

Abstract
Background:
Low back pain is a very common phenomenon in computer users. More than 80% people using computers for more than 4 h complain of back pain.
Objective:
To compare the effectiveness of multidisciplinary treatment approach and conventional treatment approach amongst computer users.
Materials and Methods:
A prospective interventional study was carried out at a private spine clinic amongst the computer users with the complaint of low back pain. The study participants were randomly distributed in two groups. The first group comprised the study participants treated by conventional approach and the second group was treated by multidisciplinary approach. Primary outcomes analyzed were pain intensity, sick leave availed, and quality of life. Statistical analysis was done using proportions, unpaired “t” test, and Wilcoxon signed-rank test.
Results:
Totally 44 study participants were randomly assigned to groups I and II, and each group had 22 study participants. Intensity of pain was reduced significantly in the group treated by multidisciplinary approach (t = 5.718; P = 0.0001). Similarly only 4 (19.19%) of the study participants of the group treated by multidisciplinary approach availed sick leave due to low back pain, while 14 (63.63%) study participants availed sick leave in the other group (P = 0.02). The quality of life amongst the study participants treated by multidisciplinary approach was significantly improved compared to the group treated by conventional approach (t = 7.037; P = 0.0001).
Conclusion and Recommendation:
The multidisciplinary treatment approach was better than the conventional treatment approach in low back pain cases when some factors like pain and quality of life were assessed. The multidisciplinary approach for treatment of low back pain should be promoted over conventional approach. Larger studies are required to confirm the findings in different settings.
Keywords: Computer users, low back pain, multidisciplinary approach
INTRODUCTION
Low back pain is a very common condition, with about 90% of people suffering from it at some point in their lives.[1] In many countries, chronic low back pain is the most common cause of long-term disability in middle age.[2] Low back pain is a major health problem, not only because of the high prevalence and incidence of low back problems but also because of the important consequences which are disability, the use of health services, sickness absence, and early retirement.[3] Back pain also accounts for many lost working days.[4,5]
Computer work has generated a new genre of occupational health problems, i.e., of computer-related problems. Postural back pain is a major public and occupational health problem, especially in the information technology (IT) and BPO sectors.[6] In India, the occupational health personnel is slowly awakening to this group of modern occupational diseases, which are slowly taking their roots among the IT professionals. These problems, if ignored, can prove debilitating and cause crippling injuries, forcing one to change their profession.[7]
According to Borenstein, low back pain should be viewed as a medical disorder, with the goal being to return to regular physical activity as quickly as possible and to enable the patient to receive the most beneficial care at optimal times.[8]
There is no established protocol or model which a back pain sufferer goes through after having a first episode of back pain. Acute back pain seems to respond well to simple treatment measures,[9,10] although there is a lot of variation in the benefit for individual patients.
Clinical trials have shown that psychosocial factors have an important influence on the prognosis of low back pain. They display more predictive power in the course of the sickness than biomedical variables.[11,12] Studies conducted have shown moderate evidence that multidisciplinary (biopsychosocial) treatments are superior to biomedical treatment in the improvement of pain, functional status, and time to return to work, and the long-term effects of psychologic interventions have been discussed controversially.[13–17]
This study was conducted with an objective of comparing the effectiveness of multidisciplinary treatment approach with conventional treatment approach amongst computer users.
MATERIALS AND METHODS
A prospective interventional study was conducted at a private setup. The criteria for selection of the study participants were formulated. The criteria were as follows.
Inclusion criteria
Postural low back pain
Computer work > 8 h/day for 5 days
Exclusion criteria
History or presence of radicular pain
Specific physical condition such as nucleus pulposus prolapse, tumor, spondylolisthesis, spinal stenosis, or cauda equine syndrome
Red flags according to the current guidelines of back pain, including history and presence of inflammation, tumor, trauma, and neurological deficits ruled out by clinical, radiological, or laboratory examination
Systemic diseases like rheumatoid arthritis, Crohn's disease, diabetes mellitus, cancer, or psychiatric disease
Clinical interventions
The interventions were based on outpatient rehabilitation programs in both groups with respect to dosage and contents. A total of 44 patients participated in the study. They were randomly distributed in two groups equally, i.e., 22 in each.
Group I included study participants to be treated by conventional treatment approach. The conventional treatment approach comprised orthopedics consultation and physical therapy.
Group II included study participants to be treated by multidisciplinary treatment approach which included combination of orthopedic consultation, physiotherapy, ergonomics, vitamin supplementation, diet plan, massage therapy, and stress management.
Study participants and assessors were blinded about the groups and therapy. The study was done over a period of 4 weeks.
Each patient received approximately 2 h of daily treatment for 15 days in 3 weeks.
The follow-up of all study participants was done after 1 year.
Primary outcomes
Intensity of pain was assessed by Pain Questionnaire (McGill Pain Questionnaire).[18] It is based on the view of pain perception as affective and cognitive-evaluative.
Leave register from office – It details the number of days of leave 3 months before and 3 months after the treatment. The leave taken for reasons other than back pain was excluded.
Quality of life measured by SF-36.[19] The 12 items provide a representative 3) sampling of the content of the eight health concepts and operational definitions of those concepts, including what respondents are able to do, how they feel, and how they evaluate their health status.
Statistical analysis
The statistical analysis was done by using statistical software programs Primer of Biostatistics[20] and Epi Info.[21] Appropriate statistical tests like proportions, unpaired “t” test, and Wilcoxon signed-rank test were applied.
Ethical aspects
The study was conducted according to the guidelines of the Helsinki Declaration and of Good Clinical Research Practice. The research study was approved by an independent ethical committee. All the study participants were told about the nature and outcome of study and written informed consent was taken.
RESULTS
The total number of study participants was 44. Each group had 22 participants.
Intensity of pain assessed by Pain Questionnaire, as mentioned in the section Materials and Methods, is given in Table 1 and Figure 1. The multidisciplinary treatment approach is found to be better than traditional treatment approach.
Table 1.
Comparison of pain intensity on visual analog score
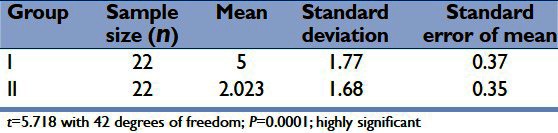
Figure 1.
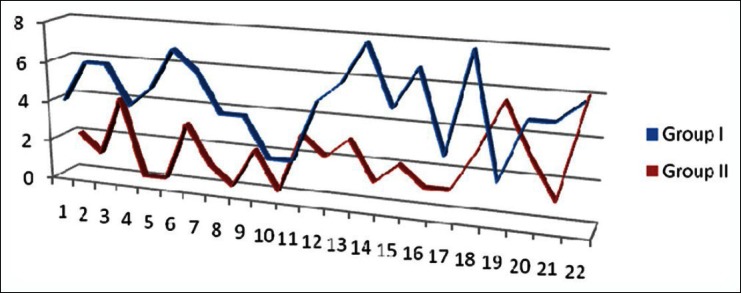
Pain intensity on visual analogue scores
The number of days of sick leave availed due to low back pain during the year was also assessed. In the group treated with traditional approach, 14 (63.63%) participants availed leave due to low back pain, while in the group treated with multidisciplinary approach, only 4 (18.18%) participants availed leave for the same reason.
For the number of days of leave taken, the statistical analysis was done by using Wilcoxon signed-ranked test (w = 96, P = 0.02; significant).
The number of days of leave taken in those treated by multidisciplinary approach was significantly less than that taken by those who were treated by traditional approach.
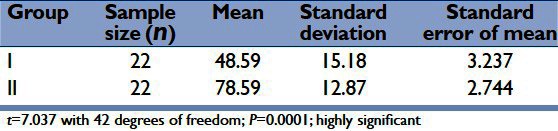
The analysis of the “SF-36 Health Survey” is designed to examine a person's perceived health status. As per Table 2, the SF-36 Health Survey scores were significantly higher in the group treated by multidisciplinary approach than the group treated by traditional approach. This shows that perceived health status was better in the group which was treated by multidisciplinary approach.
Table 2.
Comparison of perceived health status on SF-36® health survey
DISCUSSION
Postural low back pain is a major public and occupational health problem, especially in the IT and BPO sectors. Eight out of ten people working more than 8 h in front of computers have back pain. Although medical costs for back pain are high, hidden costs like absenteeism and reduced productivity are significant. Early identification of clinical, psychosocial, and professional risk factors is important to prevent the progression to chronic low back pain.[22]
There is no established protocol or model which a back pain sufferer goes through after having a first episode of back pain. A general physician or an allied health professional is the first point of contact in such cases. After the initial screening, painkillers are often prescribed and only a few times specialist consultation is sought. Conventional treatment which usually includes orthopedic consultation and physical therapy is the preferred choice of treatment when pain and discomfort during work increases at a secondary or tertiary care unit. Many different rehabilitation programs of unclear efficacy are currently in use.[23] Multidisciplinary treatment approaches including biopsychosocial rehabilitation are scarcely practiced treatment methods in India. There is strong evidence that intensive multidisciplinary biopsychosocial rehabilitation with functional restoration improves function in chronic and nonspecific back pain. The flaw in most rehabilitation approaches is that they are unidirectional and involve only the physical aspect of rehabilitation.
In our study, we compared the multidisciplinary treatment approach with the conventional treatment approach for the low back pain. We found that multidisciplinary treatment approach was better than conventional treatment approach when certain outcomes like intensity of pain, number of sick leave availed due to low back pain, and perceived health status were considered.
The randomized trial conducted by Moffett et al. revealed the superiority of combined exercise and behavioral treatment in primary care management, and they concluded that rather than the intensity of pain, the ability to cope was improved.[24] Nicholas et al. reported superior improvement in patients with chronic low back pain after a combined psychological and physiotherapeutic treatment over those treated by exercise and discussion sessions.[25] Turner et al. in a randomized trial compared behavioral treatment, exercise, and a combination of both in an outpatient and a group setting for back patients mostly not in sick leave; whilst short-term effects were superior after the combination therapy, all significant differences disappeared after 6 months due to small sample sizes.[16,26] A systematic review concluded that a high dose, biopsychosocial therapy improves function and pain considerably compared to biomedical therapy; in terms of sick leave, their conclusions were contradictory.[27]
To conclude, this study supports the evidence that the multidisciplinary treatment approach in low back pain is a better option over the conventional treatment approach. Larger studies, especially randomized controlled trials, are recommended to confirm the evidence in Indian scenario.
Limitation of the study
The study was conducted with a comparatively smaller sample size.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Frymoyer JD. Back pain and sciatica. N Engl J Med. 1988;318:291–300. doi: 10.1056/NEJM198802043180506. [DOI] [PubMed] [Google Scholar]
- 2.Badley EM, Rasooly I, Webster GK. Relative importance of musculo- skeletal disorders as a cause of chronic health problems, disability, and health care utilization: Findings from the 1990 Ontario health survey. J Rheumatol. 1994;21:505. [PubMed] [Google Scholar]
- 3.Nyman T, Grooten WJ, Wiktorin C, Liwing J, Norman L. Sickness absence and concurrent low back and neck-shoulder pain: Results from the MUSIC-Norrtalje study. Eur Spine J. 2007;16:631–3. doi: 10.1007/s00586-006-0152-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hoogendoorn WE, Bongers PM, de Vet HC, Ariens GA, van Mechelen W, Boutler LM. High physical work load and low job satisfaction increase the risk of sickness absence due to low back pain. Occup Environ Med. 2002;59:323–8. doi: 10.1136/oem.59.5.323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reme SE, Hagen EM, Eriksen HR. Expectations, perceptions, and physiotherapy predict prolonged sick leave in subacute low back pain. BMC Musculoskelet Disord. 2009;10:139. doi: 10.1186/1471-2474-10-139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bhuyar P, Banerjee A, Pandve H, Padmanabhan P, Patil A, Duggirala S, et al. Mental, physical and social health problems of call centre workers. Indian Psychiatry J. 2008;17:21–5. [Google Scholar]
- 7.Choudhary SB, Sapur S, Deb PS. Awkward posture and development of RSI (Repetitive strain injury) in computer professionals. Indian J Occup Environ Med. 2002;6:10–2. [Google Scholar]
- 8.Borenstein DG. Clinician's approach to acute low back pain. Am J Med. 1997;102:16S–22. doi: 10.1016/s0002-9343(97)00412-9. [DOI] [PubMed] [Google Scholar]
- 9.Bendix AF, Bendix T, Labriola M. Functional restoration for chronic low back pain: Two-year follow-up of two randomized trials. Spine. 1998;23:717–5. doi: 10.1097/00007632-199803150-00013. [DOI] [PubMed] [Google Scholar]
- 10.Patijn J, Durinck JR. Effects of manual medicine on absenteeism. J Man Med. 1991;6:49–53. [Google Scholar]
- 11.Thomas E, Silman AJ, Croft PR, Papageorgiou AC, Jayson MI, Macfarlane GJ. Predicting who develops chronic low back pain in primary care. A prospective study. Brit Med J. 1999;318:1662–7. doi: 10.1136/bmj.318.7199.1662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Waddell G, McCulloch JA, Kummel E, Venner RM. Nonorganic physical signs in low-back pain. Spine. 1980;5:117–25. doi: 10.1097/00007632-198003000-00005. [DOI] [PubMed] [Google Scholar]
- 13.Haldorsen EM, Grasdal AL, Skouen JS, Risa AE, Kronholm K, Ursin H. Is there a right treatment for a particular patient group? Comparison of ordinary treatment, light multidisciplinary treatment, and extensive multidisciplinary treatment for long-term sick-listed employees with musculoskeletal pain. Pain. 2002;95:49–63. doi: 10.1016/s0304-3959(01)00374-8. [DOI] [PubMed] [Google Scholar]
- 14.Jousset N, Fanello S, Bontoux L, Dubus V, Billabert C, Vielle B, et al. Effects of functional restoration versus 3 hours per week physical therapy: A randomized controlled study. Spine. 2004;29:487–93. doi: 10.1097/01.brs.0000102320.35490.43. [DOI] [PubMed] [Google Scholar]
- 15.Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, Koes B. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults. Spine. 2001;26:262–9. doi: 10.1097/00007632-200102010-00011. [DOI] [PubMed] [Google Scholar]
- 16.Turner JA, Jensen MP. Efficacy of cognitive therapy for chronic low back pain. Pain. 1993;52:169–77. doi: 10.1016/0304-3959(93)90128-C. [DOI] [PubMed] [Google Scholar]
- 17.Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work: Evidence review. Occup Med. 2001;51:124–35. doi: 10.1093/occmed/51.2.124. [DOI] [PubMed] [Google Scholar]
- 18.Melzack R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain. 1975;1:277–99. doi: 10.1016/0304-3959(75)90044-5. [DOI] [PubMed] [Google Scholar]
- 19.Quality of Life measured by SF-36. [Last accessed on 2012 Oct 13]. As Available from: http://www.sf-36.org/announcements/Updated_SF36_bookChapter_Sept04.pdf .
- 20.Stanton Glantz SA. 6th Ed. New York: McGraw-Hill; 2005. Primer of Biostatistics. [Google Scholar]
- 21.USA: CDC Atlanta; 2002. Epi Info 2002, Software package. [Google Scholar]
- 22.Blanco TR, Fernandez I, Corbella MB, Berenguera A, Moix J, Morillo EM, et al. Study protocol of effectiveness of a biopsychosocial multidisciplinary intervention in the evolution of non-speficic sub-acute low back pain in the working population: Cluster randomised trial. BMC Health Serv Res. 2010;10:12. doi: 10.1186/1472-6963-10-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: Synthesis of best evidence for clinical decisions. Ann Intern Med. 1997;126:376–80. doi: 10.7326/0003-4819-126-5-199703010-00006. [DOI] [PubMed] [Google Scholar]
- 24.Moffett JK, Torgerson D, Bell-Syer S, Jackson D, Llewlyn-Phillips H, Farrin A, et al. Randomised controlled trial of 24. exercise for low back pain: Clinical outcomes, costs, and preferences. BMJ. 1999;319:279–83. doi: 10.1136/bmj.319.7205.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nickolas MK, Wilson PH, Goyen J. Comparison of cognitive behavioral group treatment and an alternative nonpsychological treatment for chronic low back pain. Pain. 1992;48:339–47. doi: 10.1016/0304-3959(92)90082-M. [DOI] [PubMed] [Google Scholar]
- 26.Turner JA, Clancy SC, Mc Quade KJ, Cardanes DD. Effectiveness of behavioral therapy for chronic low back pain: A component analysis. J Consult Clin Psychol. 1990;58:573–9. doi: 10.1037//0022-006x.58.5.573. [DOI] [PubMed] [Google Scholar]
- 27.Guzman J, Esmail R, Karjalainen K, Malmivaara A, Emma I, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. B Med J. 2001;322:1511–6. doi: 10.1136/bmj.322.7301.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]