

Abstract
Background
Major depressive disorder (MDD) and posttraumatic stress disorder (PTSD) are commonly comorbid conditions that result in greater severity, chronicity, and impairment compared with either disorder alone. However, previous research has not systematically explored the potential effects of the psychotic subtyping of MDD and comorbid PTSD.
Method
The sample consisted of psychiatric outpatients diagnosed with psychotic MDD with PTSD, psychotic MDD without PTSD, and nonpsychotic MDD with PTSD presenting for clinic intake. Clinical indices of severity, impairment, and history of illness were assessed by trained diagnosticians using the Structured Clinical Interview for DSM-IV supplemented by items from the Schedule for Affective Disorders and Schizophrenia.
Results
In terms of current severity and impairment, the psychotic MDD with PTSD and psychotic MDD only groups were similar to each other, and both tended to be more severe than the nonpsychotic MDD with PTSD group. In terms of history of illness, the psychotic MDD with PTSD group tended to show greater severity and impairment relative to either the psychotic MDD only or nonpsychotic MDD with PTSD groups. Furthermore, the psychotic MDD with PTSD patients had an earlier time to depression onset than patients with either psychotic MDD alone or nonpsychotic MDD with PTSD, which appeared to contribute to the poorer history of illness demonstrated in the former group.
Conclusions
Future research should explore the possibility of a subtype of psychotic depression that is associated with PTSD, resulting in a poorer course of illness. The current findings highlight the need for pharmacological and psychotherapeutic approaches that can be better tailored to psychotic MDD patients with PTSD comorbidity.
Keywords: major depression, posttraumatic stress disorder, psychosis, comorbidity, psychiatric outpatients, onset of illness
Comorbidity in posttraumatic stress disorder (PTSD) is the rule rather than the exception, with major depression being one of the most commonly comorbid diagnoses.1, 2 The National Comorbidity Study found that 48% of individuals with a lifetime history of PTSD also met criteria for major depressive disorder (MDD).3 Conversely, Zimmerman et al.4 reported that 24% of psychiatric outpatients with MDD also had a lifetime diagnosis of PTSD. Some have suggested that the high co-occurrence of these two disorders may be an artifact of the diagnostic criteria.2 However, research has shown that potentially overlapping symptom criteria are unlikely to account for the overdiagnosis of comorbid MDD and PTSD in these patients.5, 6
Comorbid MDD and PTSD negatively impacts the course and severity of either disorder alone. Research has shown that patients with comorbid MDD and PTSD have greater symptom severity,7, 8 higher rates of suicidal behaviors,9 a more chronic course of illness,7 greater functional impairment,8 and a poorer response to treatment.10 Although much is known about the co-occurrence of MDD and PTSD in general, little is know about the potential effects of different depression subtypes on PTSD comorbidity. MDD with psychotic features (or psychotic MDD) is often associated with greater illness severity,11, 12 impairment,12, 13 comorbidity,12, 14 and mortality15 compared to nonpsychotic MDD. Furthermore, psychotic MDD patients tend to have higher rates of illness chronicity,12, 13 relapse,16 and psychiatric hospitalization,12, 14 as well as a poorer response to standard depression treatments such as antidepressants and psychotherapy.17, 18 Psychotic symptoms have also been reported in patients with PTSD without a formal psychotic disorder.19–21 Unfortunately, little is known about patients with psychotic features, MDD, and PTSD more specifically.
In previous reports,22, 23 we found greater severity and over twice the rates of comorbid PTSD in outpatients with psychotic compared with nonpsychotic MDD. This was higher than any other specific comorbid disorder in the psychotic depressed sample. In the present report from the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project, we further explored this relationship by examining the historical course of illness and current severity of psychotic MDD in patients with versus without PTSD to investigate the potential impact of this comorbidity pattern. For comparison purposes, we also contrasted these groups with a sample of patients with nonpsychotic MDD and comorbid PTSD. To our knowledge, this is the first study of its kind to investigate the potential effects of PTSD comorbidity on the course and severity of psychotic MDD. The current study addressed the question of whether PTSD comorbidity affects the severity and course of illness differently within the group of patients with psychotic MDD, and if so, what could account for these differences. We hypothesized that psychotic MDD patients with PTSD would show greater illness severity and poorer functioning compared with patients with either psychotic MDD without PTSD or nonpsychotic MDD with PTSD, and that these differences would be partially accounted for by an earlier age of illness onset in the patients with psychotic MDD with PTSD.
METHOD
Sample
Participants included 2,500 psychiatric patients presenting for treatment at the outpatient practice of the Rhode Island Hospital Department of Psychiatry. The sample consisted of 1,514 females (60.6%) and 986 (39.4%) males, ranging in age from 18 to 85 (M = 38.3, SD = 12.8). The majority of the sample was Caucasian (n = 2,269; 90.8%), followed by African American (n = 112; 4.5%), Hispanic (n = 65; 2.6%), other or mixed ethnicities (n = 35; 1.4%), and Asian (n = 19; 0.8%). Many participants were married (n = 1040; 41.6%), followed by never married (n = 774; 31.0%), divorced (n = 371; 14.8%), separated (n = 141; 5.6%), living as if married (n = 128; 5.1%), and widowed (n = 46; 1.8%). Over half of the sample (n = 1,573; 62.9%) had a high school degree or equivalency, whereas 355 (14.2%) received a 4-year college degree, 328 (13.1%) had a graduate degree/some graduate education, and 244 (9.8%) did not graduate from high school. The most frequent, current Axis I DSM-IV diagnoses were nonpsychotic major depression (n = 1054; 42.2%), social phobia (n = 690; 27.6%), generalized anxiety disorder (n = 428; 17.5%), panic disorder with agoraphobia (n = 339; 13.6%), posttraumatic stress disorder (n = 315; 12.6%), specific phobia (n = 258; 10.3%), alcohol abuse (n = 202; 8.1%), dysthymic disorder (n = 189; 7.6%), and obsessive-compulsive disorder (n = 179; 7.2%). A total of 42.1% (n = 1052) were diagnosed with nonpsychotic MDD and 2.4% (n = 60) with psychotic MDD. Two patients with nonpsychotic MDD diagnoses were excluded from the present analyses because they had a past history of psychotic symptoms that occurred outside the context of a depressive episode. Thus, 5.3% of patients diagnosed with MDD had psychotic features.
Measures
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID).24
The SCID was used for psychiatric diagnosis. The SCID has been shown to have generally high reliability for the major disorders in a variety of samples and experimental designs.25 In addition to psychiatric diagnoses, the following variables assessed during the SCID interview were used in the current study: demographic characteristics, current Global Assessment of Functioning (GAF), age of disorder onset, number of past psychiatric hospitalizations, number of past suicide attempts, and chronic depression status (i.e., current major depressive episode lasting for > 2 years).
Schedule for Affective Disorders and Schizophrenia (SADS).26
The SADS is a semi-structured clinical interview based on the Research Diagnostic Criteria.27 Selected items from the SADS were integrated into the SCID to provide supplemental ratings of symptom severity and impairment. The instrument has been found to have good inter-rater reliability, internal consistency, and test-retest reliability.28 Current (previous month) and past (last 5 years) social functioning ratings were on 7-point Likert scales, ranging from 1 (superior, e.g., had many special friends that he/she saw regularly and frequently and was very close to) to 7 (grossly inadequate, e.g., had practically no social contact). Suicidal ideation (past two weeks) was rated on a 7-point Likert scale, ranging from 1 (not at all) to 7 (very extreme, e.g., suicide attempt with definite attempt to die or potentially medically harmful). Time out of work (past 5 years) was rated by interviewers on a 10-point Likert scale from the SADS, ranging from 0 (not expected to work) to 9 (worked none or practically none due to psychopathology). Patients not expected to work (e.g., students, those on disability for medical reasons) were excluded from this analysis. Chronic work impairment was defined as time out of work > 2 years due to psychiatric illness.
Clinical Global Impression Scale (CGI).29
The CGI is an interviewer-rated measure of illness severity based on a 6-point, anchored scale, ranging from 0 (none) to 5 (extremely ill). In the current study, the CGI was rated specifically for depression severity based on the symptoms endorsed in the SCID, but not other nondepression-related symptoms. The CGI has been found to have good interrater reliability and convergent validity for depression.30
Procedure
Institutional Review Board-approved informed consent was obtained prior to conducting the assessments. New patients to the clinic were offered the opportunity to have a more comprehensive evaluation as part of the clinical-research program, although they were not required to undergo this evaluation. Therefore, not all patients who presented for treatment participated in the study. The varying number of trained diagnostic interviewers available influenced the number of patients who were invited to participate. Also, because one of the goals of the MIDAS project is to develop and study the reliability and validity of self-administered questionnaires, patients with significant cognitive limitations were not included. Nonetheless, as reported elsewhere, patients who did and did not participate in the study were similar in scores on self-administered symptom questionnaires.31 Of particular importance, patients who did and did not participate in the MIDAS project did not differ in their scores on the Psychiatric Diagnostic Screening Questionnaire, a self-administered scale that screens for 13 DSM-IV axis I disorders.32, 33
All participants were evaluated with the full SCID. Diagnosticians had bachelor’s degrees in the social or biological sciences or were doctoral-level clinical psychologists. Diagnosticians were trained for a period of 3 months, which included reviewing written cases, discussing item-by-item administration with the principal investigator (M.Z.), observing at least 5 interviews, and administering 15 to 20 interviews while being observed and supervised. Diagnosticians were then required to demonstrate exact or near-exact inter-rater reliability with a senior diagnostician for 5 consecutive interviews. Diagnosticians received ongoing supervision of interviews via a weekly case conference.
Psychotic MDD was diagnosed according to DSM-IV criteria, which were assessed based on the Mood and Psychotic Modules of the SCID. Furthermore, diagnosticians carefully considered the differential diagnosis of psychotic MDD versus co-occurring conditions that are commonly confused with the disorder (e.g., schizoaffective disorder). Patients with bipolar disorder, schizoaffective disorder, or substance-induced mood disorder were excluded from the current sample. However, those with comorbid posttraumatic stress disorder (PTSD) were included if they also met criteria for psychotic MDD and their psychotic features could not be accounted for by PTSD. Diagnosticians were trained to carefully distinguish between psychotic symptoms and the flashbacks and dissociative experiences often associated with PTSD. Psychotic MDD was diagnosed only when the perceptual disturbances were outside the realm of any trauma-related material.
Inter-rater reliability information was collected over the course of the entire project. From 47 joint-interview reliability evaluations of the SCID, the reliability coefficients of the major Axis I disorders were: major depression κ = 0.91; panic disorder κ = 1.0; social phobia κ = 0.84; obsessive-compulsive disorder κ = 1.0; specific phobia κ = 0.93; generalized anxiety disorder κ = 0.93; posttraumatic stress disorder κ = 0.91; alcohol abuse/dependence κ = 0.64; drug abuse/dependence κ = 0.73; impulse control disorders κ = 1.0; and somatoform disorder κ = 1.0.
Statistical Analyses
First, patients with psychotic MDD and PTSD (psychotic MDD+PTSD), psychotic MDD without PTSD (psychotic MDD only), and nonpsychotic MDD with PTSD (nonpsychotic MDD+PTSD) were compared on demographic and clinical variables using chi square tests or one-way analyses of variance (ANOVAs). If an overall group difference was found, follow-up comparisons were conducted between the psychotic MDD only group and each comparison group separately (psychotic MDD only or nonpsychotic MDD+PTSD). Follow-up 2 x 2 chi square tests or Fisher’s tests were conducted as appropriate. The purpose of testing the overall group difference first was to decrease the total number of statistical analyses conducted and thus reduce Type I error. Cohen’s d statistic (0.20 = small, 0.50 = medium, and 0.80 = large effects)34 or odds ratios35 were also computed for group differences to describe the magnitude of effects. Pearson r correlations were conducted between age of illness onset and the other clinical variables. In addition, time until illness onset among the patient groups was analyzed by means of a Kaplan-Meier survival analysis.36 All tests were two-tailed, and alpha was set at .05. Data were analyzed using SPSS 16.0 for Windows software.
RESULTS
Psychotic MDD+PTSD vs. Psychotic MDD only
According to lifetime psychiatric history as assessed by the SCID, 34 patients were diagnosed with psychotic MDD and comorbid PTSD (psychotic MDD+PTSD) and 26 patients were diagnosed with psychotic MDD without PTSD (psychotic MDD only).1 Chi square tests failed to indicate significant differences between psychotic MDD+PTSD versus psychotic MDD only groups in their rates of delusions (27% vs 39%, respectively; χ2 = .97, df = 1, p = .32) or hallucinations (85% vs 73%, respectively; χ2 = 1.37, df = 1, p = .24).
Table 1 depicts the descriptive and inferential statistics for group comparisons. First, the groups were compared on demographic variables. Results showed no significant differences between psychotic MDD+PTSD and psychotic MDD only patients on any of the demographic variables examined (age, gender, race/ethnicity, education, marital status). In addition, the groups were compared on variables related to symptom severity, functional impairment, and psychiatric history. Follow-up comparisons of significant overall group effects showed that psychotic MDD+PTSD patients had significantly greater numbers of past psychiatric hospitalizations (p = .044; d = .44, CI95% = −0.08–0.97) and suicide attempts (p = .001; d = .85, CI95% = 0.32–1.39) compared with psychotic MDD only patients. Furthermore, psychotic MDD+PTSD patients had significantly higher rates of past social impairment (p = .038; d = 0.46, CI95% = −0.05–0.99) compared with psychotic MDD only patients. The effect for greater chronic work impairment in the psychotic MDD+PTSD group was only approaching statistical significance (p = .059, OR = 3.48, CI95% = 0.92–13.17). No significant differences were found between the groups on other variables: current depression severity, current suicidal ideation, current global functioning, current social functioning, or percentage with chronic depression diagnosis. In summary, these findings suggest that patients with psychotic MDD and comorbid PTSD reported a more severe history of illness compared with patients with psychotic MDD without comorbid PTSD.
Table 1.
Group Comparisons on Demographic and Clinical Variables
| Psychotic MDD+PTSD (n = 34) | Psychotic MDD only (n = 26) | Nonpsychotic MDD+PTSD (n = 263) | Statistical Analysis | |
|---|---|---|---|---|
|
| ||||
| M/% (SD/n) | M/% (SD/n) | M/% (SD/n) | ||
| Demographics | ||||
| Age | 37.2 (12.6) | 36.7 (10.7) | 37.6 (11.1) | F(2, 319)=0.09, p=.913 |
| Female (%) | 79.4 (27) | 65.4 (17) | 73.0 (192) | χ2(2)=1.48, p=.478 |
| Caucasian (%) | 61.8 (21)a | 69.2 (18)a,b | 83.3 (219)b | χ2(2)=10.66, p=.005 |
| College Educated (%) | 11.8 (4) | 15.4 (4) | 25.1 (66) | χ2(2)=3.94, p=.140 |
| Married/Co-Habitating (%) | 41.2 (14) | 46.2 (12) | 46.0 (121) | χ2(2)=0.29, p=.866 |
| Current Severity | ||||
| CGI for Depression | 3.8 (0.5)a | 3.7 (0.5)a | 3.2 (0.6)b | F(2, 320)=25.53, p<.001 |
| Suicidal Ideation | 2.2 (1.9)a | 2.2 (1.4)a | 1.5 (1.4)b | F(2, 319)=5.53, p=.004 |
| Global Assessment of Functioning | 36.8 (10.0)a | 38.5 (9.1)a | 48.2 (7.6)b | F(2, 320)=43.75, p<.001 |
| Social Impairment | 4.0 (1.6)a | 3.9 (1.8)a | 3.3 (1.2)b | F(2, 319)=5.57, p=.004 |
| History of Illness | ||||
| Past Psychiatric Hospitalizations | 1.6 (1.8)a | 0.9 (1.3)b | 0.7 (1.2)b | F(2, 319)=7.02, p=.001 |
| Lifetime Suicide Attempts | 0.5 (0.5)a | 0.2 (0.4)b | 0.2 (0.4)b | F(2, 319)=10.01, p<.001 |
| Past Social Impairment | 3.8 (1.2)a | 3.2 (1.5)b | 3.1 (1.1)b | F(2, 319)=5.21, p=.006 |
| Chronic Work Impairment (%) | 42.3 (11)a | 17.4 (4)a,b | 17.6 (42)b | χ2(2)=9.01, p=.011 |
| Chronic Depressive Disorder (%) | 70.6 (24)a | 53.8 (14)a | 34.2 (90)b | χ2(2)=19.03, p<.001 |
Note. Sample sizes vary slightly due to missing data. MDD = major depressive disorder; PTSD = posttraumatic stress disorder; CGI for Depression = Clinical Global Impressions Severity Scale for Depression.
Means or percentages in the same row that do not share subscripts differ at p < .05.
Psychotic MDD+PTSD vs. Nonpsychotic MDD+PTSD
According to the SCID assessment, 34 patients were diagnosed with psychotic MDD and comorbid PTSD (psychotic MDD+PTSD) and 263 patients were diagnosed with nonpsychotic MDD and comorbid PTSD (nonpsychotic MDD+PTSD). We compared the groups with PTSD on their rates of specific traumatic events. A chi square test showed no significant differences between the psychotic MDD+PTSD versus nonpsychotic MDD+PTSD groups, respectively, on types of traumatic events (χ2 = 6.98, p = .80): serious accident (6% vs 5%), nonsexual assault by someone known (38% vs 29%), nonsexual assault by a stranger (0% vs 3%), sexual assault by someone known (29% vs 33%), sexual assault by a stranger (6% vs 4%), military combat (0% vs 2%), imprisonment (0% vs 0%), life-threatening illness (3% vs 0%), and witnessed a death/violent assault of another person (9% vs 13%).
Psychotic MDD+PTSD patients were significantly more likely to be non-Caucasian compared with nonpsychotic MDD+PTSD patients (p = .003; OR = 3.08, CI95% = 1.44–6.61). No other demographic differences were found between the psychotic MDD+PTSD and nonpsychotic MDD+PTSD groups. Follow-up comparisons of overall significant group effects showed that psychotic MDD+PTSD patients had significantly higher current CGI-depression severity (p < .001; d = 1.17, CI95% = 0.80–1.54) and current suicidal ideation severity (p = .01; d = .41, CI95% = 0.06–0.77), and lower current GAF scores (p < .001; d = 1.28, CI95% = 0.91–1.65) compared with nonpsychotic MDD+PTSD patients. Psychotic MDD+PTSD patients also showed significantly poorer current (p = .004; d = 0.49, CI95% = 0.12–0.85) and past social impairment (p = .001; d = 0.60, CI95% = 0.23–0.96), and were significantly more likely to evidence chronic work impairment (i.e., > 2 years out of work due to psychiatric illness) (p = .003; OR = 3.42, CI95% = 1.47–7.98). Relative to the nonpsychotic MDD+PTSD group, the psychotic MDD+PTSD group also had a greater number of past psychiatric hospitalizations (p < .001; d = 0.58, CI95% = 0.22–0.95) and suicide attempts (p <.001; d = 0.70, CI95% = 0.34–1.06), and was more likely to be diagnosed with chronic depression (i.e., a major depressive episode lasting > 2 years) (p < .001; OR = 4.61, CI95% = 2.11–10.07). In summary, these results showed that patients with psychotic MDD and comorbid PTSD were more severely ill compared with nonpsychotic MDD patients with comorbid PTSD on a variety of clinical indices.
Age of Illness Onset
Table 2 shows the correlations between age of illness onset and other clinical variables. Age of onset of MDD and PTSD were significantly correlated (r = .33, p < .01). Results showed significant inverse relationships between age of MDD onset and past severity and impairment variables (rs = −.13 to −.29), but not current severity indices. For PTSD, the only significant correlation was between age of onset and past social impairment, and was small in magnitude (r = −.12, p < .05). These results suggest that an earlier MDD onset was more likely to be related to a poorer course of illness than an earlier PTSD onset.
Table 2.
Correlations between Age of Illness Onset and Other Clinical Variables
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Major Depressive Disorder age of onset (n = 323) | — | |||||||||
| 2. Posttraumatic Stress Disorder age of onset (n = 297) | .33** | — | ||||||||
| 3. Current Clinical Global Severity for Depression | −.03 | −.03 | — | |||||||
| 4. Current Suicidal Ideation Severity | −.10 | −.11 | .41** | — | ||||||
| 5. Current Global Assessment of Functioning | .08 | −.01 | −.55** | −.46** | — | |||||
| 6. Current Social Impairment Rating | −.09 | −.03 | .21** | .13* | −.24** | — | ||||
| 7. Number of Psychiatric Hospitalizations | −.15** | −.07 | .14** | .18** | −.28** | .10 | — | |||
| 8. Number of Suicide Attempts | −.29** | −.08 | .19** | .28** | −.27** | .16** | .36** | — | ||
| 9. Past Social Impairment Rating | −.25** | −.12* | .15** | .12* | −.16** | .44** | .07 | .17** | — | |
| 10. Chronic Work Impairment (> 2 years) | −.13* | .03 | .22** | .19** | −.32** | .27** | .24** | .37** | .17** | — |
| 11. Chronic Depressive Disorder (> 2 years) | −.18** | −.03 | .18** | .15** | −.28** | .18** | .21** | .12* | .20** | .27** |
Note.
p < .05,
p < .01.
To further explore the impact of illness onset, we conducted survival analyses of the ages until onset for MDD and PTSD. There was a significant difference found in time to MDD onset in the three patient groups (log-rank χ2 = 7.27, df = 2, p = .026). Psychotic MDD+PTSD patients had an earlier time to depression onset than either the nonpsychotic MDD+PTSD (log-rank χ2 = 4.27, p = .039) or psychotic MDD only (log-rank χ2 = 6.95, p = .008) groups. The median time to MDD onset in the psychotic MDD+PTSD group was 14 years (SE = 2.1, CI95% = 9.9–18.1), in the nonpsychotic MDD+PTSD group was 18 years (SE = .9, CI95% = 16.2–19.8), and in the psychotic MDD only group was 24 years (SE = 3.2, CI95% = 17.8–30.2). See Figure 1. In contrast, there was no significant difference in time to PTSD onset in the psychotic MDD+PTSD versus nonpsychotic MDD+PTSD groups (log-rank χ2 = .05, df = 1, p = .82). The median time to PTSD onset in the psychotic MDD+PTSD group was 14 years (SE = 1.7, CI95% = 10.6–17.4) and in the nonpsychotic MDD+PTSD group was 15 years (SE = .8, CI95% = 13.4–16.6).
Figure 1.
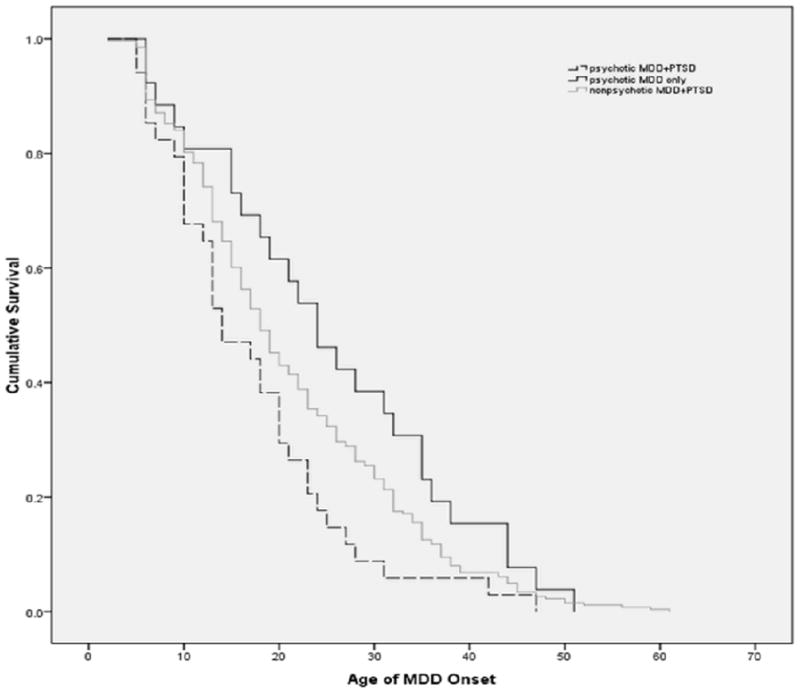
Kaplan-Meier Estimates of survival probabilities for time to onset of Major Depressive Disorder (MDD).
As ages of onset for PTSD versus depression in the psychotic MDD and nonpsychotic MDD groups differed based on the survival analysis results, we conducted paired-samples t-tests to examine this relationship further. The ages of onset of depression versus PTSD were not significantly different in the psychotic MDD+PTSD group (t = 0.38, df = 33, p = .70; PTSD onset M = 18.1, SD = 13.1; MDD onset M = 17.1, SD = 10.0; d = .09, CI95% = −0.40–0.57). In the nonpsychotic MDD+PTSD group, the age of onset of PTSD was significantly earlier than that of depression onset (t = 3.62, df = 262, p < .001; PTSD onset M = 18.0, SD = 12.4; MDD onset M = 21.1, SD = 12.0; d = .25, CI95% = 0.08–0.43). In other words, PTSD and MDD onsets were reported to occur around the same period of time on average for those with psychotic depression. In contrast, PTSD onset was reported to occur significantly earlier than depression onset in the nonpsychotic depressed group.
DISCUSSION
Psychotic depression is associated with even higher rates of psychiatric comorbidity than the nonpsychotic subtype, and this could partially explain the increased severity, impairment, and chronicity often reported in this clinical subgroup.12 PTSD was the most prevalent single comorbid disorder in our psychotic depressed sample, with over half of these patients meeting DSM-IV criteria for the diagnosis.12, 23 Thus, comorbid PTSD was examined in the current study in more detail to investigate its clinical impact on the psychotic subtype of depressed patients. No differences were found between psychotic depressed patients with versus without PTSD in terms of their current symptom severity or impairment at the time of clinic intake. This may have been partly accounted for by the fact that all patients were seeking treatment at the time of the assessment, and thus may have been experiencing elevated levels of distress. In contrast, there were several significant differences between these groups when history of illness variables were examined, which suggested that patients with comorbid psychotic depression and PTSD generally had a poorer course of illness compared with psychotic depressed patients without this comorbidity pattern. This suggests that PTSD comorbidity is related to a poorer course of illness within the psychotic depressed patient population more specifically. Furthermore, results showed that patients with comorbid psychotic depression and PTSD were more severely ill and functionally impaired when compared with patients with comorbid nonpsychotic depression and PTSD. Thus, the prevalence of comorbid PTSD alone in psychotic depressed patients did not appear to account for the findings of overall greater severity and impairment in the psychotic subgroup.
Described in another way, the pattern of differences among the groups depended upon the distinction made between current versus past severity and impairment ratings. For current severity, the psychotic MDD+PTSD and psychotic MDD only groups were similar to each other, and both tended to be more severe than the nonpsychotic MDD+PTSD group. Thus, psychotic depressed patients appeared more severe and impaired, even when compared to a comorbid nonpsychotic depressed group of patients with PTSD. This corresponds with the extant research literature and is consistent with the definition of psychotic depression as a more severe and complicated form of depressive illness.12, 37
However, the interpretation of results changed when past severity and functioning were examined. In this case, the psychotic MDD+PTSD group tended to show greater severity relative to either the psychotic MDD only or nonpsychotic MDD+PTSD groups, with the latter two groups showing more similar levels of severity. To better understand why this might have been the case, we also examined the time to onset of PTSD and depression among these patient groups. Results showed no significant differences in time until onset of PTSD in the psychotic versus nonpsychotic depressed groups. These findings suggest that an earlier onset of PTSD in the psychotic depressed group could not account for the poorer course found in these patients relative to those in the nonpsychotic group. Furthermore, there were no differences in the types of traumatic events experienced between the psychotic and nonpsychotic depressed groups with comorbid PTSD. Thus, the differences were likely due to other clinical factors.
In contrast to the lack of differences found for age of PTSD onset, a significant difference was found for depression onset, with the psychotic MDD+PTSD group reporting the earliest time to onset, followed by the nonpsychotic MDD+PTSD group, and finally the psychotic MDD only group. Thus, patients with psychotic depression and PTSD reported an earlier time to depression onset than patients with either psychotic depression alone or nonpsychotic depression with PTSD, which may help to account for the poorer history of illness demonstrated in the former group. For example, psychotic depressed patients with PTSD were found to have a greater number of suicide attempts and hospitalizations and reported more past social impairment, and a trend toward greater work impairment. We also found that age of depression onset was inversely correlated with a variety of course of illness severity and impairment variables, whereas age of PTSD onset was not, further supporting this interpretation. These findings are consistent with a recent study reporting higher rates of PTSD comorbidity in nonpsychotic depressed patients with a younger age of onset.38
In addition, the timing of onset of PTSD versus depression in the current study appeared to differ between the clinical groups. Patients with psychotic depression reported PTSD and depression onset occurring around the same period of time on average. In contrast, patients with nonpsychotic depression reported PTSD onset occurring significantly earlier than depression onset. These results suggest a potentially different course of illness in psychotic depression with comorbid PTSD, which may further account for the greater severity and impairment identified with this particular comorbidity pattern in the current study.
It should also be noted that patients with psychotic MDD plus PTSD were significantly more likely to be non-Caucasian compared with patients with nonpsychotic MDD plus PTSD. Past research has suggested that African-American and Hispanic patients are more likely to be diagnosed with psychotic MDD compared with Caucasians.14, 39 Given the broader literature showing racial/ethnic differences in primary psychotic disorders, the potential role of culture in the presentation and interpretation of symptoms requires further investigation 40. Furthermore, patients coming from disadvantaged backgrounds may be more likely to possess a history of traumatic life events, making them more vulnerable to PTSD and psychosis.41–43
Possible Explanations for the Co-Occurrence between Psychotic Depression and PTSD
There are several possible explanations for the frequent co-occurrence between psychotic depression and PTSD.2, 44 First, a pre-existing condition such as psychotic depression may relate to the later development of PTSD by increasing the risk of exposure to traumatic events and/or increasing psychobiological vulnerabilities to traumatic events. Alternatively, pre-existing PTSD may increase the risk for the later development of psychotic depression due to its chronicity and associated distress and impairment. Additionally, the co-occurrence between psychotic depression and PTSD may be non-causal and may actually stem from shared genetic and environmental factors. Of course, it is important to point out that these explanations are not necessarily mutually exclusive.
The current findings suggest that the applicability of the scenarios described above also may differ based on the psychotic subtyping of depressed patients. In the current study, psychotic MDD+PTSD patients reported the onset of both disorders around the same time period, which might implicate shared risk factors related to their development and expression. In contrast, the nonpsychotic MDD+PTSD group was more likely to report an earlier onset of PTSD, suggesting that that subsequent development of major depression may have been the result of an increased vulnerability to this disorder (e.g., secondary depression). It is important to keep in mind that the above interpretations are based on the average ages of onset for the groups, and thus simply represent a relative increased probability of occurrence. Within each diagnostic subgroup, there was variability suggesting that different factors may be operating in individuals that can not be fully accounted for by their diagnostic status.
Treatment Implications
The current study suggests the need for further treatment development in patients with psychotic MDD and comorbid PTSD due to its chronic and pernicious course. Regarding psychotic depression, research suggests the efficacy of electroconvulsive therapy (ECT) and antidepressant medications.45–47 Meta-analyses show that ECT has the largest effect sizes, at least in the acute treatment of psychotic depression.47 However, there is a paucity of research documenting the acceptability and efficacy of ECT in treating comorbid depression and PTSD, as these patients typically have been excluded from past clinical trials. Nevertheless, preliminary uncontrolled outcome data suggest the possibility of comparable ECT response in this comorbid group.48 Emerging evidence also suggests that combined pharmacotherapy with atypical antipsychotics and antidepressants may improve outcomes,49 although more research is needed to confirm the costs-benefits of this approach.50
Regarding primary PTSD, a recent report by the Institute of Medicine (IOM)51 concluded that there is insufficient evidence to conclusively determine the efficacy for most currently available pharmacological and psychological treatments for the disorder. Only the efficacy of exposure-based psychotherapies in the treatment of PTSD was deemed to be clearly established based on the committee’s review of 90 clinical trials. Other independent reviews and consensus statements note the potential efficacy of selective serotonin reuptake inhibitors (SSRIs) in the treatment of PTSD.51–54 The evidence to date suggests questionable clinically significant improvements associated with the use of atypical antipsychotic medications in the treatment of PTSD.55 The IOM report further noted significant gaps in the literature on the treatment of comorbid PTSD and other clinical conditions, such as MDD.
Certain forms of psychotherapy can be effective for even severe, nonpsychotic depression56 and primary psychotic disorders including schizophrenia,57 but the evidence for the efficacy of psychotherapy in psychotic depressed patients more specifically is sparse at this point.58 Although there are no studies of psychotherapy for patients with psychotic depression and comorbid PTSD to our knowledge, a recent study demonstrated the preliminary efficacy of CBT for PTSD in patients with severe mental illness. Mueser et al.59 randomly assigned 108 patients with PTSD and other comorbid disorders (schizophrenia, schizoaffective disorder, major depression, bipolar disorder, borderline personality disorder) to either community treatment as usual or CBT for 4–6 months. A total of 21% (n = 23) of patients diagnosed with a primary mood disorder had psychotic features at baseline (Kim T. Mueser, personal communication). Regardless of diagnosis, patients receiving CBT showed significantly greater improvement on a variety of outcomes at post-treatment and through 6-month follow-up, including PTSD and other psychiatric symptoms. This preliminary research suggests that CBT may be a promising adjunctive approach for treating patients with comorbid PTSD and psychotic depression.
Strengths and Limitations
Strengths of the current study included our use of a comprehensive assessment administered by trained diagnosticians with high interrater reliability. To our knowledge, this is the first study of its kind specifically focused on the course of illness in psychotic depression and comorbid PTSD, frequently co-occurring conditions. Several potential study limitations also require consideration. First, our sample of patients with psychotic depression was relatively small, and future research should attempt to replicate the current findings in larger community samples to determine generalizability. Second, age of illness onset was based on retrospective self-reports and may have been subject to memory inaccuracies or recall bias.60 However, Masia et al.61 found that adults were not likely to report the presence of a disorder over 10 years earlier if it did not actually occur. Third, another consideration pertains to the uneven sample sizes among the groups which may have affected statistical power in some analyses. However, analyses produced a fairly consistent pattern of results regardless of the statistical method used (e.g., parametric versus nonparametric tests), and effect sizes appeared clinically significant on most variables (i.e., medium to large in magnitude). Fourth, the current study investigated the impact of the presence of a PTSD diagnosis on the course and severity of illness. However, it is possible that patients in our sample with this diagnosis also differed in their severity of PTSD symptoms. As a measure of PTSD severity specifically was not available, future research should investigate this issue further. Fifth, there is current controversy about the possible presence of psychotic symptoms related to the PTSD syndrome itself as it may be displayed in a certain subgroup of patients.19, 20 To decrease the possible concern about measurement artifact, psychotic features in the current depressed sample were only diagnosed when their content was inconsistent with trauma-related material. Sixth, although our interrater reliability coefficients for major depression and PTSD were very high, we do not have data on interrater reliability in the subsample with psychotic MDD specifically. Finally, it is important to consider the nature of our sample. Patients in the study were predominantly female and Caucasian, similar to other samples of depressed outpatients. More acutely ill patients may not have been willing or able to participate in the comprehensive assessment. As the current study was conducted in a treatment-seeking outpatient sample, caution should be taken when attempting to generalize the current findings to other groups of psychotic depressed patients.
It is important to point out that our sample of patients with psychotic MDD was more likely to report hallucinations than delusions. Some have argued that there may exist important differences between psychotic MDD patients exhibiting primarily delusions versus hallucinations 62. Although early studies of psychotic MDD tended to focus specifically on patients with delusional depression,47 recent versions of the DSM have only required that either delusions or hallucinations be present for the diagnosis. Thus, we believe that it is important to study the official diagnostic criteria to provide more clinically relevant information on these patients. Sometimes patients with hallucinations possess delusional beliefs about their experiences (e.g., believing that a voice is produced by an “evil spirit”), and it is possible our diagnosticians may not have sufficiently probed these areas to elicit further delusional content that could have been coded separately. It will be important for future research to compare and contrast the clinical characteristics of psychotic MDD patients based on their psychotic symptom presentation to determine what affect they have, if any, on symptom presentation and course.
Conclusions and Implications
In conclusion, the earlier onset of depression reported in patients with psychotic MDD and comorbid PTSD may help to account for the poorer course of illness found in this subgroup of patients. These findings suggest that severe depression, PTSD, and psychotic symptoms represent overlapping, but semi-independent problems which appear to contribute to clinical severity and functional impairment in interacting and complex ways. Future research should explore the possibility of a specific subtype of psychotic depression that is associated with PTSD, resulting in a poorer course of illness. The current findings also highlight the need for pharmacological and psychotherapeutic approaches that can be better tailored to psychotic depressed patients with PTSD comorbidity due to their typically chronic and complicated courses of illness.
Acknowledgments
The preparation of this manuscript was supported in part by a grant from the National Institute of Mental Health (MH076937) awarded to Dr. Gaudiano.
Footnotes
Note that the term “psychotic MDD only” is used for convenience only and does not indicate that these patients were free from other comorbidities.
References
- 1.McFarlane AC. Posttraumatic stress disorder: a model of the longitudinal course and the role of risk factors. J Clin Psychiatry. 2000;61 (Suppl 5):15–20. [PubMed] [Google Scholar]
- 2.Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry. 2000;61 (Suppl 7):22–32. [PubMed] [Google Scholar]
- 3.Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1995;52:1048–1060. doi: 10.1001/archpsyc.1995.03950240066012. [DOI] [PubMed] [Google Scholar]
- 4.Zimmerman M, McDermut W, Mattia JI. Frequency of anxiety disorders in psychiatric outpatients with major depressive disorder. Am J Psychiatry. 2000;157:1337–1340. doi: 10.1176/appi.ajp.157.8.1337. [DOI] [PubMed] [Google Scholar]
- 5.Franklin CL, Zimmerman M. Posttraumatic stress disorder and major depressive disorder: investigating the role of overlapping symptoms in diagnostic comorbidity. J Nerv Ment Dis. 2001;189:548–551. doi: 10.1097/00005053-200108000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Blanchard EB, Buckley TC, Hickling EJ, Taylor AE. Posttraumatic stress disorder and comorbid major depression: is the correlation an illusion? J Anxiety Disord. 1998;12:21–37. doi: 10.1016/s0887-6185(97)00047-9. [DOI] [PubMed] [Google Scholar]
- 7.Campbell DG, Felker BL, Liu CF, et al. Prevalence of depression-PTSD comorbidity: implications for clinical practice guidelines and primary care-based interventions. J Gen Intern Med. 2007;22:711–718. doi: 10.1007/s11606-006-0101-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Momartin S, Silove D, Manicavasagar V, Steel Z. Comorbidity of PTSD and depression: associations with trauma exposure, symptom severity and functional impairment in Bosnian refugees resettled in Australia. J Affect Disord. 2004;80:231–238. doi: 10.1016/S0165-0327(03)00131-9. [DOI] [PubMed] [Google Scholar]
- 9.Oquendo MA, Friend JM, Halberstam B, et al. Association of comorbid posttraumatic stress disorder and major depression with greater risk for suicidal behavior. Am J Psychiatry. 2003;160:580–582. doi: 10.1176/appi.ajp.160.3.580. [DOI] [PubMed] [Google Scholar]
- 10.Holtzheimer PE, 3rd, Russo J, Zatzick D, Bundy C, Roy-Byrne PP. The impact of comorbid posttraumatic stress disorder on short-term clinical outcome in hospitalized patients with depression. Am J Psychiatry. 2005;162:970–976. doi: 10.1176/appi.ajp.162.5.970. [DOI] [PubMed] [Google Scholar]
- 11.Lattuada E, Serretti A, Cusin C, Gasperini M, Smeraldi E. Symptomatologic analysis of psychotic and non-psychotic depression. J Affect Disord. 1999;54:183–187. doi: 10.1016/s0165-0327(98)00141-4. [DOI] [PubMed] [Google Scholar]
- 12.Gaudiano BA, Dalrymple KL, Zimmerman M. Prevalence and clinical characteristics of psychotic versus nonpsychotic major depression in a general psychiatric outpatient clinic. Depress Anxiety. doi: 10.1002/da.20470. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Coryell W, Leon A, Winokur G, et al. Importance of psychotic features to long-term course in major depressive disorder. Am J Psychiatry. 1996;153:483–489. doi: 10.1176/ajp.153.4.483. [DOI] [PubMed] [Google Scholar]
- 14.Johnson J, Horwath E, Weissman M. The validity of major depression with psychotic features based on a community sample. Arch Gen Psychiatry. 1991;48:1075–1081. doi: 10.1001/archpsyc.1991.01810360039006. [DOI] [PubMed] [Google Scholar]
- 15.Vythilingam M, Chen J, Bremner JD, Mazure CM, Maciejewski PK, Nelson JC. Psychotic depression and mortality. Am J Psychiatry. 2003;160:574–576. doi: 10.1176/appi.ajp.160.3.574. [DOI] [PubMed] [Google Scholar]
- 16.Aronson T, Shukla S, Gujavarty K, Hoff A, Dibuono M, Kahn E. Relapse in delusional depression: a retrospective study of the course of treatment. Comp Psychiatry. 1988;29:12–21. doi: 10.1016/0010-440x(88)90032-6. [DOI] [PubMed] [Google Scholar]
- 17.Gaudiano BA, Beevers CG, Miller IW. Differential response to combined treatment in patients with psychotic versus nonpsychotic major depression. J Nerv Ment Dis. 2005;193:625–628. doi: 10.1097/01.nmd.0000177791.33649.69. [DOI] [PubMed] [Google Scholar]
- 18.Brown R, Frances A, Kocsis J, Mann J. Psychotic vs. nonpsychotic depression: comparison of treatment response. J Nerv Ment Dis. 1982;170:635–637. doi: 10.1097/00005053-198210000-00008. [DOI] [PubMed] [Google Scholar]
- 19.Lindley SE, Carlson E, Sheikh J. Psychotic symptoms in posttraumatic stress disorder. CNS Spectr. 2000;5:52–57. doi: 10.1017/s1092852900021659. [DOI] [PubMed] [Google Scholar]
- 20.Hamner MB, Frueh BC, Ulmer HG, Arana GW. Psychotic features and illness severity in combat veterans with chronic posttraumatic stress disorder. Biol Psychiatry. 1999;45:846–852. doi: 10.1016/s0006-3223(98)00301-1. [DOI] [PubMed] [Google Scholar]
- 21.David D, Kutcher GS, Jackson EI, Mellman TA. Psychotic symptoms in combat-related posttraumatic stress disorder. J Clin Psychiatry. 1999;60:29–32. doi: 10.4088/jcp.v60n0106. [DOI] [PubMed] [Google Scholar]
- 22.Gaudiano BA, Young D, Chelminski I, Zimmerman M. Depressive symptom profiles and severity patterns in outpatients with psychotic vs nonpsychotic major depression. Compr Psychiatry. 2008;49:421–429. doi: 10.1016/j.comppsych.2008.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zimmerman M, Mattia JI. Psychotic subtyping of major depressive disorder and posttraumatic stress disorder. J Clin Psychiatry. 1999;60:311–314. doi: 10.4088/jcp.v60n0508. [DOI] [PubMed] [Google Scholar]
- 24.First MB, Spitzer RL, Williams JBW, Gibbon M. Structured Clinical Interview for DSM-IV (SCID) Washington, D. C: American Psychiatric Association; 1997. [Google Scholar]
- 25.Segal DL, Hersen M, Van Hasselt VB. Reliability of the Structured Clinical Interview for DSM-III-R: an evaluative review. Compr Psychiatry. 1994;35:316–327. doi: 10.1016/0010-440x(94)90025-6. [DOI] [PubMed] [Google Scholar]
- 26.Spitzer RL, Endicott J. Schedule for Affective Disorders and Schizophrenia (SADS) 3. New York: Biometric Research, New York State Psychiatric Institute; 1977. [Google Scholar]
- 27.Spitzer RL, Endicott J, Robins E. Research diagnostic criteria: rationale and reliability. Arch Gen Psychiatry. 1978;35:773–782. doi: 10.1001/archpsyc.1978.01770300115013. [DOI] [PubMed] [Google Scholar]
- 28.Endicott J, Spitzer RL. A diagnostic interview: the schedule for affective disorders and schizophrenia. Arch Gen Psychiatry. 1978;35:837–844. doi: 10.1001/archpsyc.1978.01770310043002. [DOI] [PubMed] [Google Scholar]
- 29.Guy W. ECDEU Assessment Manual for Psychopharmacology, Revised. Rockville, MD: National Institute of Mental Health; 1976. Clinical Global Impression. [Google Scholar]
- 30.Leon AC, Shear MK, Klerman GL, Portera L, Rosenbaum JF, Goldenberg I. A comparison of symptom determinants of patient and clinician global ratings in patients with panic disorder and depression. J Clin Psychopharmacol. 1993;13:327–331. [PubMed] [Google Scholar]
- 31.Zimmerman M, Mattia JI. Psychiatric diagnosis in clinical practice: is comorbidity being missed? Compr Psychiatry. 1999;40:182–191. doi: 10.1016/s0010-440x(99)90001-9. [DOI] [PubMed] [Google Scholar]
- 32.Zimmerman M, Mattia JI. A self-report scale to help make psychiatric diagnoses: the Psychiatric Diagnostic Screening Questionnaire. Arch Gen Psychiatry. 2001;58:787–794. doi: 10.1001/archpsyc.58.8.787. [DOI] [PubMed] [Google Scholar]
- 33.Zimmerman M, Mattia JI. The Psychiatric Diagnostic Screening Questionnaire: development, reliability and validity. Compr Psychiatry. 2001;42:175–189. doi: 10.1053/comp.2001.23126. [DOI] [PubMed] [Google Scholar]
- 34.Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- 35.Bland JM, Altman DG. Statistics notes. The odds ratio Bmj. 2000;320:1468. doi: 10.1136/bmj.320.7247.1468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kaplan EL, Meier PS. Nonparametric estimation from incomplete observations. Journal of the American Statistical Association. 1958;53:457–481. [Google Scholar]
- 37.Keller J, Schatzberg AF, Maj M. Current issues in the classification of psychotic major depression. Schizophr Bull. 2007;33:877–885. doi: 10.1093/schbul/sbm065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Zisook S, Lesser I, Stewart JW, et al. Effect of age at onset on the course of major depressive disorder. Am J Psychiatry. 2007;164:1539–1546. doi: 10.1176/appi.ajp.2007.06101757. [DOI] [PubMed] [Google Scholar]
- 39.Posternak MA, Zimmerman M. Elevated rates of psychosis among treatment-seeking Hispanic patients with major depression. J Nerv Ment Dis. 2005;193:66–69. doi: 10.1097/01.nmd.0000149222.02563.be. [DOI] [PubMed] [Google Scholar]
- 40.Whaley AL, Geller PA. Ethnic/racial differences in psychiatric disorders: a test of four hypotheses. Ethn Dis. 2003;13:499–512. [PubMed] [Google Scholar]
- 41.Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34:1012–1020. doi: 10.1093/schbul/sbn103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alim TN, Charney DS, Mellman TA. An overview of posttraumatic stress disorder in African Americans. J Clin Psychol. 2006;62:801–813. doi: 10.1002/jclp.20280. [DOI] [PubMed] [Google Scholar]
- 43.Ruef AM, Litz BT, Schlenger WE. Hispanic ethnicity and risk for combat-related posttraumatic stress disorder. Cultur Divers Ethnic Minor Psychol. 2000;6:235–251. doi: 10.1037/1099-9809.6.3.235. [DOI] [PubMed] [Google Scholar]
- 44.Breslau N. Epidemiologic studies of trauma, posttraumatic stress disorder, and other psychiatric disorders. Can J Psychiatry. 2002;47:923–929. doi: 10.1177/070674370204701003. [DOI] [PubMed] [Google Scholar]
- 45.Schatzberg AF. New approaches to managing psychotic depression. J Clin Psychiatry. 2003;64 (Suppl 1):19–23. [PubMed] [Google Scholar]
- 46.Rothschild AJ. Challenges in the treatment of depression with psychotic features. Biol Psychiatry. 2003;53:680–690. doi: 10.1016/s0006-3223(02)01747-x. [DOI] [PubMed] [Google Scholar]
- 47.Vega J, Mortimer A, Tyson P. Somatic treatment of psychotic depression: review and recommendations for practice. J Clin Psychopharm. 2000;20:504–519. doi: 10.1097/00004714-200010000-00003. [DOI] [PubMed] [Google Scholar]
- 48.Watts BV. Electroconvulsive therapy for comorbid major depressive disorder and posttraumatic stress disorder. J ECT. 2007;23:93–95. doi: 10.1097/01.yct.0000264369.38033.34. [DOI] [PubMed] [Google Scholar]
- 49.Rothschild AJ, Williamson DJ, Tohen MF, et al. A double-blind, randomized study of olanzapine and olanzapine/fluoxetine combination for major depression with psychotic features. J Clin Psychopharmacol. 2004;24:365–373. doi: 10.1097/01.jcp.0000130557.08996.7a. [DOI] [PubMed] [Google Scholar]
- 50.Wijkstra J, Lijmer J, Balk FJ, Geddes JR, Nolen WA. Pharmacological treatment for unipolar psychotic depression: Systematic review and meta-analysis. Br J Psychiatry. 2006;188:410–415. doi: 10.1192/bjp.bp.105.010470. [DOI] [PubMed] [Google Scholar]
- 51.IOM. Treatment of PTSD: An assessment of the evidence. Washington DC: National Academies Press; 2007. [Google Scholar]
- 52.Ballenger JC, Davidson JR, Lecrubier Y, et al. Consensus statement on posttraumatic stress disorder from the International Consensus Group on Depression and Anxiety. J Clin Psychiatry. 2000;61 (Suppl 5):60–66. [PubMed] [Google Scholar]
- 53.Brunello N, Davidson JR, Deahl M, et al. Posttraumatic stress disorder: diagnosis and epidemiology, comorbidity and social consequences, biology and treatment. Neuropsychobiology. 2001;43:150–162. doi: 10.1159/000054884. [DOI] [PubMed] [Google Scholar]
- 54.Berlant J. New drug development for post-traumatic stress disorder. Curr Opin Investig Drugs. 2003;4:37–41. [PubMed] [Google Scholar]
- 55.Pae C-U, Lim K-K, Peindl K, et al. The atypical antipsychotic olanzapine and risperidone in the treatment of posttraumatic stress disorder: a meta-analysis of randomized, double-blind, placebo-controlled clinical trials. Int Clin Psychopharmacol. 2008;23:1–8. doi: 10.1097/YIC.0b013e32825ea324. [DOI] [PubMed] [Google Scholar]
- 56.DeRubeis RJ, Hollon SD, Amsterdam JD, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression. Arch Gen Psychiatry. 2005;62:409–416. doi: 10.1001/archpsyc.62.4.409. [DOI] [PubMed] [Google Scholar]
- 57.Gaudiano BA. Cognitive behavior therapies for psychotic disorders: current empirical status and future directions. Clin Psych Sci Pract. 2005;12:33–50. [Google Scholar]
- 58.Gaudiano BA, Miller IW, Herbert JD. The treatment of psychotic major depression: is there a role for adjunctive psychotherapy? Psychother Psychosom. 2007;76:271–277. doi: 10.1159/000104703. [DOI] [PubMed] [Google Scholar]
- 59.Mueser KT, Rosenberg SD, Xie H, et al. A randomized controlled trial of cognitive-behavioral treatment for posttraumatic stress disorder in severe mental illness. J Consult Clin Psychol. 2008;76:259–271. doi: 10.1037/0022-006X.76.2.259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Blaney PH. Affect and memory: a review. Psychol Bull. 1986;99:229–246. [PubMed] [Google Scholar]
- 61.Masia CL, Storch EA, Dent HC, et al. Recall of childhood psychopathology more than 10 years later. J Am Acad Child Adolesc Psychiatry. 2003;42:6–12. doi: 10.1097/00004583-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 62.Carpenter LL, Price LH. Psychotic depression: what is it and how should we treat it? Harv Rev Psychiatry. 2000;8:40–42. [PubMed] [Google Scholar]