

Abstract
Conventionally, patients presenting with hip pain and restricted mobility to accident and emergency (A&E) department are thought to have musculoskeletal pain. Occasionally, patients with significant abdominal pathology can present with hip pain. Such atypical presentation causes the delayed diagnosis leading to significant morbidity and possible mortality. We report a 63-year-old man who had been treated in A&E on numerous occasions with left hip pain for over 6 weeks. On this occasion, he had been brought in septic shock. On examination, he had subcutaneous emphysema of left lower limb. A CT scan showed a large psoas abscess resulting from retroperitoneal perforation of sigmoid diverticulitis tracking into his left lower limb. He underwent a Hartmann's procedure and drainage of his intra-abdominal sepsis. The thigh was not drained with separate incisions at the index operation. Residual thigh abscess was managed by image-guided drainage.
Background
Conventionally, patients presenting with hip pain and restricted mobility to accident and emergency (A&E) department are thought to have musculoskeletal pain. Rarely, patients with significant abdominal pathology such as appendicitis and diverticulitis can present with hip pain. Diverticulitis presenting as hip pain is rare with only 15 reported cases in the literature.1 2 Such atypical presentation causes delayed diagnosis leading to significant morbidity and possible mortality.2
We report a case of psoas abscess secondary to retroperitoneal perforation of sigmoid diverticulitis presenting with hip pain. The patient had been examined in A&E on numerous occasions over a 6-week period with hip pain and restricted mobility that was misdiagnosed as musculoskeletal pain. He presented in septic shock, and on examination was found to have surgical emphysema of his left lower limb. After appropriate imaging, he underwent a Hartmann's procedure. The soft tissue infections of his left lower limb were treated with radiological drainage.
Through this report, we would like to highlight the need for a high index of suspicion for other causes of hip pain, especially in patients returning to A&E with the same or unresolved complaints.
Case presentation
A 63-year-old man was brought out of hours into A&E in a state of circulatory collapse. He had been seen and treated in A&E with left hip pain and restricted mobility on numerous occasions over the preceding 6 weeks. He also reported a fall prior to the onset of his symptoms. In addition, he presented with diarrhoea, weight loss and poor appetite that started about 2 weeks prior to onset of his left hip pain. In this same duration, his mobility had progressively reduced to the point of needing help with basic activities of daily living. His medical history included type 2 diabetes and degenerative spinal discs.
On examination, he was feverish, tachypnoeic, tachycardic and hypotensive. His oxygen saturation was 96% on air. He had signs of localised peritonitis in his left iliac fossa (LIF). The rest of his abdomen was soft with no signs of generalised peritonitis. He had some degree of fixed flexion deformity of his left hip and knee and painful movement of his left hip. He also had an oedema of left lower limb.
Investigations
Routine blood tests taken on admission showed a haemoglobin 9.4 g/dl, white cell count 17.6×109/l, neutrophils 16.9×109/l and C reactive protein 168 mg/l. Glucose, liver function tests, urea, creatinine and electrolytes were all normal. No abnormalities were found on chest and abdominal x-rays. Pelvic and left thigh x-rays were requested in view of the patient's presentation. These are shown in figures 1 and 2. As seen, both these x-rays showed surgical emphysema, but these were initially misinterpreted as radiological artefact.
Figure 1.

X-ray of the pelvis showing extensive surgical emphysema.
Figure 2.

X-ray of the left thigh showing extensive surgical emphysema.
The gentleman continued to deteriorate and the x-rays were discussed with the radiologist the next morning. A CT of the abdomen, pelvis and lower limbs was performed in view of the x-ray findings. The CT images are shown in figure 3A,B.
Figure 3.
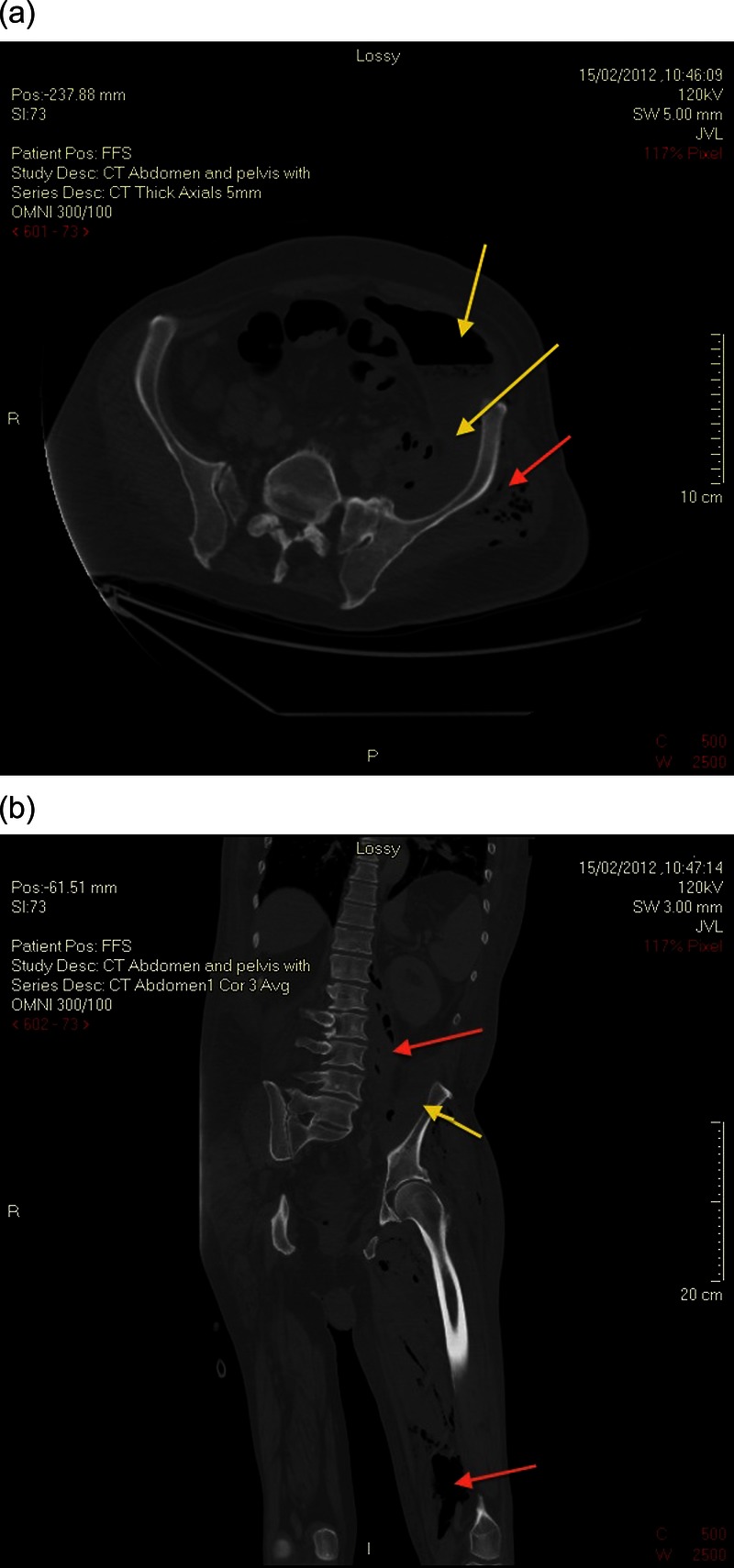
(A) Axial section of the CT showing retroperitoneal abscess and surgical emphysema. (B) Coronal section of the CT showing retroperitoneal abscess and surgical emphysema of left lower limb.
A large complicated ilio-psoas collection, at least 15 cm×5.5 cm diameter, was identified. There is also surgical emphysema extending distally along the left thigh to the level of the upper calf and posteriorly to the left gluteal muscles. The amount of gas present suggested communication to the colon.
Differential diagnosis
Initial working diagnosis was the septic arthritis of the left hip. A surgical consultation was only sought in view of LIF tenderness. In view of his general condition, a diagnosis of complicated diverticulitis was also entertained by the surgical team.
Post-CT scan, the ilio-psoas abscess was thought to be most likely to be secondary to perforated sigmoid colon. In view of paucity of bowel symptoms and the protracted presentation and a history of fall prior to the onset of symptoms, differential diagnoses of the infected haematoma and pyonephrosis were also considered.
Treatment
This man was initially treated with a broad-spectrum of antibiotics from sepsis of unknown origin. After the CT scan, the following day, he was taken to theatre for a laparotomy. At laparotomy, a large inflammatory mass was found in relation to the sigmoid colon secondary to posterior perforation of sigmoid diverticulitis. He underwent a Hartmann's procedure. This also drained the retroperitoneal abscess. Suction drains ×2 were inserted into the thigh through the infra-inguinal communication along the psoas tendon. No formal incisions were made to drain the soft tissue infection of the left lower limb.
Postoperatively, he needed level 1 care for 2 weeks duration. He had a slow, but full, recovery. He did develop small collections in the leg which needed radiological drainage.
Outcome and follow-up
The patient made a complete recovery and was discharged home fully ambulant following a period of rehabilitation.
Discussion
Diverticulitis presenting as leg pain is very rare. There are about 15 reported cases in the literature.1 Of these patients, 13 had surgical emphysema of soft tissue spaces of the thigh. Their management has been heterogeneous with variable results. Most of them have been reported in the pre-CT era and management has involved exploration and debridement of the thigh with faecal diversion.1
Psoas abscess is a condition traditionally associated with tuberculosis of the spine.3 4 In recent years, gastrointestinal (GI) diseases such as appendicitis, malignancy, Crohn's disease and, less frequently, diverticulitis have been reported as causes for psoas abscess.2 3 4 In their study, Tabrizian et al4 found that the inflammatory bowel disease was the most common cause of GI causes for psoas abscess.
More recently, CT is being increasingly used for the diagnosis and assessment of both diverticulitis and psoas abscess. Image-guided aspiration and percutaneous drainage are the preferred treatment of non-tuberculous psoas abscesses greater than 3 cm.4 However, those secondary to GI causes usually need a subsequent surgical intervention to treat the underlying primary pathology.4
Mekhail2 has reported safe usage of conservative approach for treating the psoas abscess following treatment of the primary pathology (appendicular abscess in their case).
We adopted a strategy of treatment of the primary pathology and conservative approach to treat the surgical emphysema of the leg. In our case, there was extensive surgical emphysema extending to the leg, but no obvious collections in the thigh or leg. Also, the abscess was limited to the retro-peritoneum on the CT. We placed a drain from above at the index operation and closely monitored the leg for any signs of spreading infection. The limb was imaged when appropriate, and collections were drained with image guidance with good outcome.
We suggest that, where image-guided percutaneous drainage is available, a treatment of primary GI pathology followed by percutaneous drainage of the limb may be the way forward to manage this rare presentation of diverticulitis and to avoid the morbidity associated with leg surgery.
Learning points.
High index of suspicion for rare presentation of common diseases.
‘Looking outside the box’ when interpreting investigations.
Evidence-based management of uncommon presentations.
Conservative approach to limb problems after dealing with the primary cause.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Haiart DC, Stevenson P, Hartley RC. Leg pain: an uncommon presentation of perforated diverticular disease. J R Coll Surg Edinb 1989;2013:17–20 [PubMed] [Google Scholar]
- 2.Mekhail P, Saklani A, Philobos M, et al. Thigh subcutaneous emphysema: is that a clear indication for thigh exploration? JSCR 2011;2013:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.de Jesus Lopes Fihlo G, Matone J, Arasaki CH, et al. Psoas abscess: diagnostic and therapeutic considerations in six patients. Int Surg 2000;2013:339–43 [PubMed] [Google Scholar]
- 4.Tabrizian P, Nguyen SQ, Greenstein A, et al. Management and treatment of iliopsoas abscess. Arch Surg 2009;2013:946–9 [DOI] [PubMed] [Google Scholar]