

Description
A 55-year-old man with a medical history of intrahepatic cholangiocarcinoma treated with gemcitabine and cisplatin with tumour chemoembolisation. However, the patient failed the initial therapy and was subsequently switched to fluorouracil and oxaliplatin with folinic acid. CT of the chest and abdomen showed new lesions consistent with metastatic disease in the liver and lungs and worsening ascites.
In February 2013, the patient was admitted to the hospital because of progressive left upper extremity weakness and a mechanical fall. The brain MRI showed right subcortical frontal lobe enhancing lesion concerning for metastatic disease (figure 1). Neurosurgical service was consulted for possible biopsy. Neurosurgery deferred the need for biopsy and the patient was started on whole-brain radiation therapy with resolution of his neural symptoms. Unfortunately, the patient died 1 month after brain irradiation.
Figure 1.
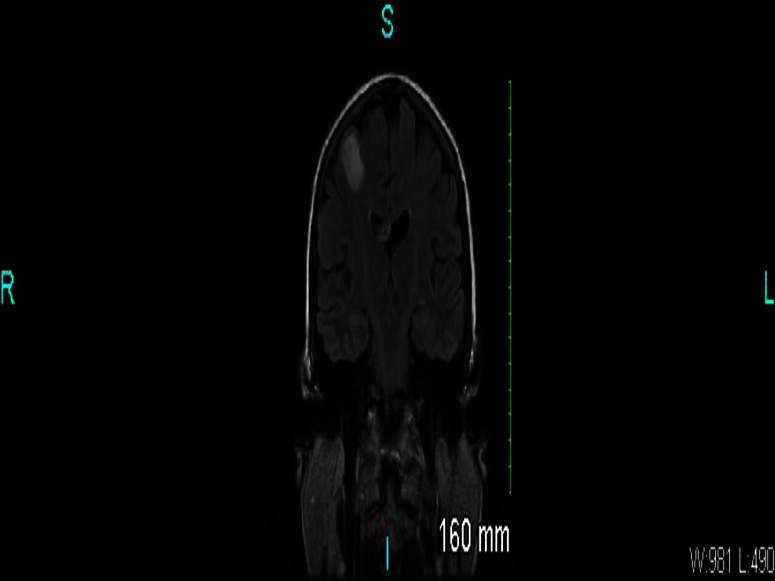
White matter right frontal lobe enhancing lesion concerning for metastatic disease.
Cholangiocarcinoma is a rare tumour arising from either extrahepatic or intrahepatic bile ducts with an approximate occurrence of 30 640 new cases annually in the USA.1 Common risk factors include pre-existent liver and biliary disease, parasitic diseases involving biliary tree, diabetes, obesity, HIV infection and toxic exposures.2 Surgical resection is the mainstay of treatment for cholangiocarcinoma.3 However, many times the disease is present at an advanced stage making surgery not amenable.
The presence of brain metastasis owing to cholangiocarcinoma is an extremely rare event, with only a few published reports. In a most recent report from Thailand, the incidence rate of brain metastases was only 0.15% and was associated with a decreased survival.4 Cholangiocarcinoma is known to be a poorly vascularised tumour, which may explain why patients with cholangiocarcinoma rarely develop brain metastases.
In conclusion, despite being an extremely rare finding, brain metastases from cholangiocarcinoma may occur. The presences of brain metastases portray an extremely poor prognosis.2 Therefore, clinicians should keep their minds open and consider brain metastases in patients with cholangiocarcinoma and with a new onset of neurological symptoms.
Learning points.
Cholangiocarcinoma is a rare tumour arising from intrahepatic or extrahepatic bile ducts.
Brain metastases from cholangiocarcinoma are extremely rare.
Poor tumour vascularisation may explain why the tumour rarely metastasise to the central nervous system.
Clinicians should keep their minds open and consider brain metastases in patients with cholangiocarcinoma with a new onset of neurological symptoms.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin 2013;2013:11–30 [DOI] [PubMed] [Google Scholar]
- 2.Tyson GL, El-Serag HB. Risk factors for cholangiocarcinoma. Hepatology 2011;2013:173–84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Friman S. Cholangiocarcinoma—current treatment options. Scand J Surg 2011;2013:30–4 [DOI] [PubMed] [Google Scholar]
- 4.Chindaprasirt J, Sookprasert A, Sawanyawisuth K, et al. Brain metastases from cholangiocarcinoma: a first case series in Thailand. Asian Pac J Cancer Prev 2012;2013:1995–7 [DOI] [PubMed] [Google Scholar]