

Abstract
Adrenal myelolipoma is a rare benign tumour. This tumour is generally considered as a type of hormonally inactive neoplasm, which is composed of mature adipose tissue and normal haematopoietic cells. Rarely adrenal myelolipoma and adrenal cortical adenoma could be found together in the same gland. Due to myelolipoma's asymptomatic character, it is generally diagnosed incidentally. In fact, myelolipoma can now be easily detected because of improved techniques such as ultrasound, CT and MRI and widespread use of imaging. Because of this a 66-year-old male patient with abdominal pain, proved that adrenal myelolipoma and non-functional adrenal cortical adenoma are rare in the same gland. The case presented here deals with different outcome which is rare in the literature.
Background
Adrenal myelolipoma is a rare benign neoplasm, which is composed of mature adipose tissue and normal haematopoietic cells. In the literature, myelolipoma was described first by the German scientist E Uber Gierke in 1905 but C Oberling was first to use myelolipoma as a term in 1929.1–4 In fact, it does not represent a haematopoietic source, myelolipoma contains precursors of white and red blood cells such as megakaryocytes. Generally, small and asymptomatic lesions are discovered incidentally. Symptomatic ones are frequently found in haemorrhage. In these kind of cases, as it is valid for our case, they require surgical exploration. In this case, adrenal cortical adenoma was well encapsulated from connective tissue. Consisting of clear cells and eosinophilic cells, adenoma is arranged with alveolar structure. Interstitial tissue is sparse but well vascularised by sinusoids. Relying on blood and urine tests, adenoma's non-functional structure was certainly proved.3
Case presentation
A 66-year-old male presented to the clinic with abdominal pain. Ultrasonographic examination of the patient's abdomen, revealed a heterogeneous hypodense solid mass measuring 60×35 mm, at the level of the upper pole of the right kidney. CT scan also showed the presence of well-demarcated right retroperitoneal mass, measuring 60×35 mm. According to the patient's history, 10 years ago, the paitent had undergone left nephrectomy. He also underwent goitre surgery. Serum cortisol, urinary metanefrin and normetanefrin were within normal limits. Suppression of dexamethasone test proves that adrenal cortical adenoma was non-functional. Under these conditions, laparoscopic right adrenalectomy was performed on the patient. Postoperatively, the patient's recovery was uneventful. Histology report described a 105 g, 65×50×35 mm sized, fragmented adrenal mass, in encapsulated focal areas, coloured yellowish and orange. Microscopically, well-demarcated adrenal cortical adenoma which was structured by clear cells and eosinophilic cells, was located under the capsule (figure 1). Myelolipoma was composed of mature adipose tissue and mature myeloid elements were found in focal areas of adenoma. Myelolipoma approximately 10 mm diameter, having haemorrhagic foci but without calcification and necrosis was observed.
Figure 1.
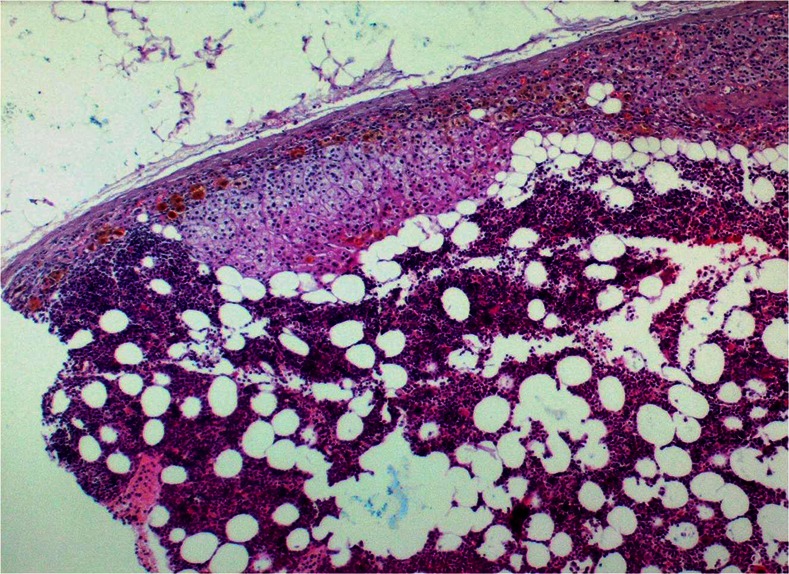
Located under capsulate adenocortical adenoma, myelolipoma foci (H&E stain-magnification ×40).
Differential diagnosis
The differential diagnosis of myelolipomas includes renal angiomyolipoma, retroperitoneal lipoma and liposarcoma. For the diagnosis of these fatty tumours of the adrenal gland, CT and sonograpy are sensitive and important imaging techniques.
Treatment
Laparoscopic right adrenalectomy was applied to the patient.
Outcome and follow-up
Postoperatively, the patient's recovery was uneventful.
Discussion
Myelolipomas are small, asymptomatic and non-functional tumours. Although the benign nature of these lesions is proved, it is unclear how this tumour develops. Thus, pathogenesis of myelolipomas is still uncertain. There are different explanations about this matter but according to a widely participated theory, pathogenesis of myelolipomas occurs in response to stimuli, such as, necrosis, infection or stress, reticuloendothelial cells of blood capillaries in the adrenal glands with metaplasia.4
Histological examinations of myelolipomas prove that haematopoietic elements, consisting of myeloid and erthyroid precursors, as well as, megakaryocytes, are interspersed within adipocytes. Our case also followed the same path. Myelolipomas, in fact, equally affect both sexes between the age of 50 and 70.5 Our case confirms this, because the patient examined in this paper is a 66-year-old man. According to reported cases, examined patients were all women ranging between 26 and 50 years, with a mean of age 34 years. Most of the cases originated from the left side. But in our case, the tumour was located in right adrenal region.
The adrenal cortical adenoma was encapsulated by a thin layer of connective tissue. The tumour was composed of clear cells and eosinophilic cells arranged in an alveolar structure (figure 2).3 In this case, in the tumour, well-demarcated myelolipoma was found under a capsule, in focal areas. The size of the tumours may vary from a few millimetres to 34 cm and they account for about 8% of adrenal ‘incidentalomas’. The tumour size up to 4 cm is not treated but any tumour over 4 cm requires surgical excision.2 In this case, the adrenal mass was 60×35 mm and therefore patient under went laparoscopic surgery. Three radiological patterns for adrenal myelolipomas are described: isolated adrenal myelolipomas, myelolipomas with haemorrhage and complex lesions with small myelolipomatous foci within other adrenal tumours (non-functional adenoma, adrenocortical adenoma, Conn's syndrome) often with extensive calcifications.6 In our case, according to histological examinations, myelolipoma and non-functional adrenal cortical adenoma were found together. This coexistence of two is a rare in the literature, which makes our research interesting.
Figure 2.
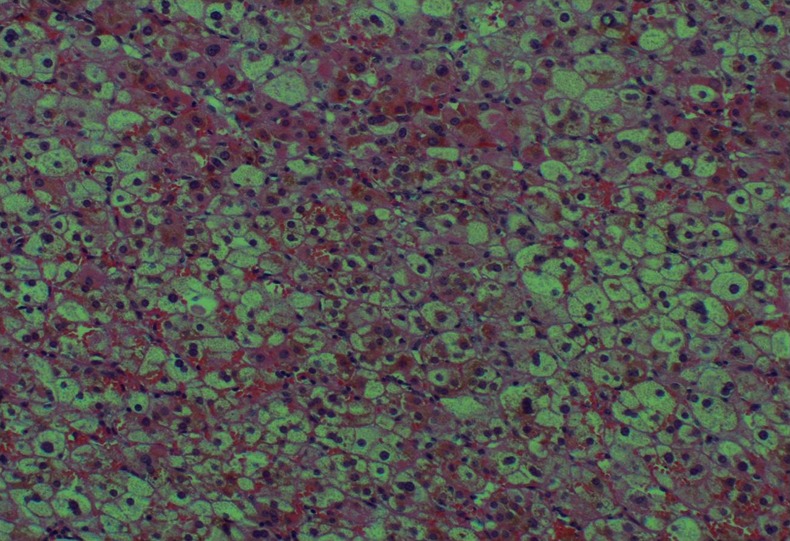
Adrenocortical adenoma appears characteristic alveolar architecture and lipid-rich cells (H&E stain-magnification ×200).
Recent studies by Linwah Yip et al confirmed that 61 out of 66 histopathological cases of adrenal masses with imaging characteristics supported benign adenoma and remaining the five consisted benign non-adenomatous lesions: three myelolipomas, one composite myelolipoma/adenoma and one ganglioliponeuroma. This research proved that specificity of imaging techniques for benignity are accurate and affective to recognise benignity.7 In this research, malignant adrenal lesions were diagnosed in 17 out of 130 patients in which eight metastases, seven adrenal cortical carcinomas, one epithelioid angiosarcoma and one ganglioneuroblastoma were attained. Imaging techniques also achieved total success identifying malignancy. Both in this study there was correlation between imaging and histopathological findings.
The differential diagnosis of myelolipomas includes renal angiomyolipoma, retroperitoneal lipoma and liposarcoma. For the diagnosis of these fatty tumours of the adrenal gland, CT and sonograpy are sensitive and important imaging techniques. If the case contained myeloid material with extensive calcification or haemorrhage, the fat content may not be recognised. Major difference between myelolipomas and other adrenal neoplasm is the presence of mature fat. For those tumours, histopathological examination is required for description of myelolipoma.8
In conclusion, we decided to submit this research paper because, according to study of the related literature, correlation of adrenocortical adenoma and myelolipoma is a rare case of benignity, as in our patient.
Learning points.
In general perception, myelolipoma is non-functional, rare and benign tumour. Adrenocortical adenoma is also benign.
The main aim of this paper is that myelolipoma and adrenocortical adenoma are located in same adrenal gland. According to literature it is rare case.
For the diagnosis of this tumour of the adrenal gland, CT and sonograpy are sensitive and important imaging techniques. Surgery is performed in symptomatic cases.
Footnotes
Contributors: EG mainly did this research under HS advisory. SB and MFI double checked the paper and made necessary comments on it.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Al Harthi B, Riaz MM, Al Khalaf AH, et al. Adrenal myelolipoma a rare benign tumour managed laparoscopically: report of two cases. J Minim Access Surg 2009;2013:118–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Amin MB, Tickoo SK, Schultz D, et al. Myelolipoma of the renal sinus. Arch Pathol Lab Med 1999;2013:631–4 [DOI] [PubMed] [Google Scholar]
- 3.Repassy DL, Csata S, Sterlik G, et al. Case report I giant adrenal myelolipoma. Pathol Oncol Res 2001;2013:72–3 [DOI] [PubMed] [Google Scholar]
- 4.Wani NA, Kosar T, Rawa IA, et al. Giant adrenal myelolipoma: incidentaloma with a rare incidental association. Urol Ann 2010;2013:130–3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Manassero F, Pomara G, Rappa F, et al. Adrenal myelolipoma associated with adenoma. Int J Urol 2004;2013:326–8 [DOI] [PubMed] [Google Scholar]
- 6.Yildiz L, Akpolat I, Erzurumlu K, et al. Giant adrenal myelolipoma: case report and review of the literature. Pathol Int 2000;2013:502–4 [DOI] [PubMed] [Google Scholar]
- 7.Yip L, Tublin ME, Falcone JA, et al. The adrenal mass: correlation of histopathology with imaging. Ann Surg Oncol 2010;2013:846–52 [DOI] [PubMed] [Google Scholar]
- 8.Matsuda T, Abe H, Takase M, et al. Case of combined adrenal cortical adenoma and myelolipoma. Pathol Int 2004;2013:725–9 [DOI] [PubMed] [Google Scholar]