

Abstract
A grossly obese woman was wrongly diagnosed throughout her adult life of having lymphoedema. Her condition was subsequently confirmed as lipoedema, an entirely different condition, which is noted in medical text books but is seldom taught to medical students or to general practitioners. The condition is caused by abnormal deposition of adipose tissue in the extremities (usually the lower limbs) and almost exclusively affects women. It often starts at puberty or may occur after pregnancy. The exact aetiology is not yet understood but genetic and hormonal factors may be implicated. The problem is that misdiagnosis leads to inappropriate tests and improper treatment to the patient. When recognised it is often too late to do anything for the patient and they become highly dependent on social care. This case describes how the diagnosis can be confirmed through an ultrasound image and illustrates the need for early recognition to facilitate specialist care.
Background
This condition is rarely diagnosed and there are only a few reports in the literature. This is because there is a lack of knowledge but also by the fact the ultrasound diagnostic test was only recently reported.
When recognised it is often too late to do anything for the patient and they become highly dependent on social care. This case describes how the diagnosis can be confirmed through an ultrasound image and illustrates the need for early recognition to facilitate specialist care.
Case presentation
A 38-year-old lady was admitted to hospital after a fall and was diagnosed as having cellulitis of her legs, which was treated with antibiotics.
Incidentally she was noted to have massive bilateral leg swelling (figure 1) which she had always attributed to being ‘overweight’. She reported that her legs had been abnormally large, disproportionate to the rest of her body, since around the time of puberty but had become increasingly large with time. Attempting weight loss by dieting had never helped to reduce the size of her legs. She reported a history of easy bruising and haematoma formation with minimal trauma.
Figure 1.

The typical features of lipodema with symmetrical distribution of the tissue in the hips, buttocks and legs with sparing of the feet causing ‘shouldering’ at the ankle. Of note there is marked disproportion between the torso and the affected limbs.
Her medical history included osteoarthritis of the hips, depression, irritable bowel syndrome and asthma. Of note she was also claustrophobic. She had never travelled abroad and there was no family history of leg swelling.
Clinically she had symmetrical bilateral leg swelling from the ankles to hips disproportionate to her upper body. The legs were tender on minimal palpation, were warm and well perfused and of normal colour. There was minimal pitting oedema and Stemmers sign was absent.
Investigations
High-resolution cutaneous ultrasonography was used to aid the diagnosis in addition to the clinical presentation. Normal dermal thickness and dermal hypoechogenicity (figure 2, distance A) was indicative of lipoedema and not lymphoedema wherein the latter this demarcation between the layers is lost.
Figure 2.
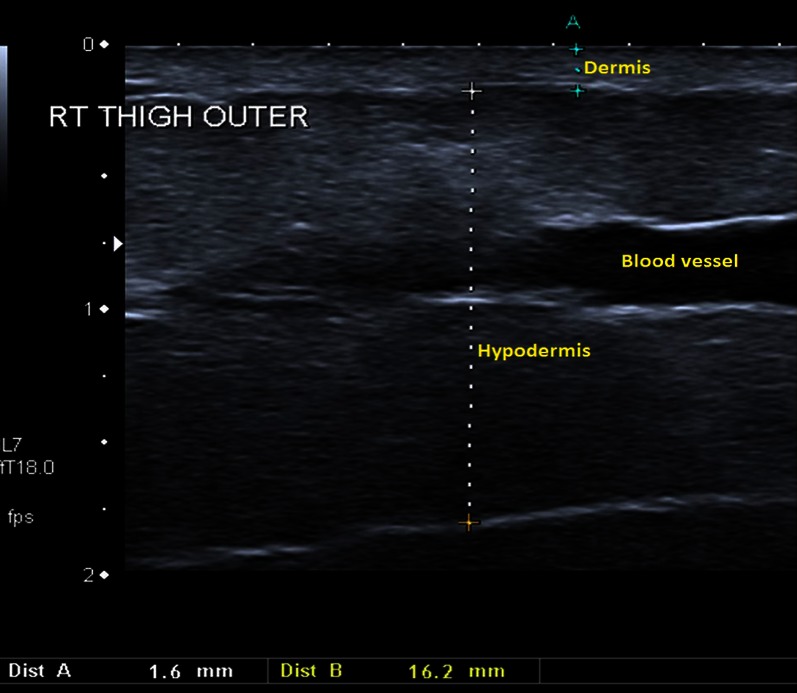
Ultrasound of the lateral thigh demonstrating normal dermal thickness.
Differential diagnosis
Main differences between lipoedema and lymphoedema
Lipoedema
Swelling of the lower limbs (and sometimes arms) which is symmetrical (the same on both sides).
The swelling is usually soft and often comprises of loose, floppy, connective tissue and fat.
There is often a pad of fat just under the knees and hips.
Feet (or hands) are usually not affected (giving the appearance of a ‘bracelet effect’ at the ankles/wrists). However, as the disease progresses over time, the hands and feet can become swollen.
Pitting (firm pressure on the skin leaving obvious indentations) of the skin is not present.
Pain in the joints, especially the knees is often reported.
Tenderness of the tissues can also be a feature.
Limbs will often bruise easily.
Risk of infection in affected areas is no greater than normal.
The affected skin condition is usually soft and supple and not thickened.
Affects women only.
Does not seem to respond to losing weight.
There is often a family history of the condition.
Lymphoedema
Swelling may be unequal on each side of body—one limb is often much larger than the other.
Feet are frequently affected.
Pitting of the skin will be present—especially in the early stages of the condition.
No pain is felt if pressure is applied to the skin, but there is often a feeling of tightness in the tissues.
Limbs do not tend to bruise easily.
Increased risk of infection (cellulitis) in affected, swollen areas.
Can affect women and men of any age.
The affected skin is often thickened and may have other features such as warty change or papillomatosis (cobble stone effect on the skin).
Losing weight usually has a beneficial effect on the swelling.
In 20% there is a family history of the condition.
Adapted from the LSN—the Lipoedema Support Network http://lymphoedema.org/Menu7/Index.asp
Treatment
After being successfully treated with antibiotics for cellulitis the patient was then transferred to a local hospital for a period of rehabilitation to improve her mobility and level of function. Upon discharge from hospital she was referred to a specialist lipoedema clinic run by Professor Peter Mortimer at St George's Hospital, London.
Discussion
Based on the clinical history and appearance, this lady was diagnosed as having lipoedema, an infrequently diagnosed condition first described by Allen and Hynes in 1940.1 Often patients are mislabelled as simply being obese or having lymphoedema—a different clinical entity. The condition is caused by the abnormal deposition of adipose tissue in the extremities (usually the lower limbs) and almost exclusively affects women. It often begins at around the time of puberty or may occur after pregnancy. The exact aetiology is not yet understood although Child et al2 suggest that genetic and hormonal factors play a role and propose that the condition is either X-linked dominant inheritance or autosomal dominant with sex limitation. The distribution of the tissue is symmetrical and characteristically involves the hips, buttocks and legs. Typically there is sparing of the feet with ‘shouldering’ at the ankle. There is often marked disproportion between the torso and the affected limbs. Tenderness on palpation of the tissue and easy bruising and haematoma formation with only the slightest insult are also characteristic.3 Stemmers sign—the inability to pinch up a fold of skin at the base of the second toe—is absent in pure lipoedema whereas this test is positive in lymphoedema. Contrary to what the name suggests oedema is not a key feature and the swelling is caused by adipose tissue and not fluid. There may be associated dependent oedema but this makes only a small contribution to the swelling. The true incidence of the condition is not entirely clear and figures in the literature on the subject show wide variability, possibly owing to the infrequent recognition of the condition. Overall, the condition is thought to be relatively rare3 and is distinct from simple obesity. The general physician should be aware of its existence.
Learning points.
Lipoedema could easily be misdiagnosed as lymphoedema; however, with a little knowledge of the typical features of each this need not be the case.4 As with a lot of medicine, history and examination are key to clinching the diagnosis. This was crucial in our case, whereby the use of ultrasound imaging was primarily to confirm the diagnosis.5 A history of easy bruising and haematoma formation, tenderness on palpation and onset after puberty would be typical of lipoedema. On examination one of the key features which can differentiate between the pure forms of each condition is the sparing of the feet and hands seen in lipoedema where there is often a visible step or ‘shouldering’ at the ankle. Skin changes with thickening and fibrosis are seen in lymphoedema and this is why one often cannot pinch a fold of skin at the base of the second toe—known as a positive Stemmer's test.6
Footnotes
Contributors: JMG and JOMO wrote paper under SR's supervision. AB performed the ultrasonic diagnosis.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Allen EU, Hines EA. Lipedema of the legs: a syndrome characterized by fat legs and orthostatic edema. Proc Staff Mayo Clin 1940;2013:184–7 [Google Scholar]
- 2.Child AH, Gordon KD, Sharpe P, et al. Lipedema: an inherited condition. Am J Med Genet A 2010;2013:970–6 [DOI] [PubMed] [Google Scholar]
- 3.Reich-Schupke S, Altmeyer P, Stücker M. Thick legs—not always lipedema. J Dtsch Dermatol Ges 2013;2013:225–33 [DOI] [PubMed] [Google Scholar]
- 4.Shin BW, Sim YJ, Jeong HJ, et al. Lipedema, a rare disease. Ann Rehabil Med 2011;2013:922–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Naouri M, Samimi M, Atlan M, et al. High-resolution cutaneous ultrasonography to differentiate lipoedema from lymphoedema. Br J Dermatol 2010;2013:296–301 [DOI] [PubMed] [Google Scholar]
- 6.Mortimer PS. Swollen lower limb-2: lymphoedema. BMJ 2000;2013:1527–9 [DOI] [PMC free article] [PubMed] [Google Scholar]