

Abstract
Background:
Tuberculosis (TB) remains as an important public health problem in India. Awareness about the disease, its diagnosis, and treatment among public will help in controlling the killer disease. This study aims at arriving at an educational diagnosis about TB in an urban poor community.
Materials and Methods:
A cross-sectional study was conducted in an urban slum in South India using a structured, pretested questionnaire. Domains identified were knowledge about TB, symptoms, spread, diagnosis, treatment, and prevention of TB.
Results:
A total of 395 households were interviewed. Of them, 370 (94%) respondents had heard about TB. Regarding the symptoms of TB, 82% were aware that cough is a symptom of TB. Among the 79% of study subjects who reported any test to diagnose TB, sputum examination as a method of diagnosis was known to only 40%. However, 84% of the subjects were aware of the free treatment available for TB under National program.
Conclusion:
Level of awareness about TB among urban poor in a slum area is good. Knowledge about “free treatment” and “duration of treatment” has to be stressed during health education activities.
Keywords: Awareness, tuberculosis, urban slum
INTRODUCTION
Periodic knowledge, attitude, and practice (KAP) studies serve as an educational diagnosis of a population or community and are an important way to measure changing beliefs and behaviors over time. It tells us what people know about certain things, how they feel, and how they behave. This information helps programs set communication objectives linked to increased community engagement and demand for services and develop tailored strategies appropriate for the social, cultural, and political contexts of at-risk communities.
India has the highest burden of tuberculosis (TB) in the world, accounting for approximately one-fifth of the global incidence - an estimated two million cases annually.[1] India alone accounts for more than 25% of the world′s incident cases.[2] Under Revised National Tuberculosis Control Programme, through a consistent communication, a lot of awareness has been created about TB - about its cause, symptoms, and cure, as well as various misconceptions and stigmas attached to it. Studies on awareness of TB and treatment seeking behavior have been carried out in various parts of India on various subgroups.[3–5] Awareness among general population, especially vulnerable population like urban slums, regarding TB is important and it leads to timely treatment seeking. Knowledge about the common symptoms of TB and availability of free diagnosis and treatment facility for TB will help in improving the treatment seeking behavior. This study was carried out to assess awareness regarding symptoms, causes, spread, and treatment of TB in an urban slum area of Puducherry.
MATERIALS AND METHODS
Study design
A community-based cross sectional study was designed.
Study setting
The study was conducted in an urban slum of Puducherry district of Union Territory of Puducherry. The study area, “Vaithikuppam” is an urban slum and part of urban field practice area of the Department of Community Medicine of a teaching institute. It is a coastal slum about 2 km from the main town Puducherry. The majority of adult men in the study area were fishermen. An urban health center run by a premier teaching institute (JIPMER) at about 1 km is the nearest health facility for this area. District hospital of Puducherry, a tertiary care center, is about 3 km away from this coastal slum. Revised National Tuberculosis Control Program (RNTCP) was implemented in this area since 1997. The study area is a part of Muthialpet Primary Health Centre, which is a designated microscopy center (DMC) for the diagnosis of TB under RNTCP. Under RNTCP, sputum examination is the mainstay of diagnosis of TB and anti-TB drugs are provided free of cost for entire duration of treatment which is usually 6–8 months.
Study instrument
A pretested, structured interview schedule was used to assess the KAP related to symptoms, causes, spread, and treatment of TB. Domains identified were knowledge about TB, symptoms, spread, diagnosis, treatment, and prevention of TB.
Study population and selection of households
House to house visit was done in the study area, and there were about 450 households in the slum part of study area. Thirty-five houses were locked during visit and 415 households were approached for an interview. An adult member in the house present at the time of visit and who was willing to participate in the study were interviewed.
Data entry and analysis
Data were entered into a Microsoft Excel spreadsheet and analyzed with Microsoft excel and SPSS version 13.0. Descriptive statistics were calculated.
OBSERVATIONS AND RESULTS
A total of 415 households were approached for an interview. Twenty households (4.8%) refused to participate citing household work at the time of visit. A total of 395 people were interviewed, of whom 285 (72%) were females and 110 (28%) were males [Table 1]. Of them, 72% of females were housewives and 23% of males were engaged in fishing and related work. About one-fifth of the study subjects were living in kutcha houses, and more than half of them were living in overcrowded houses. Median family income per month was 5000 rupees, and about one-fourth of the study subjects had their monthly income less than 3000 rupees. Mean per capita income was 2186 rupees.
Table 1.
Sociodemographic characteristics of study population

Awareness about TB and its symptoms
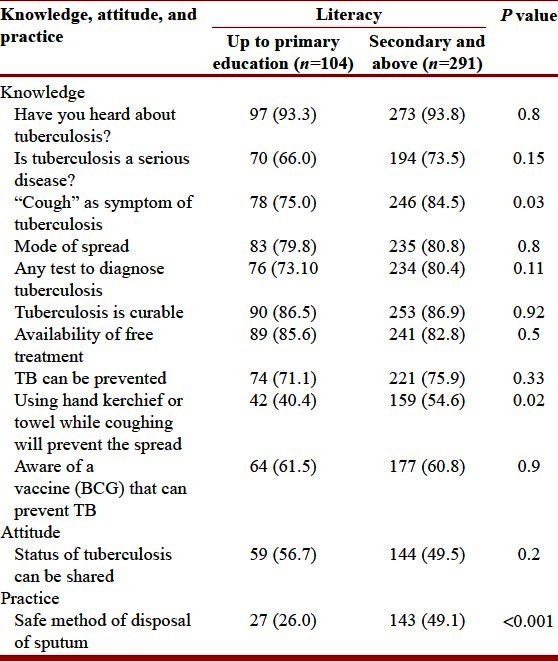
A total of 370 (94%) respondents had heard about TB. Out of them, 71% (264) considered TB as a serious disease. Regarding the symptoms of TB, 82% were aware that cough is a symptom of TB, followed by weight loss (28%), blood in sputum (18%), and fever (14%). Also, 4% reported that vomiting as a symptom of TB and diarrhea by 2% of respondents. However, 10% of respondents were not aware of any symptom. There is no difference in the knowledge about “cough” as a symptom of TB between males and females (P = 0.95) [Table 2]. Although majority of participants were aware of “cough” as a symptom, participants who were educated secondary school and above had better knowledge (P = 0.03) [Table 3]. Of the respondents, 75% were aware that TB can affect children and 14% denied it.
Table 2.
Knowledge, attitude, and practice regarding tuberculosis by gender in the study population
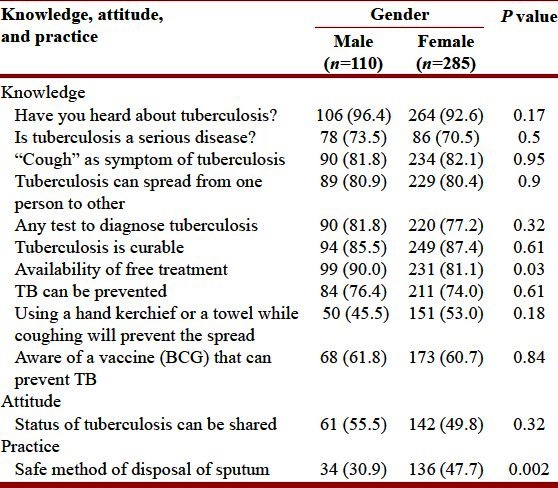
Table 3.
Knowledge, attitude, and practice regarding tuberculosis by literacy in the study
Awareness about modes of spread and diagnosis
When asked about the spread of TB, 81% stated that TB can spread from one person to another and 11% were of opinion that TB will not spread. Regarding the modes of spread, 65% knew that TB spreads through cough and 18% stated that talking with a TB patient can spread TB. Also, 13% reported that TB can spread by touching and 5% perceived contaminated water as a mode of spread of TB. Only 1% of respondents were aware that overcrowding can spread TB. Out of 395 study subjects, 79% stated that there were tests to diagnose TB. Among the 79% of study subjects who reported any test, sputum examination as a method of diagnosis was known to only 40% and X-ray was stated by 8%. Among the respondents, 32% of subjects reported blood tests as a method of diagnosis and 9% were not aware of any diagnostic method. Only 51% of participants reported that they would share the status of TB of family members with their relatives or neighbors.
Awareness about treatment
When asked whether TB is curable, 87% said that TB is curable. Regarding duration of treatment, 42% were aware of the treatment duration of 6 months and/or above. Of them, 20% reported that treatment should be taken as long as symptoms disappear, and 26% did not know the duration of treatment. Moreover, 18% of subjects were of the opinion that visiting religious places will cure TB. Among the respondents, 84% were aware of the free treatment available for TB and 11% were not aware of the free treatment and 5% denied the availability of free treatment. Men were more aware about free treatment for TB compared to women, and this difference is statistically significant (P = 0.03) [Table 2].
Awareness and practices regarding cough and disposal of sputum
Of the respondents, 75% said that TB can be prevented from spreading to other family members by some precaution and 45% said that isolation of TB patients from other family members will prevent spread. In addition, 51% were aware that using a hand kerchief or a towel while coughing will prevent the spread, and 18% were aware of chemoprophylaxis to children as a measure to prevent spread of TB to children. When asked about their usual method of disposal of sputum, 43% of study subjects stated that they disposed it in a dustbin/sewage. Knowledge of women was better compared to men regarding safe disposal of sputum (P = 0.002) [Table 2]. Knowledge regarding using a hand kerchief or a towel during cough and safe disposal of sputum were more in participants, who had education secondary school and above [Table 3]. Of the respondents, 43% reported the disposal of sputum in front or back of the house in open space and 61% were aware of a vaccine (BCG) that can prevent TB and it is given for children. Of the participants, 26% were not aware of the vaccine and even 13% denied the presence of vaccine against TB.
DISCUSSION
In our study awareness about TB is good except for some components of diagnosis and treatment of TB. A high level of literacy in this slum area and geographical proximity to the government hospital might be reasons for the good level of awareness. Mean per capita income of study population was 2186, and it is much lower compared to mean per capita income of UT of Puducherry (7980 rupees) and All India (5081 rupees).[6] This may be the scenario in an urban slum, but underreporting of income cannot be ruled out. Of the respondents, 71% considered TB as a serious disease, an important determinant of health care seeking. Regarding modes of spread, 65% were aware of cough as a mode of spread compared to a 20% in a study done in rural Tamil Nadu.[7] Only 40% were aware about sputum examination as a method of diagnosis and efforts have to be made to create more awareness sputum examination who have cough more than two weeks. Of them, 32% told that blood tests can be a diagnostic method which may be because of their experiences with the private practitioners, where blood investigations are commonly advised for the diagnosis of TB.
About 16% were not aware of the free treatment for TB. Residents of slums are more vulnerable because of overcrowding and poverty and should be more aware of the free treatment. Treatment for TB is generally costlier in private settings pushing the family into poverty trap, and it may lead to treatment default after few weeks of treatment.[8] In some of the studies, literacy has been identified as a key factor deciding the level of awareness.[9,10] In addition to the literacy level, health care providers should reinforce the information related to TB in the community. Village health and nutrition days can be utilized for this purpose. “Free diagnosis and free treatment” of TB should be known to all, and it will help in improving the health seeking behavior and adherence to treatment of TB. Social issues such as stigma associated with TB and isolating the TB patients have to be dealt during health education sessions.
Regarding practices related to prevention of spread of TB, though 65% were aware of spread by cough, 43% are disposing their sputum in front or back of the house. There exists a knowledge-practice gap, which should be focused during health education sessions. Carrying out representative periodic KAP surveys, focus groups, community dialogues, and in-depth discussions will identify the deficiencies in knowledge and practices of the community thereby providing clues to improve the performance of RNTCP, especially the case detection rate and adherence to treatment. World Health Organization recommends KAP surveys related to TB-related knowledge, attitude, and practice, which will help in advocacy, communication, and social mobilization strategy planning.[11]
CONCLUSION
Level of awareness about TB among urban poor in a slum area is good. Knowledge about “free treatment” and “duration of treatment” has to be stressed during health education activities.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Central TB Division, Directorate General of Health Services. New Delhi: Ministry of Health and Family Welfare Nirman Bhawan; 2011. TB India. RNTCP Annual Report; p. 1. [Google Scholar]
- 2.WHO Report 2011. Geneva: World Health Organization; 2011. Global tuberculosis control. [Google Scholar]
- 3.Malhotra R, Taneja DK, Dhingra VK, Rajpal S, Mehra M. Awareness regarding tuberculosis in a rural population of Delhi. Indian J Community Med. 2002;27:62–8. [Google Scholar]
- 4.Fochsen G, Deshpande K, Diwan V, Mishra A, Diwan VK, Thorson A. Health care seeking among individuals with cough and tuberculosis: A population-based study from rural India. Int J Tuberc Lung Dis. 2006;10:995–1000. [PubMed] [Google Scholar]
- 5.Sharma N, Malhotra R, Taneja DK, Saha R, Ingle GK. Awareness and perception about tuberculosis in the general population of Delhi. Asia Pac J Public Health. 2007;19:10–5. doi: 10.1177/10105395070190020301. [DOI] [PubMed] [Google Scholar]
- 6.Per capita net state domestic product at current prices, 2011-12. Central statistical office. Ministry of statistics and programme implementation. Government of India. [Last accessed on 2012 Jun 09]. Available from: URL: http://mospi.nic.in/Mospi_New/upload/State_wise_SDP_2004.05_14mar12.pdf .
- 7.Kar M, Logaraj M. Awareness, attitude and treatment seeking behavior regarding tuberculosis in a rural area of Tamil Nadu. Indian J Tuberc. 2011;57:226–9. [PubMed] [Google Scholar]
- 8.Social assessment study for RNTCP-final report, Submitted to: Central TB Division, Ministry of Health and Family Welfare (Government of India), New Delhi. ORG Centre for Social Research. 2003. [Last accessed on 2012 Feb 20]. Available from: http://www.tbcindia.nic.in/pdfs/Social%20Assessment%20Study%20for%20RNTCP%20.%20Final%20Report%20.%20ORG%20CSR.pdf .
- 9.Yadav SP, Mathur ML, Dixit AK. Knowledge and attitude towards tuberculosis among sandstone quarry workers in desert parts of Rajasthan. Indian J Tuberc. 2006;53:187–95. [Google Scholar]
- 10.Devey J. Report on a knowledge, attitude, and practice (KAP) survey regarding tuberculosis conducted in northern Bihar. 23 April 2001. Report on an independent study conducted during a HNGR internship with: Champak and Chetna community health and development projects, Duncan hospital, Bihar, India. [Last accessed on 2012 Feb 20]. Available from: http://www.eha.health.org/index.php/resources/doc_view/11.tb.study.html .
- 11.Advocacy, communication and social mobilization for TB control: A guide to developing knowledge, attitude and practice surveys. Geneva: World Health Organization; 2008. [Google Scholar]