) and membrane CD22 (P=0.01) was not significantly different between the subgroups (when adjusted for multiple comparisons), CD20 expression was rare on t(4;11)-positive blasts (P<0.0001), and the intensity of staining for the two stem cell antigens, CD133 and CD135 was high (P<0.0001), suggesting an immature differentiation stage. However, the frequency of blasts expressing the prototype stem cell antigen, CD34, (P<0.0001) as well as their intensity of staining for CD34 (P=0.003) were lower in t(4;11)-positive than in t(4;11)-negative leukemia and the intensity of staining for another progenitor cell antigen, CD123, was not different between the two groups (P=0.9). Interestingly, CD105 (endoglin), an antigen predominantly expressed by myeloerythropoietic progenitors and mesenchymal cells, was present at lower density on the surface of t(4;11)-positive blasts than on t(4;11)-negative one (P<0.0001). As previously reported for CD10NEG ALL20 in general, t(4;11)-positive lymphoblasts showed unique expression of the two myeloid antigens, CD65(S) and CD15(S) (P<0.0001) when compared to t(4;11)-negative cases.
Table 3.
A comparison of the immunophenotypic characteristics of t(4;11)-positive and negative ALL.
Cytogenetic and genetic abnormalities
Additional chromosomal abnormalities were present in 31 (41%) of the 75 patients in whom cytogenetic analysis was successful. The most common additional cytogenetic abnormalities were gain of chromosome X (n=13), i(7)(q10) (n=7) and abnormalities of 1p (n=4). Thirty-four UKALLXII t(4;11)-positive patients were screened by MLPA for deletions of CDKN2A/B, IKZF1, PAX5, ETV6, RB1 and EBF1.12 No deletions at all were detected in 22 (65%) of the patients and none of the patients harbored a deletion of PAX5, ETV6, RB1 or EBF1. Twelve patients had either a deletion of the IKZF gene (n=6) or the CDKN2A/B locus (n=6). All 34 cases tested by MLPA were also successfully tested by cytogenetics and showed t(4;11).
Major outcomes and causes of death
Seventy-seven t(4;11)-positive patients attained a complete remission (93%); remission status was not known for two patients. This complete remission rate is comparable to that in the total population of patients in the trial. All six patients who failed to achieve a complete remission had a WBC count >100×109/L and three of the six were >40 years old. The two patients with unknown remission status died at 28 and 403 days. The complete remission rate by WBC count was 100% (27/27) for patients with a WBC <100×109/L compared to 89% (48/54) for patients with a WBC count >100×109/L (P=0.171). Younger patients were slightly more likely to achieve a complete remission but the difference was not statistically significant. The complete remission rate by age was 17/17 (100%) in patients 15–24 years old, 29/32 (91%) in patients aged 25–39 years and 31/34 (86%) in those 40–59 years old (P=0.641).
A total of 29/77 (38%) patients have relapsed after a median follow-up of 3.8 years. Slightly more ECOG2993 patients than UKALLXII patients relapsed (48% versus 33%, P=0.194). All relapses were isolated bone marrow relapses and all but one of these patients have subsequently died; the sole survivor has been followed up for 1.8 years. The median time to relapse was 335 days and 28/29 relapses occurred within 2 years of diagnosis. The overall 5-year relapse rate was 45% (95% CI: 33–58%).
In total, 57/85 (67%) patients have died, including all eight who did not achieve remission or for whom remission status is not known. Among the 77 patients who achieved a complete remission, 21 (27%) patients died in first remission while 28 (36%) died following a relapse. One female patient aged 33 developed acute myeloid leukemia 5 months after achieving a complete remission and died 5 weeks later of refractory acute myeloid leukemia.
At a median follow up of 5.4 years the 5-year event-free survival was 34% (95% CI: 24–44%) while the overall survival rate was 35% (95% CI: 25–45%). Fifty-five of 58 (94%) events occurred within the first 2 years (Figure 1A,B). The two events occurring after 5 years were related to allogeneic transplantation: graft-versus-host disease and pulmonary complications after an allograft.
Figure 1.
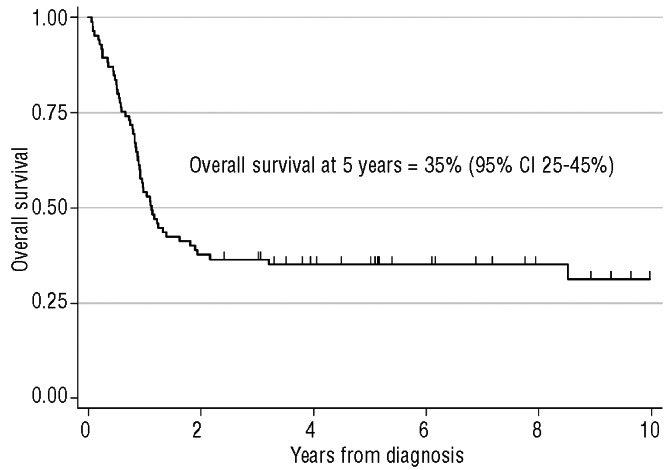
Overall survival of 85 adult patients with t(4;11)-positive acute lymphoblastic leukemia (ALL) treated in the UKALLXII/ECOG2993 study.
Post-remission therapy
Only 25/77 (32%) patients who achieved a complete remission were entered into the randomization to receive either an autograft or continue chemotherapy alone. Of these 25 patients, seven were assigned an autograft with etoposide and total body irradiation conditioning but only one patient received it. The reasons for patients not receiving the autograft are not known. Eleven patients were randomized to chemotherapy and seven other patients were allocated to a sibling allograft with five receiving that allograft. The numbers of patients randomized were insufficient to perform an analysis by randomized allocation.
Analysis was carried out by treatment received (Figure 2). Among the patients who attained a complete remssion, 31 (40%) patients had an allograft in first remission. Hematopoietic cell donors for the allograft were as follows: 16 matched siblings, 14 unrelated donors and one mismatched related donor. The unrelated donor transplants were performed off-study at the discretion of investigators. The remaining 46 (60%) patients received chemotherapy in first remission, although a single patient received an autograft. First remission treatment was closely correlated with age with 12/17 patients aged 15–24 years receiving an allograft compared to 13/29 patients aged 25–39 years and only 6/31 patients aged 40–59 years (P=0.002).
Figure 2.
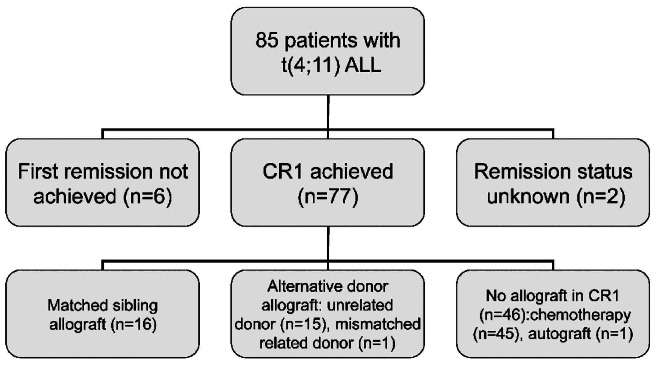
Patient flow chart. CRI: first complete remission.
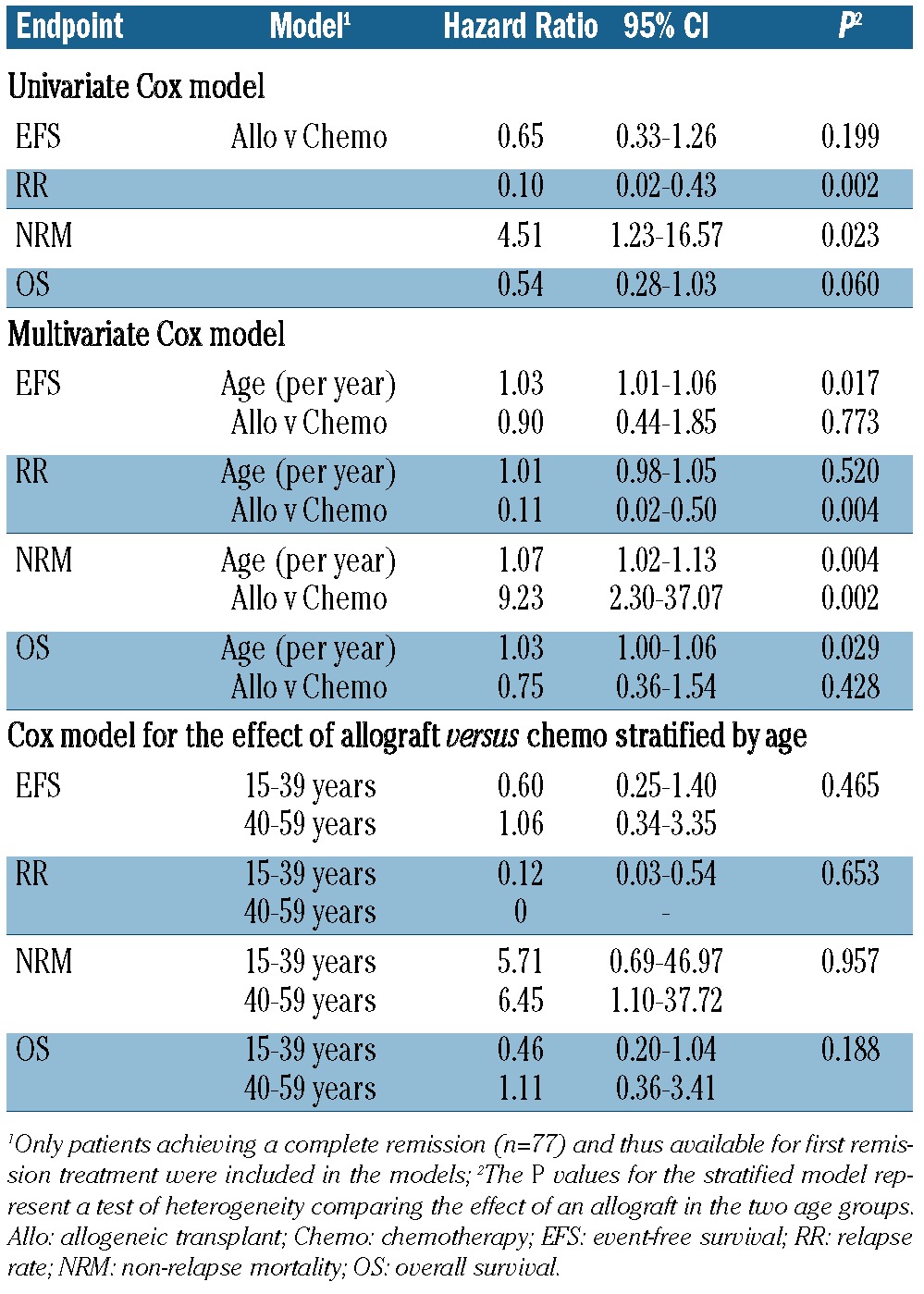
The event-free and overall survival rates of patients according to treatment received in first remission are shown in Figure 3A. Those patients receiving chemotherapy/autograft had a 5-year overall survival rate of 24% (95% CI: 13–37%) and 27/46 (59%) have relapsed. In contrast, the 5-year overall survival rate of the 31 patients who had a sibling donor or unrelated donor allograft was 56% (95% CI: 30–76%) and 67% (95% CI 38–85%), respectively. As the outcome of sibling and unrelated allograft donor groups was similar the groups were combined for analysis. Although Cox regression analysis comparing allograft versus chemotherapy/autograft in first remission showed a hazard ratio (HR) consistent with a benefit for an allograft, the superiority over chemotherapy was not statistically significant for either event-free or overall survival (Table 4). Patients who received an allograft had a very low relapse rate (2/31, 6%) indicating that this is effective anti-leukemic therapy in this high-risk leukemia and providing further evidence of a graft-versus-leukemia effect. Thus the data are highly suggestive that the superior survival observed in the allograft group was due to protection against relapse (Figure 3B).
Figure 3.

(A) Relapse rate and survival of 77 adult patients with t(4;11)-positive acute lymphoblastic leukemia (ALL) treated in the UKALLXII/ECOG2993 study by treatment received in first remission. The 15 patients with unrelated donors include one transplanted from a mismatched related donor. (B) Relapse rate and survival of 85 adult patients with t(4;11)-positive acute lymphoblastic leukemia (ALL) treated in the UKALLXII/ECOG2993 study by age.
Table 4.
Cox regression analysis examining the effect of age and first remission treatment among adult patients with t(4;11)-positive acute lymphoblastic leukemia (ALL).
Five patients aged 15–24 years received chemotherapy alone after achieving first remission and three of these patients remain in complete remission at 3.3, 3.8 and 15 years after diagnosis. The other two patients relapsed and died within 1.5 years of diagnosis, with one having received an allograft in second remission.
Six patients >40 years old received an allograft. Four died of transplant-related causes and none relapsed. Two patients survive more than 3 years after the allograft.
Analysis of prognostic factors affecting major outcomes
We examined the following prognostic factors in relation to complete remission, relapse and death rate: age, sex, WBC count, central nervous system disease, additional cytogenetic abnormalities, gain of chromosome X, i(7q), abnormalities of 1p, IKZF1 deletions, CDKN2A/B deletions, expression of CD34, CD133, CD135 or CD105. Only age showed an association with outcome. However, the power to detect differences associated with specific antigens and additional cytogenetic abnormalities was compromised by the small dataset.
Age at diagnosis was a strong predictor of outcome (Table 2), with increasing risks of relapse and death observed with increasing age. Although the outcome differences by age group were clear cut (Table 2), univariate Cox regression models showed that the adverse effect of age was continuous for risk of relapse, death and any event [HR=1.03/year (1.00–1.07), P=0.046; 1.03/year (1.01–1.06), P=0.002; and 1.04/year (1.01–1.05), P=0.003, respectively], although these findings may be difficult to interpret given the fact that treatment received in first complete remission was also strongly linked to age (Table 2). Multivariate analysis showed that the effect of age was independent of post-remission treatment for both event-free and overall survival (Table 4) and did not show an advantage of allografting over chemotherapy. A stratified analysis did not show a statistically significant difference for the effect of allogeneic hematopoietic cell transplantation between the two age groups (Table 4).
Table 2.
First remission treatment and outcome among 85 adult patients with t(4;11)-positive acute lymphoblastic leukemia by age group.
Discussion
In this study we report on the outcome of the largest cohort of adults with t(4;11)-positive ALL who were uniformly treated on the UKALLXII/ECOG2993 protocol. The complete remission rate in these 85 patients was similar to that of the entire trial population (93%) but only a third of patients survived 5 years because of a high relapse rate. Eighty-six percent had a high diagnostic WBC count and although this did not significantly affect survival it was associated with the failure to achieve first remission. Age was the major determinant of outcome with patients 15–24 years old having very encouraging survival. However, age had clear effects on treatment assignment with most young patients undergoing allogeneic hematopoietic cell transplantation in first remission.
Analysis of the effects of post-remission treatment on the outcome of the 77 patients who achieved a first remission was confounded by a number of factors, not least the role of age in directing therapy. It is not valid to compare the survival of patients who received continuing chemotherapy (24%) with those who had an allograft (>60%) as the latter group was younger and there may have been other selection factors not accounted for in our analyses. A donor versus no donor analysis is also unhelpful as half of the allografted patients had stem cells from an alternative donor. However, there is now considerable evidence that recipients of sibling and unrelated donor grafts achieve similar outcomes in adult ALL and this finding is confirmed by this study, albeit in small numbers. It is important to note that the unrelated donor transplants in first remission occurred off-protocol and it seems likely that patients selected for this intervention were fitter and would have had a well-matched donor available. An important finding was the very low relapse rate in the allografted group (2 of 31 patients), confirming that high-dose chemoradiotherapy and an allogeneic graft-versus-leukemia effect represent the strongest antileukemic therapy in t(4;11) adult ALL. However transplant-related mortality almost reached 30%, affecting both event-free and overall survival in the allografted group and contributing to the finding that allografting was not superior to chemotherapy in multivariate analysis. Lowering transplant-related mortality will constitute the most important way of achieving better outcomes in patients who are allografted.
Too few patients aged 15–24 years were treated with chemotherapy alone to assess the effectiveness of this strategy. Most patients in this age group are now treated on trials using intensive pediatric regimens with minimal residual disease detection guiding treatment assignment. For example, patients with t(4;11) aged 15–24 years old in the newly opened UKALL2011 trial in the UK will be classified as high risk but will not routinely receive allogeneic hematopoietic cell transplantation in first remission. However, patients who have minimal residual disease after 14 weeks of therapy will be taken off study and will receive an allograft. Hence this trial and trials such as the ongoing Cancer and Leukemia Group B ALL Intergroup study C10403 [in which patients with t(4;11) are recommended to have a transplant] should enable us to understand if allografting is necessary in younger patients with t(4;11) who are treated with more ‘pediatric-like’ induction and consolidation regimens. We had insufficient minimal residual disease data to analyze this prognostic variable.
The outcome for patients aged 40–59 years was poor. Intensification of chemotherapy regimens is unlikely to be the solution for patients in this age group because of toxicity. The judicious application of allogeneic hematopoietic cell transplantation in selected fit patients with well-matched donors bears consideration based on the very low relapse rate seen in patients who had myeloablative allografts. Reduced intensity allografts have not been tested prospectively in adults with ALL, particularly in defined high-risk groups such as patients with t(4;11). This approach is being assessed in the UKALL14 study but the low incidence of this cytogenetic abnormality may make it difficult to draw definitive conclusions. It is worth noting that the two major studies of reduced intensity conditioned allografts in adults with ALL suggest a higher relapse rate with this reduced intensity conditioning than full intensity allografts.21,22
The outcome after relapse was extremely poor, confirming the results of our previous study.23 More effective salvage strategies such as blinatumamab and inotuzamab deserve study in this group of patients.24,25 Until there are effective salvage therapies for patients with relapse, allografting will have to be considered for all adults with high-risk ALL.
Detailed immunophenotypic analysis of 27 patients confirmed the known prevalence of the CD10NEG, immature differentiation stage in t(4;11)-positive ALL.26 These data correlate with those of our previous analysis of antigen receptor genes in this cohort of UKALLXII patients which indicated that the t(4;11) translocation arises in an immature cell.27 The dual presence of myeloid antigens CD15(S) and CD65(S) is, however, a feature of all CD10 NEG B-lineage cases and not restricted to those with t(4;11).20,28 Contrary to earlier reports,12 we found CD33 and CD13 to be expressed by significantly fewer lymphoblasts in t(4;11)-positive ALL than in other Philadelphia-negative BCP-ALL. We expanded on the characteristic stem cell antigen signature of t(4;11)-positive ALL, namely CD133 high/CD34 low expression, previously proposed in pediatric ALL,29 by showing overexpression also of CD135 and CD105, while CD123 was present though non-discriminating. The high intensity of CD135 expression (FLT3) is in agreement with our gene expression data from the ECOG2993 trial17 and findings in pediatric MLL-positive BCP-ALL.30 Although CD133 is overexpressed on CD34+ cells in normal hematopoietic tissue, functional studies have revealed that a very rare population of CD133+CD34−CD38−Lin−cells have long-term in vitro and in vivo repopulating abilities.30
The pathogenesis of MLL-positive ALL is likely to be a multistep process requiring the acquisition of several secondary genetic and/or epigenetic alterations. However, emerging data suggest that t(4;11)-positive ALL may be different because the reciprocal gene product – AFF1-MLL - also has leukemogenic properties.6 While this hypothesis is substantiated by the short latency period observed in infant t(4;11)-positive ALL, the possible re-emergence of this abnormality in adult ALL is an intriguing observation and one that warrants further investigation. Studies investigating the prognostic impact of secondary genetic and epigenetic alterations in t(4;11)-positive ALL have largely been confined to infant and childhood ALL and, moreover, have been mostly inconclusive. In this study, we were able to investigate both additional chromosomal abnormalities and to characterize the most prevalent copy number alterations observed in ALL in our study population. In keeping with previous studies, we found that t(4;11) ALL harbors few recurrent genomic alterations.10,11,31,32 Further studies are needed to assess the incidence and clinical relevance of sequence mutations (especially those affecting the RAS pathway). In contrast to the lack of genomic aberrations observed in these patients, epigenetic dysregulation in MLL-rearranged leukemia appears to be widespread and specific methylation signatures have been reported for MLL-rearranged leukemias as a whole and also within different translocation subgroups.16,17,33 In particular, the histone methyltransferase DOT1L has been shown to play a pivotal role in leukemogenesis in MLL-rearranged cases and in vitro studies have demonstrated sensitivity to targeted inhibition.33,34 A phase I study of an DOT1L inhibitor (EPZ-5676) has recently been announced raising the prospect of a targeted therapeutic strategy for this poor-risk subgroup. Additional therapeutic possibilities have emerged from our recent study which demonstrated that adult t(4;11)-positive ALL displays a unique DNA methylation signature with predominant hypomethylation, resulting in transcriptional up-regulation and over-expression of several oncogenes including BCL6.17
In summary t(4;11)-positive ALL in adults has a slightly poorer outcome than B-cell precursor ALL overall although that outcome is highly dependent upon age. Allogeneic hematopoietic cell transplantation offers excellent outcomes in younger patients and may have a part to play in the management of t(4;11)-ALL but its precise role requires further exploration in different age groups in prospective trials. We again confirm that effective therapy for relapse represents a major unmet need in adult ALL. Finally, studies that attempt to elucidate the biology of this disease may enable us to develop more individualized and targeted therapies.
Acknowledgments
We thank all the patients for agreeing to take part in this clinical trial. AVM, CJH, AE, and LAC would like to thank the Leukemia & Lymphoma Research for financial support. We thank the MRC for the grant (G8223452) which funded the UK trial management. We would also like to acknowledge the support of the member laboratories of the United Kingdom Cancer Cytogenetic Group (UKCCG) for providing cytogenetic data and material and past and present members of the Leukaemia Research Cytogenetics Group (LRCG) for their contribution to establishing this dataset. We thank all the members of the Adult Leukaemia Working Party during this period, and all the doctors who entered patients into the trial. We also thank Dr Sue Richards and Dr Georgina Buck (Clinical Trial Service Unit, University of Oxford) for data management and statistical input.
Footnotes
Funding
This study was coordinated in the USA by the Eastern Cooperative Oncology Group (Robert L. Comis, M.D., Chair) and supported in part by Public Health Service Grants CA23318, CA66636, CA21115, CA14958, CA13650, CA14588, CA17145, and CA14548 from the National Cancer Institute, National Institutes of Health and the Department of Health and Human Services. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Cancer Institute.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Goldstone AH, Richards SM, Lazarus HM, Tallman MS, Buck G, Fielding AK, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993). Blood. 2008;111 (4):1827–33 [DOI] [PubMed] [Google Scholar]
- 2.Rowe JM, Buck G, Burnett AK, Chopra R, Wiernik PH, Richards SM, et al. Induction therapy for adults with acute lymphoblastic leukaemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG 2993. Blood. 2005;106(12):3760–7 [DOI] [PubMed] [Google Scholar]
- 3.Moorman AV, Harrison CJ, Buck GA, Richards SM, Secker-Walker LM, Martineau M, et al. Karyotype is an independent prognostic factor in acute lymphoblastic leukaemia: analysis of cytogenetic data from patients treated on the MRC UKALL XII/ECOG 2993 trial. Blood. 2007;109(8): 3189–97 [DOI] [PubMed] [Google Scholar]
- 4.Marks DI, Paietta EM, Moorman AV, Richards SM, Buck G, DeWald G, et al. T-cell acute lymphoblastic leukemia in adults: clinical features, immunophenotype, cytogenetics, and outcome from the large randomized prospective trial (UKALL XII/ECOG 2993). Blood. 2009;114(25): 5136–45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moorman AV. The clinical relevance of chromosomal and genomic abnormalities in B cell precursor acute lymphoblastic leukaemia. Blood Rev. 2012;26(3):123–35 [DOI] [PubMed] [Google Scholar]
- 6.Pieters R, Schrappe M, De Lorenzo P, Hann I, De Rossi G, Felice M, et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (Interfant-99): an observational study and a multicentre randomised trial. Lancet. 2007; 370(9583):240–50 [DOI] [PubMed] [Google Scholar]
- 7.Greaves M. Pre-natal origins of childhood leukemia. Rev Clin Exp Hematol. 2003;7 (3):233–45 [PubMed] [Google Scholar]
- 8.Mullighan CG, Goorha S, Radtke I, Miller CB, Coustan-Smith E, Dalton JD, et al. Genome-wide analysis of genetic alterations in acute lymphoblastic leukaemia. Nature. 2007;446(7137):758–64 [DOI] [PubMed] [Google Scholar]
- 9.Bardini M, Galbiati M, Lettieri A, Bungaro S, Gorletta TA, Biondi A, et al. Implementation of array based whole-genome high-resolution technologies confirms the absence of secondary copy-number alterations in MLL-AF4-positive infant ALL patients. Leukemia. 2011;25(1):175–8 [DOI] [PubMed] [Google Scholar]
- 10.Marschalek R. Mechanisms of leukemogenesis by MLL fusion proteins. Br J Haematol. 2011;152(2):141–54 [DOI] [PubMed] [Google Scholar]
- 11.Moorman AV, Ensor HM, Richards SM, Chilton L, Schwab C, Kinsey SE, et al. Prognostic effect of chromosomal abnormalities in childhood B-cell precursor acute lymphoblastic leukaemia: results from the UK Medical Research Council ALL97/99 randomised trial. Lancet Oncol. 2010;11(5): 429–38 [DOI] [PubMed] [Google Scholar]
- 12.Moorman AV, Ensor HM, Richards SM, Chilton L, Schwab C, Kinsey SE, et al. Key pathways are frequently mutated in high risk childhood acute lymphoblastic leukemia: a report from the Children’s Oncology Group. Blood. 2011;118(11): 3080–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mahgoub N, Parker RI, Hosler MR, Close P, Winick NJ, Masterson M, et al. RAS mutations in pediatric leukemias with MLL gene rearrangements. Genes Chromosomes Cancer. 1998;21(3):270–5 [PubMed] [Google Scholar]
- 14.Stam RW, den Boer ML, Schneider P, Meier M, Beverloo HB, Pieters R. D-HPLC analysis of the entire FLT-3 gene in MLL rearranged and hyperdiploid acute lymphoblastic leukemia. Haematologica. 2007;92(11): 1565–8 [DOI] [PubMed] [Google Scholar]
- 15.Stumpel DJ, Schneider P, van Roon EH, Boer JM, de Lorenzo P, Valsecchi MG, et al. Specific promoter methylation identifies different subgroups of MLL rearranged infant acute lymphoblastic leukemia, influences clinical outcome and provides therapeutic options. Blood. 2009;114(27):5490–8 [DOI] [PubMed] [Google Scholar]
- 16.Geng H, Brennan S, Milne TA, Chen WY, Li Y, Hurtz C, et al. Integrative epigenomic analysis of adult B-acute lymphoblastic leukemia identifies biomarkers and therapeutic targets. Cancer Discov. 2012;2(11): 1004–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.van Dongen JJ, Macintyre EA, Gabert JA, Delabesse E, Rossi V, Saglio G, et al. Standardised RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Leukemia. 1999;13 (12):1901–28 [DOI] [PubMed] [Google Scholar]
- 18.Mantel N, Byar DP. Evaluation of response-time data involving transient states: an illustration using heart-transplant data. J Am Stat Assoc. 1974;69:81–6 [Google Scholar]
- 19.Paietta E. Immunobiology of acute leukemia. In: Wiernik P, Dutcher J, Goldman J, Kyle R, eds. Neoplastic Diseases of the Blood, 4th Edition Cambridge, UK: Cambridge University Press; 2003:194–231 [Google Scholar]
- 20.Marks DI, Wang T, Pérez WS, Antin JH, Copelan E, Gale RP, et al. The outcome of full-intensity and reduced-intensity conditioning matched sibling or unrelated donor transplantation in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia in first and second complete remission. Blood. 2010;116(3):366–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mohty M, Labopin M, Volin L, Gratwohl A, Socié G, Esteve J. Acute Leukemia Working Party of EBMT. Reduced-intensity versus conventional myeloablative conditioning allogeneic stem cell transplantation for patients with acute lymphoblastic leukemia: a retrospective study from the European Group for Blood and Marrow Transplantation. Blood. 2010;116(22): 4439–43 [DOI] [PubMed] [Google Scholar]
- 22.Fielding AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukaemia (ALL); an MRC UKALL XII/ECOG 2993 study. Blood. 2007;109(3):944–50 [DOI] [PubMed] [Google Scholar]
- 23.Topp MS, Kufer P, Gökbuget N, Goebeler M, Klinger M, Neumann S, et al. Targeted therapy with the T-cell-engaging antibody blinatumomab of chemotherapy-refractory minimal residual disease in B-lineage acute lymphoblastic leukemia patients results in high response rate and prolonged leukemia-free survival. J Clin Oncol. 2011(18);29:2493–8 [DOI] [PubMed] [Google Scholar]
- 24.Kantarjian H, Thomas D, Jorgensen J, Jabbour E, Kebriaei P, Rytting M, et al. Inotuzumab ozogamicin, an anti-CD22-calecheamicin conjugate, for refractory and relapsed acute lymphocytic leukaemia: a phase 2 study. Lancet Oncol. 2012;13(4): 403–11 [DOI] [PubMed] [Google Scholar]
- 25.Sverdlow SH, Camp E, Harris NL, et al. Eds. WHO classification of tumour of haematopoietic and lymphoid tissues. International Agency for Research on Cancer, Lyon, 2008 [Google Scholar]
- 26.Rai L, Casanova A, Moorman AV, Richards S, Buck G, Goldstone AH, et al. Antigen receptor gene rearrangements reflect on the heterogeneity of adult Acute Lymphoblastic Leukaemia (ALL) with implications of cellorigin of ALL subgroups – a UKALLXII study. Br J Haematol. 2010;148(3):394–401 [DOI] [PubMed] [Google Scholar]
- 27.Litzow MR, Buck GAN, Paietta E, et al. Outcome of 1229 adult Philadelphia chromosome negative B-lineage acute lymphoblastic leukemia patients on the international UK ALL XII-ECOG2993 trial. (manuscript in preparation) [Google Scholar]
- 28.Schwab CJ, Jones LR, Morrison H, Ryan SL, Yigittop H, Schouten JP, et al. Evaluation of multiplex ligation-dependent probe amplification as a method for the detection of copy number abnormalities in B-cell precursor acute lymphoblastic leukemia. Genes Chromosomes Cancer. 2010;49(12):1104–13 [DOI] [PubMed] [Google Scholar]
- 29.De Zen L, Bicciato S, te Kronnie G, Basso G. Computational analysis of flow-cytometry antigen expression profiles in childhood acute lymphoblastic leukemia: an MLL/AF4 identification. Leukemia. 2003;17(8):1557–65 [DOI] [PubMed] [Google Scholar]
- 30.Cox CV, Diamanti P, Evely RS, Kearns PR, Blair A. Expression of CD133 on leukemia initiating cells in childhood ALL. Blood. 2009;113(14):3287–96 [DOI] [PubMed] [Google Scholar]
- 31.Armstrong SA, Staunton JE, Silverman LB, Pieters R, den Boer ML, Minden MD, et al. MLL translocations specify a distinct gene expression profile that distinguishes a unique leukemia. Nat Genet. 2002;30(1):41–7 [DOI] [PubMed] [Google Scholar]
- 32.Moorman AV, Schwab C, Ensor HM, Russell LJ, Morrison H, Jones L, et al. IGH@ translocations, CRLF2 deregulation, and microdeletions in adolescents and adults with acute lymphoblastic leukemia. J Clin Oncol. 2012; 30(25):3100–8 [DOI] [PubMed] [Google Scholar]
- 33.Bernt KM, Armstrong SA. Targeting epigenetic programs in MLL-rearranged leukemias. Hematology Am Soc Hematol Educ Program. 2011;2011:354–60 [DOI] [PubMed] [Google Scholar]
- 34.Daigle SR, Olhava EJ, Therkelsen CA, Majer CR, Sneeringer CJ, Song J, et al. Selective killing of mixed lineage leukemia cells by a potent small-molecule DOT1L inhibitor. Cancer Cell. 2011;20(1):53–65 [DOI] [PMC free article] [PubMed] [Google Scholar]