

Abstract
A rupture or avulsion of the triceps tendon is very rare but concomitant elbow injuries with avulsion of the triceps tendon are even rarer. In this study, an extraordinary and unusual injury combination (radial head and trochlear fracture associated with triceps tendon avulsion), which happened during a fall onto the elbow with outstretched hand, was identified and has been discussed in the literature.
Background
Triceps tendon ruptures are rare injuries that comprise less than 1% of all tendon ruptures.1 Either direct or indirect mechanisms may play a role in triceps tendon rupture. A direct blow to the elbow, stab wounds or lacerations may cause distal triceps rupture. However, the most common mechanism of injury is a sudden forceful contraction of the triceps muscle during a fall onto an outstretched hand.2–4 As a fall onto an outstretched hand is a common mechanism of injury for several other elbow and upper extremity injuries, associated injuries may occur simultaneously with triceps tendon ruptures. It usually occurs due to a direct force, and less frequently due to an indirect force.1 2 Triceps tendon avulsion (TTA) may be isolated or associated with elbow-related fractures such as radial head and olecranon fractures.4–6 These types of combined injuries may easily go unnoticed due to extensive swelling around the elbow, presence of pain and lack of clinical suspicion. If not diagnosed, associated injuries to elbow fractures (including TTA) may lead to loss of function in the long term.7
Case presentation
A 17-year-old man presented at the outpatient orthopaedic clinic with a history of radial head fracture. He stated that he had attended the emergency department (ED) after he had fallen on his outstretched hand during a football game 12 days previously, and elbow radiographs had been taken. A long arm plaster cast had been applied in the ED for a diagnosis of non-displaced radial head fracture.
Re-evaluation of the elbow radiographs taken at the initial admission revealed a non-displaced radial head fracture and a small flake-like fragment posterior and proximal to the tip of olecranon (figure 1). The plaster cast was therefore removed, and on physical examination there was mild swelling over the entire elbow. There was marked tenderness over the radial head with palpation and forearm rotations. The tip of the olecranon was also tender and a gap was palpable over the triceps tendon (figure 2). Active and passive elbow movements were all painful and restricted, particularly active elbow extension could not be performed.
Figure 1.
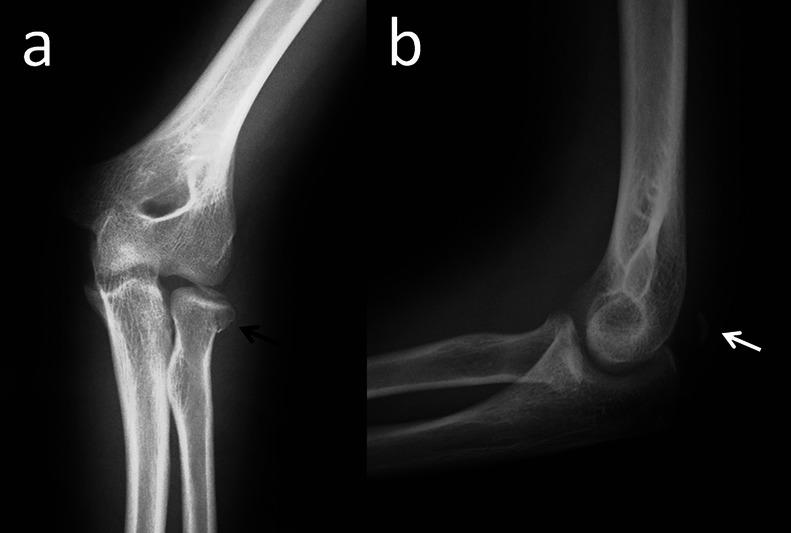
Direct elbow radiographs on initial admission.
Figure 2.

A gap between the triceps tendon stump and olecranon tip with palpation.
Investigations
On the basis of these radiographic and clinical findings, radial head fracture associated with triceps tendon rupture was presumed and a MRI scan was obtained. MRI showed a complete rupture of the triceps tendon with a non-displaced fracture of the radial head and an osteochondral fracture fragment in the ulna-trochlear joint space (figure 3). In order to understand the fracture geometry and the origin of the fragment, further CT was ordered. Elbow CT demonstrated the trochlear fracture (figure 4).
Figure 3.
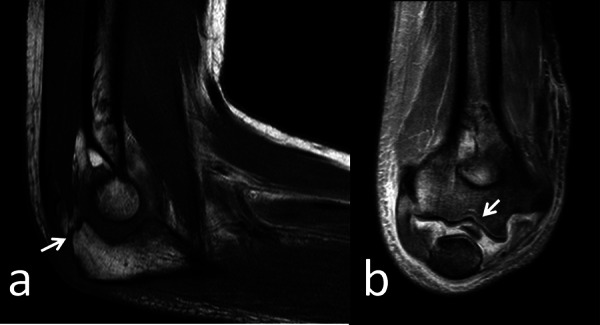
(A) Sagittal T1_TSE MRI demonstrates complete rupture of the triceps tendon (white arrow). (B) Coronal proton-density-weighted TSE image shows the osteochondral fragment within the ulna-humeral joint space (white arrow).
Figure 4.
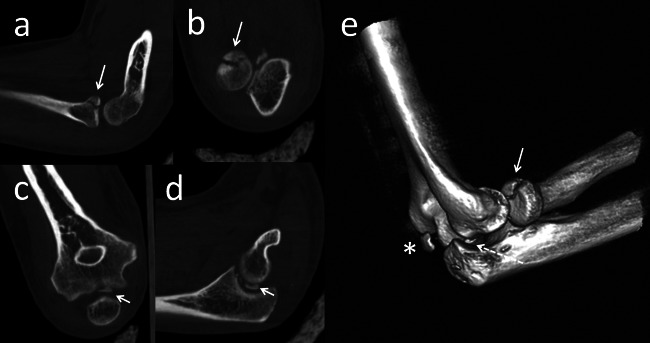
CT examination of the patient.
Treatment
The patient was treated for triceps tendon repair using transosseous suture technique and the trochlear osteochondral fragment was excised (figure 5). No additional intervention was performed for the radial head fracture as it was not displaced and not blocking rotational movements.
Figure 5.

(A) Intraoperative appearance of the case. (B) Excised osteochondral fracture of the trochlea.
Outcome and follow-up
The postoperative course was uneventful. After 3 weeks of immobilisation, active and passive range of motion exercises were started and increased gradually. At the final follow-up 9 months after the operation, the patient was free of pain with full range of elbow movements (figure 6).
Figure 6.
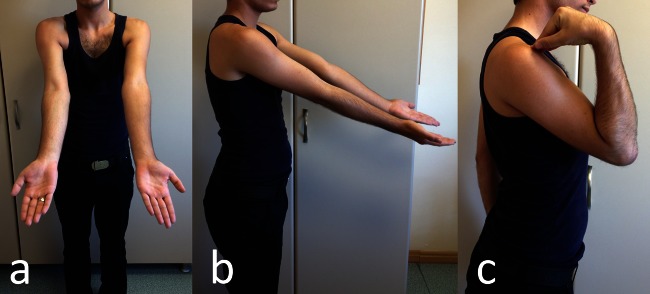
Functional result of the patient at the final follow-up.
Discussion
TTA injuries are rare but may be associated with common fractures such as radial head or other inside joint fractures.3 6 8 In the case presented here, the radial head fracture and TTA were associated with the trochlear osteochondral fracture fragment. To the best of our knowledge, this is the first such report in literature of a combined injury including radial head fracture, TTA and trochlear fracture.
According to Levy et al, TTA occurs due to the forceful contraction of the triceps tendon during a fall onto an outstretched hand with the elbow extended. Simultaneous twisting and abduction of the elbow leads to radial head fractures.3 Rahmi et al4 similarly described the injury mechanism as the sudden contraction of the triceps muscle and extension of the elbow during a fall onto an outstretched hand. In our case the injury occurred during a fall onto an outstretched hand with elbow over-extension.
TTAs (ruptures) may be overlooked during the initial examination in 45% of cases.6 7 9 TTA may not be detected due to the trauma causing pain around the elbow and mis-perception of tenderness on the radial side.5 In the case presented here, elbow extension was weak but actively present probably because of the remaining anconeus muscle fibres. TTA was suspected due to the extensive swelling of the elbow and ecchymosis, which complied with the literature.3 5 6 9 These findings suggested that the presence of a palpable gap in the posterior elbow is a more valuable symptom than loss of active elbow extension in the diagnosis of TTA.
Triceps tendon injuries most commonly occur as total or partial avulsion of the tendon from the olecranon tip.2 9 Likewise, in the current case, the tendon was found to be ruptured from the triceps olecranon in the form of avulsion during surgery. The most important radiological evidence has been seen to be the lateral elbow radiograph, which demonstrates the presence of a flake from the bone just behind the posterior olecranon fossa.3 7 8 Accordingly in the current case, the elbow radiograph clearly demonstrated a tiny posterior bone fragment at the proximal of the olecranon tip (figure 1).
Yoon et al5 stated that if the lateral radiograph reveals a bone flake, MRI is not required to diagnose TTA. According to Gaines et al,10 MRI demonstrates the extent of the tendon rupture and is beneficial in deciding the timing of the surgery. In our opinion, a palpable gap in the posterior elbow with the presence of a bone flake in the lateral radiograph strengthens the diagnosis of TTA. Notwithstanding, MRI is necessary for treatment planning and should therefore be taken routinely.
The most common surgical method in TTA is to anchor the triceps tendon to the olecranon tip with non-absorbable suture materials through the tunnels drilled in the bone.4 5 7 K-wires and cerclage wires are other materials included in suture anchoring in surgical treatment.5 11 12 In the current case, surgical treatment included transosseous repair of the triceps tendon with non-absorbable suture material and excision of the trochlear osteochondral fragment. To avoid any interference with the rotation of the elbow joint, no additional treatment was applied to the radial head fracture.
Learning points.
Injuries associated with radial head fractures including triceps tendon avulsion (TTA) require a high level of attention and scepticism in diagnosis.
In the presence of extensive swelling and pain around the elbow joint after a fall onto an outstretched hand, MRI should be routinely applied and added to the radiographies. An advanced level of scepticism, careful physical examination and further tests such as MRI will make it easier to diagnose associated injuries.
Palpable gap over the triceps tendon and inability to extend elbow against gravity are the key physical examination findings for TTA. The presence of a palpable gap in the posterior elbow is a more valuable symptom than loss of active elbow extension in the diagnosis of TTA.
Appropriate diagnosis and surgical treatment of the TTA and other interjoint fractures will prevent the symptoms continuing after recovery.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Anzel SH, Convey KW, Weiner AD, et al. Disruption of muscles and tendons: an analysis of 1014 cases. Surgery 1959;2013:406–14 [PubMed] [Google Scholar]
- 2.Rajasekhar C, Kakarlapudi TK, Bhamra MS. Avulsion of the triceps tendon. Emerg Med J 2002;2013:271–2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Levy M, Fishel RE, Stern GM. Triceps tendon avulsion with or without fracture of the radial head. A rare injury? J Trauma 1978;2013:677–9 [DOI] [PubMed] [Google Scholar]
- 4.Rahmi M, Arssi M, Hattoma N, et al. Traumatic avulsion of the triceps tendon with fracture dislocation of the elbow. Pan Arab J Orthop Trauma 2001;2013:25–7 [Google Scholar]
- 5.Yoon MY, Koris MS, Ortiz JA, et al. Triceps avulsion, radial head fracture, and medial collateral ligament rupture about the elbow: a report of 4 cases. J Shoulder Elbow Surg 2012;2013:e12–17 [DOI] [PubMed] [Google Scholar]
- 6.Chamseddine AH, Jawish MR, Zein HK. Avulsion of the distal triceps tendon with fracture of the radial head. Eur J Orthop Surg Traumatol 2011;2013:607–10 [Google Scholar]
- 7.Riet VR, Morrey BF, Ho E, et al. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am 2003;2013:1961–7 [DOI] [PubMed] [Google Scholar]
- 8.Levy M, Goldberg I, Meir I. Fracture of the head of the radius with a tear or avulsion of the triceps tendon. A new syndrome? J Bone Joint Surg 1982;2013:70–2 [DOI] [PubMed] [Google Scholar]
- 9.Chan APH, Lo CK, Lam HY, et al. Unusual traumatic triceps tendon avulsion rupture: a word of caution. Hong Kong Med J 2009;2013:294–6 [PubMed] [Google Scholar]
- 10.Gaines ST, Durbin RA, Marsalka DS. The use of magnetic resonance imaging in the diagnosis of triceps tendon ruptures. Contemp Orthop 1990;2013:607–11 [PubMed] [Google Scholar]
- 11.Bava ED, Barber AF, Lund ER. Clinical outcome after suture anchor repair for complete traumatic rupture of the distal triceps tendon. Arthroscopy 2012;2013:1058–63 [DOI] [PubMed] [Google Scholar]
- 12.Pina A, Garcia I, Sabater M. Traumatic avulsion of the triceps brachii. J Orthop Trauma 2002;2013:273–6 [DOI] [PubMed] [Google Scholar]