

Abstract
The bicipitoradial bursa lies at the insertion of the biceps tendon on the radial tuberosity. It is an unusual site for chronic bursitis and most often, results from repetitive mechanical trauma or overuse. Other causes include tuberculosis, immunological complications of the rheumatological disease, for example, psoriatic arthropathy, rheumatoid arthritis and synovial chondromatosis. Unlike ganglion cyst arising from the elbow joint, resection of the bursa through the elbow arthroscopy is not possible as the bursa is not communicated with the joint. We reported a patient with rheumatoid arthritis presenting with bicipitoradial bursitis extended around the radial neck which was successfully resected endoscopically.
Background
The bicipitoradial bursa lies at the insertion of the biceps tendon on the radial tuberosity. The role of this bursa is to reduce friction between the biceps tendon and the tuberosity of the radius. It is an unusual site for chronic bursitis and most often, results from repetitive mechanical trauma or overuse.1–4 Other causes include tuberculosis,5 immunological complications of the rheumatological disease, for example, psoriatic arthropathy1 and rheumatoid arthritis and synovial chondromatosis.6 It can present as swellings in the cubital fossa, symptoms of nerve irritation, for example, median7 and ulnar nerves.2 We reported a patient with rheumatoid arthritis presenting with bicipitoradial bursitis extended around the radial neck which was successfully resected endoscopically.
Case presentation
A 52-year-old woman, a known patient, with rheumatoid arthritis was followed up by a rheumatologist. She was referred to our clinic for the management of persistent right elbow swelling and pain for 1 year despite medical treatment. Clinically, there was swelling over the lateral part of her right upper forearm with local tenderness. The pain was exacerbated by passive forearm pronation or active elbow flexion and forearm supination. There was also tenderness over the radiocapitellar articulation with crepitus. MRI showed diffuse and marked synovial thickening in the elbow joint with erosion over the lateral humeral epicondyle and olecranon process. There was also bicipitoradial bursitis extended around the radial neck. Arthroscopic synovectomy and endoscopic resection of the bicipitoradial bursa were performed.
Treatment
The patient was put on prone position and arthroscopic synovectomy was performed through the proximal medial, anterolateral, posterocentral, posterolateral, soft spot and accessory lateral portals. The patient was then turned to supine position. Biceps tendoscopy was performed through the proximal and distal portals at the lateral side of the biceps tendon. A 4 mm 30° arthroscope was used for this procedure. No arthroscopic pump was used. The proximal portal was just distal to the musculotendinous junction of the biceps and the distal portal was at the level of bicipital tuberosity. The part of inflamed bursa along the biceps tendon was resected endoscopically (figure 1). Under arthroscopic visualisation through the proximal portal, the part of inflamed synovium at the bicipital tubercle was debrided (figure 2). The elbow was flexed and supinated and the synovium anterior to the radial head was removed with the arthroscopic shaver (figure 3). Finally, the synovium deep in between the proximal radius and ulna, and posterior to the radial neck was debrided with the arthroscopic shaver at the previously established accessory lateral portal which was 2 cm distal to the soft spot under arthroscopic visualisation through the distal biceps portal (figure 4). The forearm should be pronated at this time (figure 5). With this approach, the inflamed bicipital bursa surrounding the radial neck (figure 6) was completely resected (figure 7).
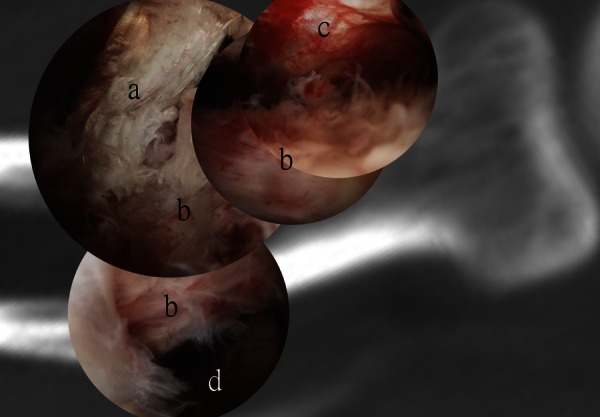
Figure 1.

(A) Biceps tendoscopy was performed through the proximal and distal portals at the lateral side of the biceps tendon. (B and C). The part of inflamed bursa along the biceps tendon was resected endoscopically. (a) Arthroscope (b) arthroscopic shaver (c) distal biceps tendon (d) inflamed synovium around the distal biceps tendon.
Figure 2.

(A–D) Under arthroscopic visualisation through the proximal portal with the arthroscope (a) along the lateral side of the distal biceps tendon (b), the arthroscopic shaver (c) was inserted through the distal portal and the part of inflamed synovium (d) at the bicipital tubercle was debrided. (e) Radius, (f) ulna.
Figure 3.

(A–D) The elbow was flexed and supinated. The arthroscope was inserted through the proximal portal (a) along the lateral side of the distal biceps tendon (b) the arthroscopic shaver (c) was inserted through the distal portal. The synovium anterior to the radial head and deep to the extensor carpi radialis brevis (d) was removed with the arthroscopic shaver. (e) Inflamed synovium; (f) radius, (g) ulna.
Figure 4.

(A–D) The accessory lateral and distal biceps portals are coaxial portals. The arthroscope cannula and trocar (a) can be passed from the distal biceps portal to the accessory lateral portal (b). (c) distal biceps tendon; (d) radius; (e) ulna; (f) anconeus; (g) extensor carpi ulnaris; (h) inflamed synovium.
Figure 5.

(A–D) The synovium deep in between the proximal radius and ulna and that posterior to the radial neck was debrided with the arthroscopic shaver at the accessory lateral portal under arthroscopic visualisation through the distal biceps portal. The forearm was pronated. (a) Arthroscope; (b) arthroscopic shaver; (c) distal biceps tendon; (d) radius; (e) ulna; (f) anconeus; (g) extensor carpi ulnaris; (h) inflamed synovium.
Figure 6.

Arthroscopic view showing the inflamed synovium (a) around the distal biceps tendon (b) and radial neck (c).
Figure 7.
Arthroscopic view after synovectomy showing the distal biceps tendon (a) radial neck (b) spaces anterior (c) and posterior (d) to the radial neck.
Outcome and follow-up
Postoperatively, there was no neurological deficit detected. Her right elbow pain and swelling was subsided and no recurrence was detected during the latest follow-up which was 19 months after the operation.
Discussion
The bicipitoradial bursa is located between the biceps tendon and the radial tuberosity.
The bursa sits between the biceps tendon and the radius when the forearm in supination. As pronation occurs, the radius rotates posteriorly and the bursa is elongated and compressed between the tendon and the radius. This is responsible for painfully restricted pronation.1 On the other hand active biceps action of elbow flexion and forearm supination can also elicit the pain.5 MRI allows accurate diagnosis of bicipitoradial bursitis and study of its relationship with the adjacent structures.8
Isolate bicipioradial bursitis is not common in patients with rheumatoid arthritis; however, it is common in those with synovitis of the elbow.6 Unlike ganglion cyst arising from the elbow joint, resection of the bursa through the elbow arthroscopy is not possible as the bursa is not communicated with the joint.8 9
Open resection with the anterior requires extensive dissection to expose the radial tuberosity and radial neck, which increases the risk of neurovascular injury.10
Various approaches of extra-articular elbow arthroscopy have been developed to treat various pathologies such as lateral epicondylitis, ulnar nerve entrapment, distal biceps tendon rupture,10–12 synovial cysts13 or olecranon bursitis. Many of the extra-articular pathologies were treated through an intra-articular endoscopic approach. The true endoscopic extra-articular technique is proceed through a real anatomical space or inside a space of work created de novo by the surgeon.14 Distal biceps tendoscopy was one of the true endoscopic extra-articular techniques. It has been used for endoscopic repair of distal biceps brachii tendon avulsion,11 15 debridement of partial distal biceps tendon tears16 and synovectomy.14 The portals were located at the lateral side of the tendon in order to avoid damage to the median nerve and brachial artery. Through this technique, the tract of the distal biceps tendon can be approached endoscopically down to the radial tuberosity.10–12 The parts of the inflamed bursa anterior and posterior to the radial neck can be approached through the biceps portals and the accessory lateral portal. The accessory lateral portal which is 2 cm distal to the soft spot portal was used for arthroscopic synovectomy of the radiocapitellar articulation. The distal biceps portal and the accessory lateral portal are coaxial portals and are interchangeable as the visualisation and instrumentation portals. It is important to keep the forearm supinated during synovectomy anterior to the radial neck and pronated during synovectomy posterior to the radial neck. This can keep the posterior interosseous nerve away from the operative site. It is also important to keep the shaver end pointing proximally and towards the radial neck, keep the suction to minimum in order to minimise the risk of neural injury.
Although this endoscopic procedure has the potential advantage of minimally invasive surgery of better cosmetic result and less soft tissue dissection, this case report cannot demonstrate its superiority in terms of results and security compared with the open technique. The difficulty of using this endoscopic technique is related to the vasculonervous structures surrounding the articulation which are directly subject to potential injury. It must be considered as a difficult and sometimes dangerous procedure reserved to experienced elbow arthroscopic surgeons.14
Learning points.
Endoscopic resection of inflamed bicipitoradial bursa extended around the radial neck is a feasible approach.
It has the advantages of minimally invasive surgery.
Details of the operation techniques should be followed strictly in order to minimise the risk of neurovascular injury.
It is technically demanding and should be reserved to experienced elbow arthroscopic surgeons.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Kannangara S, Munidasa D, Kross J, et al. Scintigraphy of cubital bursitis. Clin Nucl Med 2002;2013:348–50 [DOI] [PubMed] [Google Scholar]
- 2.Kijowski R, Tuite M, Sanford M. Magnetic resonance imaging of the elbow. Part II: abnormalities of the ligaments, tendons, and nerves. Skeletal Radiol 2005;2013:1–18 [DOI] [PubMed] [Google Scholar]
- 3.Liessi G, Cesari S, Spaliviero B, et al. The US, CT and MR findings of cubital bursitis: a report of five cases. Skeletal Radiol 1996;2013:471–5 [DOI] [PubMed] [Google Scholar]
- 4.Radunovic G, Vlad V, Micu MC, et al. Ultrasound assessment of the elbow. Med Ultrason 2012;2013:141–6 [PubMed] [Google Scholar]
- 5.Singh AP, Chadha M, Singh AP, et al. Isolated tuberculous biceps tenosynovitis bicipitoradial bursitis: a case report. J Shoulder Elbow Surg 2009;2013:e30–3 [DOI] [PubMed] [Google Scholar]
- 6.Taira H, Yoshida S, Takasita M, et al. Localized cortical bone absorption induced by cubital bursitis in rheumatoid arthritis. Orthopedics 2002;2013:860–1 [DOI] [PubMed] [Google Scholar]
- 7.Karanjia ND, Stiles PJ. Cubital bursitis. J Bone Joint Surg Br 1988;2013:832–3 [DOI] [PubMed] [Google Scholar]
- 8.Skaf AY, Boutin RD, Dantas RW, et al. Bicipitoradial bursitis: MR imaging findings in eight patients and anatomic data from contrast material opacification of bursae followed by routine radiography and MR imaging in cadavers. Radiology 1999;2013:111–16 [DOI] [PubMed] [Google Scholar]
- 9.Feldman MD. Arthroscopic excision of a ganglion cyst from the elbow. Arthroscopy 2000;2013:661–4 [DOI] [PubMed] [Google Scholar]
- 10.Sharma S, MacKay G. Endoscopic repair of distal biceps tendon using an EndoButton. Arthroscopy 2005;2013:897e1–4 [DOI] [PubMed] [Google Scholar]
- 11.Gregory T, Roure P, Fontes D. Repair of distal biceps tendon rupture using a suture anchor: description of a new endoscopic procedure. Am J Sports Med 2009;2013:506–11 [DOI] [PubMed] [Google Scholar]
- 12.Saldua N, Carney J, Dewing C, et al. The effect of drilling angle on posterior interosseous nerve safety during open and endoscopic anterior single-incision repair of the distal biceps tendon. Arthroscopy 2008;2013:305–10 [DOI] [PubMed] [Google Scholar]
- 13.Mileti J, Largacha M, O'Driscoll SW. Radial tunnel syndrome caused by ganglion cyst: treatment by arthroscopic cyst decompression. Arthroscopy 2004; 2013:39–44 [DOI] [PubMed] [Google Scholar]
- 14.Lenoble E. Extra-articular elbow arthroscopy. Chir Main 2006; 2013Suppl 1):S121–30 [PubMed] [Google Scholar]
- 15.Duffiet P, Fontes D. Endoscopic repair of distal biceps brachii tendon avulsion: a new technique. Report of 25 cases. Chir Main 2009;2013:146–52 [DOI] [PubMed] [Google Scholar]
- 16.Bain GI, Johnson LJ, Turner PC. Treatment of partial distal biceps tendon tears. Sports Med Arthrosc Rev 2008;2013:154–61 [DOI] [PubMed] [Google Scholar]