

Description
A 42-year-old man was presented to the emergency service with pain and swelling around the right ankle after a motorcycle accident. No significant pathology was identified in the radiographies taken in the emergency service (figure 1). He was diagnosed with ‘soft tissue injury’. He was discharged with the use of non-steroidal anti-inflammatory drug (NSAID), ice and bandage. He was presented to the orthopaedic clinic 10 days later since his complaints persisted. In the physical examination of the limping patient, tenderness was observed during palpation in the medial tarsal region of the right foot. There was no significant swelling or ecchymosis and sensory-motor examination was normal.
Figure 1.
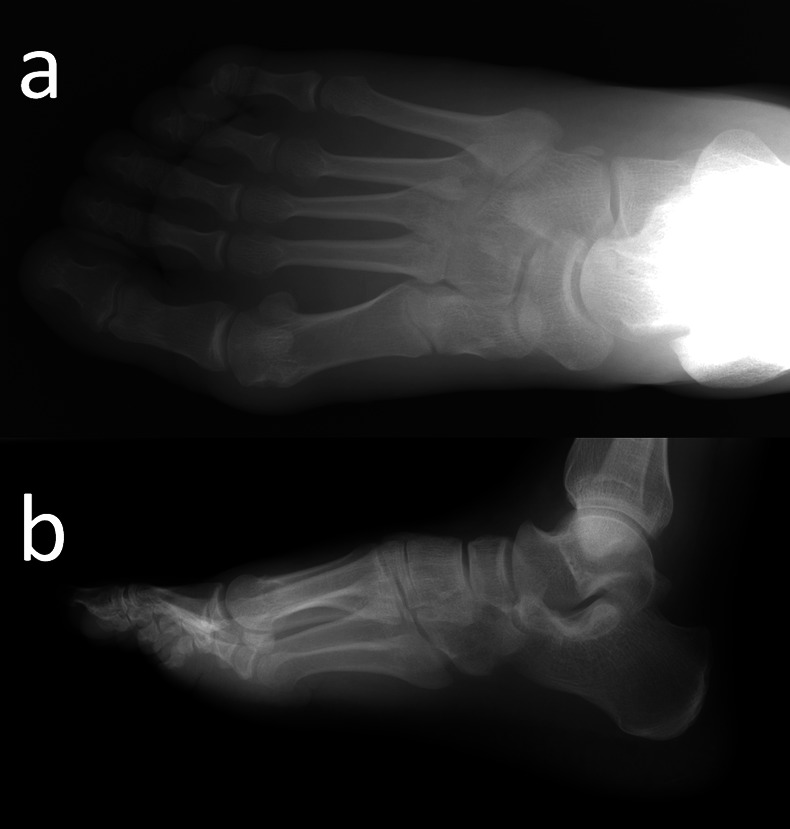
Plain radiographs of the patient's foot.
The MR images revealed an isolated non-displaced fracture in the medial cuneiform bone with an associated oedema (figure 2). A short-leg cast was applied for 20 days. The patient was allowed full weight bearing on the sixth week. He was observed to reach the activity level before injury at the final follow-up 6 months.
Figure 2.
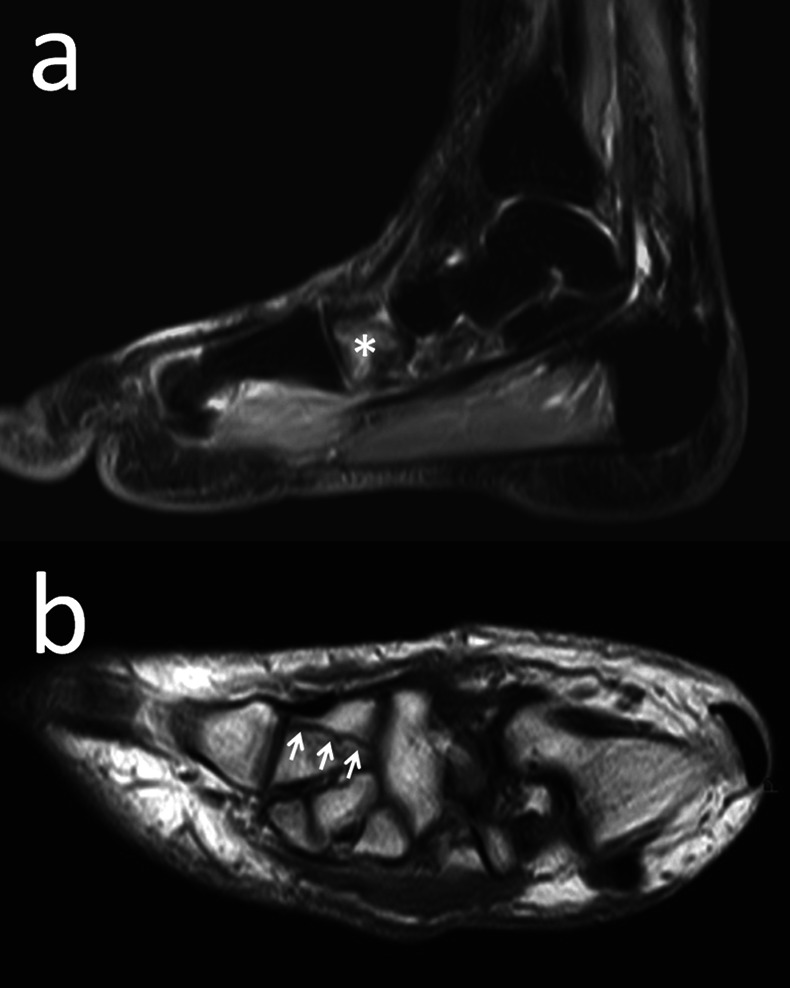
Sagittal short time inversion recovery (STIR) MR image shows oedema in the medial cuneiform bone (asterisk) and coronal T1-weighted MR image shows the fracture line (arrows).
Isolated cuneiform fractures are extremely rare and may be missed at initial admission especially in emergency services because plain radiographs often grossly underestimate the extent of injury. Isolated medial cuneiform fractures are very rare among the mid-tarsal fractures and a total of six cases have been reported in the literature.1
Non-displaced medial cuneiform fracture may be difficult to diagnose and easily be overlooked in the radiographies taken in the emergency service. Direct radiographies should be examined thoroughly, but MRI had better be performed when there is a suspected medial cuneiform fracture; MRI may also reveal an associated tissue or ligament injuries. CT is another diagnostic method which can reveal these fractures and provide reformatted images from different angles.1
In our case, conservative treatment was chosen since the fracture was non-displaced. Positive respond to the treatment without any complication supports the opinion of Guler et al1 for these fractures as being ‘benign nature’.
In this case, the aetiologic reason for the medial cuneiform fracture was a motorcycle accident. In these types of accidents, cuneiform fracture was considered to occur when the medial tarsal region was crushed under the weight of the motorcycle. Swelling and ecchymosis in the tarsal region may provide a clue for diagnosis. However, in our examination of the patient 10 days after the accident, no significant oedema or ecchymosis was present related to the accident.
In the differential diagnosis, bipartite medial cuneiform should be considered.2 These cases may seem similar to cuneiform fracture in the radiological examinations and mis-diagnosed as a fracture. When tenderness is present during palpation on the medial cuneiform bone, stress fractures should also be considered. Medial cuneiform stress fractures caused by repetitive physical loads rather than direct traumas are reported to be more commonly seen among the athletes.3
Learning points.
Isolated medial cuneiform fractures are extremely rare and may be missed at initial admission especially in emergency services because plain radiographs often grossly underestimate the extent of injury.
In context of foot trauma, bipartite medial cuneiform, a normal anatomic variant, may be misdiagnosed as isolated medial cuneiform fracture.
Footnotes
Contributors: All authors have contributed equally in preparing the manuscript research, review, writing and all of them have approved the final draft of the article.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Guler F, Baz AB, Turan A, et al. Isolated medial cuneiform fractures: report of two cases and review of the literature. Foot Ankle Spec 2011;2013:306–9 [DOI] [PubMed] [Google Scholar]
- 2.Elias I, Dheer S, Zoga AC, et al. Magnetic resonance imaging findings in bipartite medial cuneiform—a potential pitfall in diagnosis of midfoot injuries: a case series. J Med Case Reports 2008;2013:272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khan KM, Brukner PD, Bradshaw C. Stress fracture of the medial cuneiform bone in a runner. Clin J Sport Med 1993;2013:262–4 [Google Scholar]