

Abstract
We report a greenstick fracture of the patella in an ambulant boy with diplegic cerebral palsy (CP). The boy was known to have knee crouch which was documented in our gait laboratory. Greenstick fractures usually occur in the long bones of children and are caused by a bending force. This is the first report of a patellar greenstick fracture and provides a unique insight into the propagation of patellar fractures in CP crouch.
Background
Fractures of the patella occur rarely in normal children as a result of forced knee flexion during sporting activities.1–5 We have recently reported their occurrence in cerebral palsy (CP) diplegia with mild knee crouch in the absence of an acute injury.6 We believe that knee crouch in CP diplegia puts excessive tension on the extensor mechanism and is the primary cause of the fracture.7 A greenstick fracture of the long bones is common in children but such a fracture, described also as an incomplete fracture, has not, to our knowledge, been reported for the patella. This case report confirms the mechanism of fracture in CP knee crouch as a three-point bending force which fails mechanically on the tension side.
Case presentation
A 15-year-old boy with CP, Gross Motor Function Classification System (GMFCS) Level 2, attended our Gait Laboratory for repeat gait analysis due to a noted deterioration in his walking. His first analysis carried out 2 years earlier had identified bilateral knee crouch of 40° together with a stiff right knee and surgical intervention was recommended (figure 1). This was postponed due to other factors. The repeat gait analysis demonstrated bilateral knee crouch which was unchanged since the previous analysis; however, there was a noticeable lack of shock absorption and return to extension of the right knee, suggestive of extensor disruption. Radiography confirmed an incomplete fracture, greenstick fracture, of the anterior cortex of the right patella (figure 2).
Figure 1.
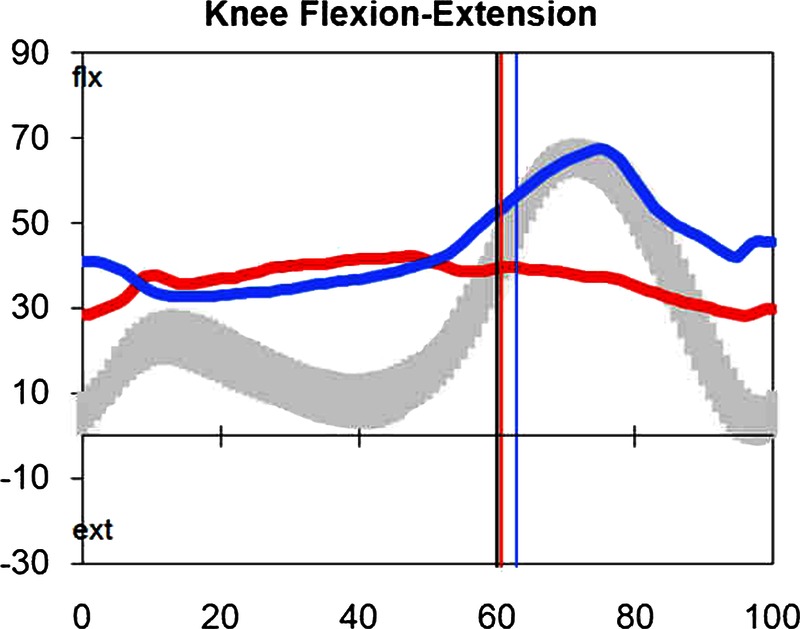
Sagittal kinematics of both knees during a single gait cycle demonstrating midstance bilateral knee crouch (left—blue line and right—red line).
Figure 2.

Lateral radiograph of right knee demonstrating greenstick fracture of the patella.
Treatment
He was treated in a long leg cast for 6 weeks.
Outcome and follow-up
On review the fracture was fully united.
Discussion
Greenstick fractures are caused by a bending force such as when one tries to break a soft branch. The patella is usually fractured by direct impact or avulsion of the quadriceps or the patellar tendon. This case illustrates how a bending force applied to the patella by crouch knee gait can result in mechanical failure of the anterior surface of the patella causing a greenstick fracture without acute trauma. It is significant that the anterior cortex of the patella, the tension cortex, is the site of the greenstick fracture as this confirms that the crouch knee position is the cause. Furthermore, the site of the fracture is at the distal articular limit of the patella where it is unsupported by the femoral condyles. It is this last point of contact with the femoral condyles that acts as a fulcrum therefore making this a pivotal point for bending forces.
Learning points.
A fracture of the patella is a cause of deterioration of gait in diplegic cerebral palsy (CP).
Crouch knee gait generates a great bending force on the patella.
The patellar fracture propagates from the anterior cortex.
A high level of suspicion is required to diagnose these fractures in CP as they may be clinically pain free.
Footnotes
Contributors: YE collected the data for this report. JM performed the gait analysis. DK collated material and prepared the illustrations. TOB supervised the writing of the report.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Maguire JK, Canale ST. Fractures of the patella in children and adolescents. J Pediatr Orthop 1993;2013:567–71 [PubMed] [Google Scholar]
- 2.Carpenter JE, Kasman R, Matthews LS. Fractures of the patella. Instr Course Lect 1994;2013:97–108 [PubMed] [Google Scholar]
- 3.Dai LY, Zhang WM. Fractures of the patella in children. Knee Surg Sports Traumatol Arthrosc 1999;2013:243–5 [DOI] [PubMed] [Google Scholar]
- 4.Ray JM, Hendrix J. Incidence, mechanism of injury, and treatment of fractures of the patella in children. J Trauma 1992;2013:464–7 [DOI] [PubMed] [Google Scholar]
- 5.Grogan DP, Carey TP, Leffers D, et al. Avulsion fractures of the patella. J Pediatr Orthop 1990;2013:721–30 [DOI] [PubMed] [Google Scholar]
- 6.Elhassan Y, O'Sullivan R, Walsh M, O Brien T. Knee extensor disruption in mild diplegic cerebral palsy: a risk for adolescent athletes. BMJ Case Rep 2013. Feb 20;2013. pii: bcr2012008120. doi:10.1136/bcr-2012-008120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.O'Sullivan R, Walsh M, Kiernan D, et al. The knee kinematic pattern associated with disruption of the knee extensor mechanism in ambulant patients with diplegic cerebral palsy. Clin Anat 2010;2013:586–92 [DOI] [PubMed] [Google Scholar]