

Abstract
Purpose
Reciprocal Imitation Training (RIT) is a naturalistic behavioral intervention that teaches imitation to children with autism within a social-communicative context. RIT has been shown to be effective at teaching spontaneous, generalized object and gesture imitation. In addition, improvements in imitation were associated with increases in verbal imitation and spontaneous language.
Method
This study used a modified multiple-baseline design across four children to examine whether adding gesture imitation training improves the overall rate of appropriate language use in children with ASD who have already been participating in object imitation training.
Results
Three of the four children showed greater improvements in their use of appropriate language after gesture imitation was begun. Further, the children were more likely to use verbal imitation during gesture than object imitation training.
Conclusions
These findings suggest adding gestural imitation training to object imitation training can lead to greater gains in rate of language use than object imitation alone. Implications for both language development and early intervention are discussed.
Children with autism exhibit significant deficits in social communication, including delayed language development and imitation skills (APA, 2000). Imitation deficits have been identified on a variety of tasks, including object (DeMyer et al., 1972; Stone, Ousley, & Littleford, 1997), gesture (DeMyer et al., 1972; Stone et al., 1997; Rogers, Bennetto, McEvoy, & Pennington, 1996), and verbal (Sigman & Ungerer, 1984). Imitation is an early emerging behavior (Meltzoff & Moore, 1977) that appears to play a foundational role in the development of more complex social-communication skills (Rogers & Pennington, 1991; Uzgiris, 1981). In particular, a growing body of literature suggests that imitation skills are associated with language development in typically developing children (Bates et al., 1988) and children with autism (Stone et al., 1997; Stone & Yoder, 2005). For example, imitation skills were strongly predictive of vocabulary size in young children with autism, both concurrently and six months later (Stone et al., 1997). Further, Stone and Yoder (2005) found that after controlling for initial language level, imitation skills, along with hours of speech therapy, were the best predictor of language skills two years later in a sample of young children with autism. Similarly, Toth, Munson, Meltzoff, and Dawson (2006) reported that immediate imitation skills were correlated with concurrent language ability in preschoolers with autism and deferred imitation was correlated with language gains over two years. Carpenter, Pennington, and Rogers (2002) also found an association between immediate imitation of arbitrary actions and referential language skills in young children with autism, both of which emerged before joint attention skills. This finding led them to propose that, unlike typically developing children, children with autism may rely more heavily on imitation than joint attention for language acquisition. Taken together, these data suggest that, particularly for children with autism, imitation skills play a foundational role in the development of spoken language.
These findings have highlighted the importance of interventions which can teach imitation skills to young children with autism (e.g., Ingersoll, 2008; Rogers, 1999). Reciprocal Imitation Training (RIT) is a naturalistic behavioral intervention that has been found to be effective for teaching object and gesture imitation during play in young children with autism. In one study, Ingersoll and Schreibman (2006) used a multiple-baseline design across five young children with autism to examine the efficacy of RIT for teaching object imitation. All five children improved their ability to imitate actions with objects. In addition, they also improved their verbal imitation skills, despite the fact that the intervention did not directly target verbal imitation. In a second study using a multiple-baseline design, Ingersoll et al. (2007) taught five different young children with autism to imitate gestures during play. Again, all children increased their ability to imitate gestures, as well as their verbal imitation. Further, in both studies, there was some evidence that the interventions also improved non-imitative language skills. For example, three of the five children in both studies also improved their use of spontaneous language.
Taken together, these studies suggest that teaching nonverbal imitation skills via RIT may be an effective method for increasing language skills in children with autism. However, the degree to which the specific nonverbal imitative behavior targeted (i.e., object versus gesture) affects language use is unclear. Previous data suggest that children in both interventions made gains in language skills; however, it might be expected that teaching gesture imitation may be particularly important for supporting language development. For example, in typical infants, natural gestures generally precede verbal language, while serving many of the same communicative functions (Acredolo & Goodwyn, 1990; Özçalişkan & Goldin-Meadow, 2005). Further, parents routinely interpret these gestures as if they were words (Acredolo & Goodwyn, 1990). Thus, teaching gesture imitation may lead to additional gains in language skills, either directly, by providing increased cognitive resources (Özçalişkan & Goldin-Meadow, 2005), or indirectly, by recruiting more parental linguistic input (Yoder, Kim, Warren, & Gazdag, 1994).
The goal of this study was to examine the effects of RIT for object and gesture imitation on language behavior in four young children with ASD. The first question examined whether adding gesture imitation training improved the overall rate of appropriate language use in children with ASD who were already participating in object imitation training. The second question examined whether children were more likely to engage in verbal imitation during object or gesture imitation training using RIT.
Method
Participants
Four children (three boys) with an autism spectrum disorder participated in this study. Participants were diagnosed by an outside professional with an expertise in autism using APA criteria (APA, 2000). Diagnoses were verified using the Autism Diagnostic Observation Schedule-Generic (ADOS-G; Lord et al., 2000). The children ranged in age from 35 to 47 months, with a cognitive age equivalent of 22 to 30 months as measured on the Bayley Scales of Infant Development, 3rd Ed. (Bayley, 2006), and a language age equivalent of 18 to 21 on the Preschool Language Scales, 4th Edition (Zimmerman, Steiner, & Pond, 2002). Three of the children were White and one child was Hispanic. All children’s families were in the top two social strata on the Hollingshead Four Factor Index (Hollingshead, 1975). The children received outside services from public preschool programs and private therapy throughout the study. All children exhibited deficits in spontaneous imitation, as determined by parent report, and a score of less than 40% on the Unstructured Imitation Assessment (see below). Parents gave informed consent for their children to participate in the study (see Table 1 for Participant Characteristics).
Table 1.
Participant Characteristics
| Participant | Chronological Age (Mos.) | Cognitive Agea (Mos.) | Language Ageb (Mos.) | Ethnicity | Socio-economic Statusc | Hours of Outside Therapy per week |
|---|---|---|---|---|---|---|
| Richard | 40 | 30 | 21 | White | 48 | 25.5 |
| Lenore | 35 | 22 | 18 | Hispanic | 60 | 18 |
| Donald | 37 | 27 | 18 | White | 63 | 16.5 |
| Jared | 41 | 24 | 21 | White | 53 | 9.25 |
Bayley Scales of Infant Development, 3rd Edition
Preschool Language Scales, 4th Edition
Hollingshead Four Factor Index
Design & Procedure
This investigation was conducted as part of a larger randomized controlled trial testing the efficacy of RIT for teaching imitation skills in young children with ASD. As part of this study, all participants received training in object and gesture imitation using RIT one hour per day, three days a week for 10 weeks; each one-hour visit was broken into three 20-minutes sessions. Given the design of the larger study, we did not collect ongoing baseline data; however, two aspects of the treatment implementation allowed us to examine our research questions using single-subject design methodology. First, all participants received training in object imitation first (e.g., all three sessions per day targeted object imitation) and the addition of gesture imitation training was staggered across participants, so that Richard received it after 6 days of treatment, Lenore after 10 days, Donald after 11 days, and Jared after 18 days. Thus, we were able to examine whether the addition of gesture imitation improved language behavior above and beyond object imitation training using a modified multiple-baseline design with object imitation training serving as the baseline (Hersen & Barlow, 1976). Second, once gesture imitation was added, object and gesture imitation training were alternated every session, such that each child received one or two sessions of each condition per day. This aspect of the design allowed us to examine whether the children were more likely to use verbal imitation during object or gesture imitation training using a rapidly alternating treatments design.
Setting and Materials
Outcome assessments were conducted in a large sitting room with a small table and couch. All treatments sessions were conducted in a small treatment room with mounted cameras. Five pairs of identical play materials (one for the child and one for the therapist) were used in each treatment session. Toys were selected for each child based on his or her interests and included a wide variety of developmentally appropriate toys, such as vehicles, dolls/figurines, balls, slinkies, playdoh, musical instruments, and art materials. Toys were varied each 20-minute session, totaling 15 pairs of play materials per day. Assessment materials were not used during treatment.
Treatment
RIT uses several naturalistic techniques to teach imitation skills during play. To promote reciprocity, the therapist contingently imitated the child’s verbal and nonverbal behavior, described the child’s actions using simplified language, and expanded the child’s utterances (Warren, Yoder, Gazdag, & Kim, 1993). For example, if the child was rolling a car back and forth on the ground, the therapist would role another car back and forth, while saying “Roll car. Car is rolling.” If the child said, “Roll car,” the therapist would respond by saying, “Roll the car” or “Roll car fast.” To teach imitation, the therapist modeled an action, either with an object or a gesture, once a minute on average. Actions were modeled up to three times, paired with a distinct verbal marker describing the action. If the child did not imitate the action within 10 seconds of the third model, the therapist physically prompted the child to complete the action. The therapist praised the child for imitation and returned to using contingent imitation and describing the child’s play. Language behavior, including verbal imitation, was not prompted or systematically reinforced.
Object Imitation Training
The therapist taught object imitation by modeling an action with the duplicate of the toy the child was currently attending to. For example, if the child was spinning the wheels of a car, the therapist might model pushing a second car, while saying “Vroom, vroom” or might model opening the door on the car, while saying, “Open door.”
Gesture Imitation Training
The therapist taught gesture imitation by modeling a gesture related to the child’s play. For example, if the child was spinning the wheels of the car, the therapist might model a spinning gesture (e.g., spinning finger in a circle), while saying “Spin, spin” or might model a driving gesture (e.g., pantomiming turning the wheel), while saying “It’s a car.” All modeled gestures involved the upper extremities to ensure that the therapist could physically prompt the correct response when necessary.
The goal of RIT is for the child to be able to imitate the majority of actions of a play partner rather than to be able to accurately produce specific actions in response to a model (Ingersoll & Schreibman, 2006). Therefore, rather than teaching the imitation of specific actions to criterion, multiple actions were targeted concurrently based on the context of the child’s play. Modeled actions were varied across toys to avoid associating a specific action with a specific toy. Further, although the verbal marker was kept consistent across the three presentations of the action within the trial, it was varied across trials so that it did not become associated with a specific toy or action. Finally, good attempts at imitation were also reinforced, even if the exact model was not reproduced. See Ingersoll (2008) for a more detailed description of the intervention.
Therapist Training
All therapy was conducted by the authors, a masters’ level clinician, and trained graduate and undergraduate research assistants. Prior to working with the children, therapists were trained to 90% correct implementation of the intervention during role play sessions with the lead therapist who was a masters’ level clinician. Therapists received in-session coaching and feedback from the lead therapist during their first few sessions with the participants, until they were able to maintain 90% fidelity across three sessions (i.e., average rating across RIT components of at least “4” for each session) as rated by the lead therapist. Each child worked with at least three different therapists throughout treatment to promote generalization and to rule out therapist effects. To ensure correct implementation of the procedure, fidelity of implementation was scored in vivo for all sessions by a trained therapist who observed and recorded the session using a rating scale developed for this study. If therapists fell below an average fidelity rating of 4 for any session, they received additional coaching from the lead therapist. Fidelity of implementation was high across sessions (mean=4.8 out of 5; range=3.6–5.0). See Appendix A for the Fidelity of Implementation rating form.
Appendix A.
RIT Fidelity of Implementation Rating Form
| RIT Component | Low Fidelity 1 |
2 | 3 | 4 | High Fidelity 5 |
|---|---|---|---|---|---|
|
Contingent Imitation Imitate child’s toy play, gestures, and vocalizations. |
Therapist does not imitate the child’s gestures, vocalizations, and toy play | Therapist imitates a few of the child’s gestures, vocalizations, and toy play, but misses the majority of opportunities | Therapist imitates the child’s gestures, vocalizations, and toy play up to 50% of the time, but misses many opportunities | Therapist imitates more than 50% of the child’s gestures, vocalizations, and toy play when the child is appropriately engaged, but misses opportunities | Therapist imitates almost all of the child’s gestures, vocalizations, and toy play throughout the session when the child is appropriately engaged. |
|
Linguistic Mapping Use simplified, repetitive language around child’s attentional focus. |
Therapist does not use simplified language around the child’s attentional focus, language is too complex, or therapist does not use any language. | Therapist uses simplified language around the child’s attentional focus during some of the session, but misses the majority of opportunities or majority of language is too complex. | Therapist uses simplified language around the child’s attentional focus up to 50% of the time, but misses many opportunities. | Therapist uses simplified language around the child’s attentional focus for more than 50% of the session, but misses opportunities or language is not appropriate for child’s level of language. | Therapist uses simplified language around the child’s attentional focus throughout the session. Almost all of the therapist’s language is appropriate for child’s language level. |
|
Model Model actions around child’s focus of interest. |
Therapist models actions that are inappropriate for child’s level/interest or does not recruit child’s attention. | Therapist models some actions that are appropriate for child’s level/interest but also many that are not or often fails to recruit the child’s attention. | Therapist models some actions that are appropriate for child’s level/interest and recruits child’s attention some of the time. | Therapist models actions that are appropriate for child’s level/interest more than 50% of the time and recruits child’s attention the majority of the time. | Therapist models actions that are very appropriate for child’s level/interest and recruits child’s attention. |
|
Pacing Model an action once a minute, on average. Adjust rate when necessary to keep child engaged. |
Therapist models actions at a significantly lower or higher rate throughout session. Pacing significantly disrupts child’s engagement or learning. | Therapist models actions at a significantly lower or higher rate throughout session. Pacing somewhat disrupts child’s engagement or learning. | Therapist models actions at a somewhat lower or higher rate throughout session. Pacing does not significantly disrupt child’s engagement or learning. | Therapist models at an appropriate rate for some, but not all of the session. Pacing does not significantly disrupt child’s engagement or learning. | Therapist models actions at an appropriate rate throughout session. Pacing is appropriate for keeping child engaged and learning. Therapist models at least 10 trials, and no more than 20. |
|
Prompt Physically prompt child to imitate after 3 presentations of action. |
Therapist does not physically prompt child to imitate action after presenting the action 3 times. | Therapist prompts child to complete action after third trial a minority of the time, but misses many opportunities or prompting often does not result in imitation (e.g., child switches activities without imitating). | Therapist prompts child to complete action after third trial up to 50% of the time, but misses many opportunities or prompting does not result in imitation (e.g., child switches activities without imitating). | Therapist prompts child to complete action after third trial the majority of the time, but misses opportunities or prompting occasionally does not result in imitation (e.g., child switches activities without imitating). | Therapist consistently prompts child to complete action after third trial if child has not spontaneously imitated. Once therapist begins a trial, therapist follows through such that the trial ends in imitation. |
|
Praise Animatedly praise child’s spontaneous or prompted imitation. |
Therapist does not praise child’s spontaneous or prompted imitation or consistently praises incorrect responses. | Therapist praises a minority of the child’s spontaneous and prompted imitations, but misses the majority of opportunities or praises multiple responses. | Therapist praises some of the child’s spontaneous and prompted imitations, but misses many opportunities or praises incorrect responses. | Therapist praises the majority of the child’s spontaneous and prompted imitation, but misses some opportunities or praise is provide for an incorrect response. | Therapist praises all of the child’s spontaneous and prompted imitation throughout the session. Praise is withheld for incorrect responding. |
Dependent Measures
Session Data
The first 10 minutes of the second session of each day was videotaped and scored for appropriate language and verbal imitation using the Noldus Observer software (Noldus, 1991). Appropriate language was defined as any language that the child used for the purpose of communicating with the therapist. It could be in response to the therapist’s communication or spontaneously initiated. To be coded as appropriate, the language had to be in context and meaningful. Appropriate language was scored using frequency counts and then converted to an overall rate per minute. Verbal imitation was defined as imitation within 10 seconds of all or a portion of the therapist’s verbal marker during object or gesture imitation modeling. Verbal imitation was scored as a percent of opportunities, with opportunities defined as the number of verbal markers presented by the therapist in conjunction with object and gestures models. Scoring was completed by undergraduate research assistants trained to 80% accuracy on practice tapes. Inter-rater reliability was obtained for 33% of the observations using Pearson’s product-moment correlations (Hartman, 1977). Pearson’s product-moment correlations were chosen over percent agreement since, unlike percent agreement, Pearson’s r is independent of the specific rate of behavior. A potential shortcoming of Pearson’s r is the possibility that one observer may consistently code more of the behavior than the other observer. To examine this possibility, we conducted paired t-tests of the differences between correlated scores. None of these observations was found to be significantly different (all p-values <.05), indicating no systematic observer bias (Hartmann, 1977). Reliability for each participant was acceptable for appropriate language (Richard=.81; Lenore=.96; Donald=.97; Jared=.96) and verbal imitation (Richard=.97; Lenore=.99; Donald=.96; Jared=.95). The primary rater also worked as a therapist with the children in this study; however, the reliability rater did not.
Assessment Data
All assessments were administered at pretreatment, post-treatment, and at a two-month follow-up. Two measures were used to examine changes in nonverbal imitation skills, the target of the intervention. The Motor Imitation Scale (MIS; Stone et al., 1997) measured the child’s ability to imitate in a structured setting. It included 8 object and 8 gesture imitation tasks. Participants were seated at table at a 90 degree angle from the examiner. Before the task began, the examiner said, “I have some toys to play with. Watch closely and do what I do.” Before each trial, the examiner said, “Watch me” and then modeled the action. The toy was then presented to the child for 10-seconds and the child was instructed, “You do it.” For each item, the child had three opportunities to imitate the examiner’s action. Responses were scored on a 3-point scale: a “2” was recorded if the child produced exact imitation, a “1” was recorded if the child produced an emerging response (e.g., the child attempted to manipulate the toy in the correct manner, but failed to complete the act exactly as modeled), and a “0” was recorded if the child failed to imitate. For each action, only the best trial was recorded. Overall imitation scores could range from 0–32. Reliability was calculated by two independent observers on 25% of observations. Cohen’s Kappa collapsed across MIS items and observations was .93.
The Unstructured Imitation Assessment (UIA) was developed for this project to measure the child’s ability to imitate spontaneously during unstructured play. The child was seated on floor with examiner with two pairs of each toy freely available. Before the task began, the examiner said, “I have some toys to play with. We can play together.” Then, the examiner imitated all of the child’s play with a duplicate toy for 2 minutes. After the initial contingent imitation period, the examiner began to model actions with toys. Before each trial, the examiner said “Watch me” and then modeled an action and its verbal marker followed by a 10-second response period. Each action was modeled three times regardless of the child’s subsequent behavior. After the third model, the examiner returned to imitating the child for 45 seconds before presenting a new model. Toys were presented in random order; however, the examiner refrained from modeling an action with the toy that the child was currently engaged with. The child’s response was scored similarly to the MIS, with a “0” for no response or an incorrect response, “1” for an emerging response, and “2” for a full imitative response. Scores could range from 0–40. Reliability was calculated by two independent observers on 25% of observations. Cohen’s Kappa collapsed across UIA items and observations was .84. See Table 2 for sample items from the MIS and UIA.
Table 2.
Sample Items from the Imitation Assessments
| Motor Imitation Scale | Unstructured Imitation Assessment | |
|---|---|---|
| Object Imitation | Drive car across table. | Put slinky on nose. “Look at my nose!” |
| Tap spoon on table. | Hit tambourine with rattle. “Ta da!” | |
| Gesture Imitation | Pat cheek. | Place hands on cheeks. “Oh no!” |
| Pull on earlobe. | Hold both arms out at sides. “It’s a plane.” |
Two measures were used to assess changes in the children’s language skills from pre- to post-treatment, as well as at a two-month follow-up. The children’s primary caregivers completed the MacArthur-Bates Communicative Development Inventory (MCDI; Fenson et al., 1993) to determine child vocabulary size. Children who used primarily single words (Lenore and Donald) were given the Words and Gestures form. Children who used phrase speech (Richard and Jared) were given the Words and Sentences form. In addition, the UIA was scored for appropriate language using the same scoring criteria as the session data. The UIA was conducted in a separate testing room, included toys not used during treatment sessions, and did not involve prompting or reinforcement. Thus, child language use during the UIA provided a measure of generalization and maintenance of skill over time.
Results
Language Skills
Session Data
We examined whether the children increased their rate of appropriate language once gesture imitation was added to the intervention. Three of the four children (Lenore, Donald, and Jared) showed a stable pattern of language use during the object imitation training phase, followed by an ascending pattern of language use concurrent with the onset of gesture imitation training. The fourth child, Richard, showed a less consistent pattern of response. During the object imitation training phase, Richard showed a decrease in his language use over time. With the onset of gesture imitation training, he showed an increase in his rate of language use, returning to a rate similar to his initial performance. However, half-way through treatment, Richard’s family went on vacation and when they returned, Richard was intermittently sick for several weeks. During this time period, Richard’s performance in treatment sessions declined significantly, both in terms of his language use as well as his nonverbal imitation performance. Towards the end of treatment, his behavior improved; however, his language use remained lower than his earlier performance (see Figure 1).
Figure 1.

Rate of appropriate language use during treatment sessions.
We next examined whether the children were more likely to use verbal imitation in the object or gesture imitation conditions once they began alternating. Richard showed an immediate difference in his percent of verbal imitation between conditions, with a substantially higher percent of verbal markers imitated during the gesture sessions. Half way through treatment, he exhibited a decrease in his percentage of verbal imitation in the gesture sessions, such that by the end of treatment, he was no longer discriminating between conditions. This decrease in verbal imitation corresponded with his family’s vacation and his illness. In contrast, Lenore, Donald, and Jared did not show an initial difference in the percent of verbal markers imitated across the two conditions. However, by the end of treatment, they showed a higher percent of verbal imitation during the gesture than object sessions. Donald and Jared, and to a lesser extent Lenore, also showed an increase in their use of verbal imitation in the object imitation sessions over time; however, their use of verbal imitation in the gesture sessions increased at a greater rate (see Figure 2). To supplement visual analysis of the data, Wilcoxon signed-rank tests were used to compare verbal imitation in the object and gesture conditions for each children. Given our a priori assumptions, one-tailed tests were used. This analysis suggested that Richard (Z=1.88, p=.03), Lenore (Z=2.07, p=.02), and Donald (Z=2.38, p=.01) imitated a higher percentage of verbal markers in the gesture than object condition, while Jared (Z=.84, n.s.) did not show a significant difference between conditions.
Figure 2.
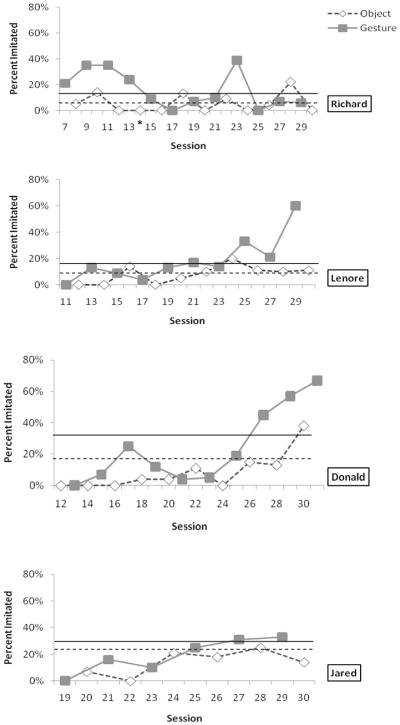
Percent of verbal markers imitated during object and gesture imitation sessions. The dashed horizontal line represents the average performance across object sessions and solid horizontal line represents average performance across gesture sessions.
Assessment Data
All children increased their rate of appropriate language during the UIA from pre- to post-treatment. This rate remained above pretreatment rates at the two-month follow-up for three of the four participants. Further, all children exhibited an increase in their vocabulary from pre- to post-treatment, and again at follow-up, as measured by the MCDI (see Table 4).
Table 4.
Participant’s Imitation Performance at Pre, Post, and Follow-up
| Motor Imitation Scale | Unstructured Imitation Scale | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Participant | Pre | Post | Follow-up | Pre | Post | Follow-up |
| Richard | 30 | 32 | 32 | 14 | 19 | 26 |
| Lenore | 6 | 24 | 24 | 4 | 15 | 18 |
| Donald | 2 | 31 | 24 | 2 | 18 | 7 |
| Jared | 17 | 27 | 19 | 7 | 13 | 9 |
| Average (SD) | 13.75 (12.55) | 28.50 (3.70) | 24.75 (5.38) | 6.75 (5.25) | 16.25 (2.75) | 15.00 (8.76) |
Nonverbal Imitation Skills
All children made improvements in their object and gesture imitation skills on both the MIS and UIA from pre- to post-treatment. Performance maintained or continued to improve at the two-month follow-up for three of the four children (See Table 3). Although indicative of improvement in imitation skills over time, these results cannot be attributed to treatment because there were no experimental controls for these measures.
Table 3.
Participant’s Language Performance at Pre, Post, and Follow-up
| Rate per minute of Appropriate Language (UIA) | Expressive Vocabulary Size (MCDI) | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Participant | Pre | Post | Follow-up | Pre | Post | Follow-up |
| Richard | 1.71 | 2.13 | 1.81 | 303b | 427 | 482 |
| Lenore | .98 | 1.38 | 2.51 | 102a | 157 | 181 |
| Donald | .25 | 1.16 | .79 | 80a | 99 | 142 |
| Jared | .43 | 1.34 | .45 | 347b | 464 | 497 |
| Average (SD) | .84 (.66) | 1.50 (.43) | 1.39 (.94) | 208 (137) | 287 (185) | 326 (190) |
Words and Gestures form
Words and Sentences form
Discussion
The results indicate that adding gestural imitation training to object imitation training can lead to greater gains in rate of language use than object imitation alone in young children with ASD. Three of the four children exhibited an increase in their rate of language use once gesture imitation was added. Further, all children were more likely to imitate the verbal marker paired with the modeled action in the gesture than object imitation sessions, once these sessions began alternating. Finally, all children exhibited generalized improvements in language skills that maintained after the intervention was completed on both an observation assessment as well as parent report. Thus, the fact that the rate of language use increased for three of the children with the onset of gesture imitation training suggests that teaching gesture imitation skills may be associated with improved language use.
There are several reasons why gesture imitation training may have improved language use above and beyond object imitation training. One possibility is that the children were more likely to learn verbal imitation through gesture than object imitation training. This possibility is supported by our data which indicate the children were more likely to imitate the verbal marker in the gesture sessions than object session. However, why gesture imitation promotes verbal imitation more than object imitation training is unclear. To this end, we offer several potential explanations. First, gestures are inherently communicative, whereas object play is not necessarily communicative. Thus, when the therapist modeled a gesture the children may have attended more to the verbal marker which accompanied it because the gesture and the verbal marker were perceived as a joint communicative act. Another possibility is that because the gestures modeled were more abstract (i.e., representational) than the actions with objects, the children may have attended more to the verbal marker paired with the gesture in an attempt to understand the therapist’s action. It is also possible that the children may have become overly focused on the therapist’s object during object modeling, attending less to the therapist’s other behavior (i.e., verbal marker). In each of these cases, increased attention to the verbal marker in gesture sessions may have led to more verbal imitation. Another possibility is that because gestures are more difficult for children with autism to imitate (DeMyer et al., 1972; Stone et al., 1997), the children may have been less sure of the expected response in the gesture imitation sessions. This led them to use another behavior that had been reinforced in the past (verbal imitation). Finally, it is possible that the therapists were more inclined to model gestures in the children’s line of sight than objects. This may have improved the children’s joint attention during gesture trials, leading to more verbal imitation (Clibbens, Powell, & Atkinson, 2002).
Interestingly, the improvement in rate of language use was not limited to the gesture imitation sessions. Rather, the children exhibited an overall change in trajectory across both gesture and object sessions once gesture training was introduced. This finding suggests that the benefits of gesture imitation training were not due exclusively to enhanced attention to the verbal model or performance of a previously reinforced behavior during gesture sessions. Thus, it is likely that gesture imitation training directly enhanced language use in other ways as well. This possibility is consistent with a number of studies of the role of gesture in language development in typical children. These studies have shown that early gesture use is correlated with later vocabulary comprehension and production (e.g., Bates, Thal, Whitesell, Fenson, & Oakes, 1989; Bavin et al., 2008). Further, gesture has been shown to have a tight relationship with lexical and syntactic development. For example, Iverson and Goldin-Meadow (2005) found that lexical items first produced in gesture quickly emerged in the children’s verbal lexicon. Similarly, children who began to use gesture-word combinations to produce two elements in a proposition were the first to produce two-word combinations. Thus, there is evidence to suggest that, in typical development, gesture precedes and, in some cases, directly supports the acquisition of early vocabulary and grammar skills (Capone & McGregor, 2004).
Several possibilities for how gesture may facilitate language use in typical and atypical development have been proposed. One possibility is that the use of gestures eases the process of speech production by reducing demands on memory (Iverson & Goldin-Meadow, 2005). In our study, teaching gesture imitation may have improved spontaneous gesture use. The use of these spontaneous gestures may then have reduced cognitive load (Özçalişkan & Goldin-Meadow, 2005), which may have increased the children’s ability to use previously heard verbal markers, a result we found in our previous work (Ingersoll et al., 2007).
Another possibility is that gesture serves as signal to the child’s communicative partner that the child is ready for a particular type of linguistic input (Iverson & Goldin-Meadow, 2005). Indeed, there is evidence that when children begin using gestures, their parents perceive their communication as more intentional and provide increased linguistic input (Yoder et al., 1994). In our study, although the therapist’s language input was kept constant across conditions, it is possible that increases in child gesture use led to greater parent linguistic input, which in turn, promoted child language use.
This study provides additional evidence that targeting nonverbal imitation can lead to improvements in language skills. Although previous studies on RIT have shown that increases in language behaviors co-occurred with the onset of treatment (Ingersoll et al., 2007; Ingersoll & Schreibman, 2006), it is not clear whether these gains were specifically due to improvement in imitation skills, or whether they were due to some other aspect of the treatment. For example, two RIT strategies that are used to facilitate reciprocity, contingent imitation and modeling descriptive language, have been shown to increase language skills in children with autism and other developmental delays when used in isolation (e.g., Gazdag & Warren, 2000; Girolametto, Pearce, & Weitzman, 1996). In this study, however, contingent imitation of the child’s verbal and nonverbal behavior and modeling language were kept constant across phases, as they are implemented similarly when targeting object and gesture imitation. Thus, the fact that the rate of language use increased for three of the children with the onset of gesture imitation training suggests that teaching gesture imitation skills can improve language use.
There are several limitations to this study. First, only three of the four children showed durable gains in their rate of language use with the introduction of gesture imitation training. Richard showed an initial increase; however, he also exhibited a gradual decline in his rate of language use across treatment. Interestingly, he showed gains from pre- to post-treatment in his rate of language use on the UIA, and he also had a substantial increase in his vocabulary size. These findings suggest that he exhibited improvements in language skills outside of the treatment sessions; thus, the intervention did not negatively affect his language skills. Then why did he exhibit a decrease in rate of language use across treatment sessions? Richard appeared to use the most language at the beginning of a training phase, both during the object imitation only phase, and again with the addition of gesture imitation training. Thus, it is possible that Richard used more language when the situation was novel, declining in language use as the situation became more familiar. It is also possible his illness prevented him from showing his true range of skills during treatment sessions. The fact that his language use began increasing towards the end of treatment around the same time he exhibited an improvement in health supports this possibility. Thus, while this study provides preliminary support for the theory the addition of gesture imitation training enhances language use in children with autism more than object imitation training alone, additional research is needed.
Another limitation is that, due to the larger treatment design, this study did not include a true baseline phase. On the one hand, our design provides a very conservative measure of the effect of gesture imitation on language development because object imitation training (phase 1) has been shown to improve language skills in young children with autism in previous research (Ingersoll & Scheibman, 2006). However, given the lack of a true baseline, we cannot determine the degree to which object imitation alone improved language skill. In addition, this study introduced object imitation prior to gesture imitation for all children, and object imitation was continued throughout treatment. Thus, it is unclear whether the result would have differed had gesture imitation been introduced first or whether object and gesture imitation training had been used in isolation. Thus, additional research is needed to determine the individual contributions of both object and gesture imitation implemented both in isolation and in combination on language use in children with autism. Also, all of the children in this study were verbal. Therefore, it is unknown whether similar results would have been obtained with nonverbal children. In addition, the primary coder provided some of the intervention and was not blind to the goal of study, which could have affected the objectivity of the coding. Finally, the small number of participants limits the generalizability of the findings.
In sum, this study provides additional support for the efficacy of RIT at improving social-communication skills in young children with ASD. Further, it suggests that adding gesture imitation training to object imitation training using RIT can improve language use in some children. This finding is consistent with research demonstrating an association between gesture imitation and use and language development in children with autism and typical development. These findings would suggest that teaching gesture use to young children with ASD, either via RIT or other naturalistic methods, may be an effective approach for improving language skills (Capone & McGregor, 2004). Further, these benefits do not appear to be limited to preverbal children; rather, gesture use may also be an important treatment target for children with ASD who exhibit some verbal language. Future research which can examine the exact mechanisms by which teaching gesture imitation improves language in children with autism is needed.
Acknowledgments
This study was supported by a grant from Autism Speaks to the first author (#ASCN5020). We are grateful to the children and their families who participated in this research. We would also like to thank Nicole Bonter and Matthew Goodman for their assistance on this project.
References
- Acredolo LP, Goodwyn SW. Sign language among hearing infants: The spontaneous development of symbolic gestures. In: Volterra V, Erting C, editors. From gesture to language in hearing and deaf children. New York: Springer; 1990. pp. 68–78. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: American Psychiatric Association; 2000. text revision. [Google Scholar]
- Bates E, Bretherton I, Snyder L, Beeghly M, Shore C, McNew S, Carlson V, Williamson C, Garrison A. From first words to grammar: Individual differences and dissociable mechanisms. New York: Cambridge University Press; 1988. [Google Scholar]
- Bates E, Thal D, Whitesell K, Fenson L, Oakes L. Integrating language and gesture in infancy. Developmental Psychology. 1989;25:1004–1019. [Google Scholar]
- Bavin EL, Prior M, Reilly S, Bretherton L, Williams J, Eadie P, Barrett Y, Ukoumunne OC. The early language in Victoria study: Predicting vocabulary at age one and two years from gesture and object use. Journal of Child Language. 2008;35:687–701. doi: 10.1017/S0305000908008726. [DOI] [PubMed] [Google Scholar]
- Bayley N. Bayley Scales of Infant and Toddler Development. 3. San Antonio, TX: Pearson Education, Inc; 2006. [Google Scholar]
- Capone NC, McGregor KK. Gesture development: A review for clinical and research practices. Journal of Speech, Language, and Hearing Research. 2004;47:173–186. doi: 10.1044/1092-4388(2004/015). [DOI] [PubMed] [Google Scholar]
- Carpenter M, Pennington BF, Rogers SJ. Interrelations among social-cognitive skills in young children with autism. Journal of Autism and Developmental Disorders. 2002;32(2):91–106. doi: 10.1023/a:1014836521114. [DOI] [PubMed] [Google Scholar]
- Clibbens J, Powell G, Atkinson E. Strategies for achieving joint attention when signing to children with Down’s syndrome. International Journal of Language and Communication Disorders. 2002;37(3):309–323. doi: 10.1080/13682820210136287. [DOI] [PubMed] [Google Scholar]
- DeMyer MK, Alpern GD, Barton S, DeMyer WE, Churchill DW, Hingtgen JN, et al. Imitation in autistic, early schizophrenic, and non-psychotic subnormal children. Journal of Autism and Developmental Disorders. 1972;2(3):264–287. doi: 10.1007/BF01537618. [DOI] [PubMed] [Google Scholar]
- Fenson L, Dale PS, Reznick JS, Thal D, Bates E, Hartung JP, et al. MacArthur Communicative Development Inventories: User’s Guide and Technical Manual. San Diego, CA: Singular Publishing Group; 1993. [Google Scholar]
- Gazdag G, Warren SF. Effects of adult contingent imitation on development of young children’s vocal imitation. Journal of Early Intervention. 2000;23(1):24–35. [Google Scholar]
- Girolametto L, Pearce PS, Weitzman E. Interactive focused stimulation for toddlers with expressive vocabulary delays. Journal of Speech, Language and Hearing Research. 1996;39(6):1274–1283. doi: 10.1044/jshr.3906.1274. [DOI] [PubMed] [Google Scholar]
- Hartmann DP. Considerations in the choices of interobserver reliability estimates. Journal of Applied Behavior Analysis. 1977;10:103–116. doi: 10.1901/jaba.1977.10-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hersen M, Barlow DH. Single case experimental designs: Strategies for studying behavior change. Oxford, UK: Pergamon Press; 1976. [Google Scholar]
- Ingersoll B. The social role of imitation in autism: implications for the treatment of imitation deficits. Infants & Young Children. 2008;21(2):107–119. [Google Scholar]
- Ingersoll B, Lewis E, Kroman E. Teaching the imitation and spontaneous use of descriptive gestures in young children with autism using a naturalistic behavioral intervention. Journal of Autism and Developmental Disorders. 2007;37(8):1446–1456. doi: 10.1007/s10803-006-0221-z. [DOI] [PubMed] [Google Scholar]
- Ingersoll B, Schreibman L. teaching reciprocal imitation skills to young children with autism using a naturalistic behavioral approach: Effects on language, pretend play, and joint attention. Journal of Autism and Developmental Disorders. 2006;36(4):487–505. doi: 10.1007/s10803-006-0089-y. [DOI] [PubMed] [Google Scholar]
- Iverson J, Goldin-Meadow S. Gesture paves the way for language development. Psychological Science. 2005;16(5):367–371. doi: 10.1111/j.0956-7976.2005.01542.x. [DOI] [PubMed] [Google Scholar]
- Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, DiLavore PC, et al. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders. 2000;30(3):205–223. [PubMed] [Google Scholar]
- Meltzoff A, Moore M. Imitation of facial and manual gestures by human neonates. Science. 1977;198(4312):75–78. doi: 10.1126/science.198.4312.75. [DOI] [PubMed] [Google Scholar]
- Noldus LPJJ. The Observer: A software system for the collection and analysis of observational data. Behavior Research Methods, Instruments, & Computers. 1991;23(3):415–429. [Google Scholar]
- Özçaliskan S, Goldin-Meadow S. Gesture is at the cutting edge of early language development. Cognition. 2005;96(3):101–113. doi: 10.1016/j.cognition.2005.01.001. [DOI] [PubMed] [Google Scholar]
- Rogers SJ. An examination of the imitation deficit in autism. In: Nadel J, Butterworth G, editors. Imitation in infancy. Cambridge: Cambridge University Press; 1999. pp. 254–279. [Google Scholar]
- Rogers SJ, Pennington BF. A theoretical approach to the deficits in infantile autism. Development and Psychopathology. 1991;3(2):137–162. [Google Scholar]
- Rogers S, Bennetto L, McEvoy R, Pennington B. Imitation and pantomime in high-functioning adolescents with autism spectrum disorders. Child Development. 1996;67(5):2060–2073. [PubMed] [Google Scholar]
- Sigman M, Ungerer JA. Cognitive and language skills in autistic, mentally retarded, and normal children. Developmental Psychology. 1984;20(2):293–302. [Google Scholar]
- Stone WL, Ousley OY, Littleford CD. Motor imitation in young children with autism: What’s the object? Journal of Abnormal Child Psychology. 1997;25(6):475–485. doi: 10.1023/a:1022685731726. [DOI] [PubMed] [Google Scholar]
- Stone WL, Yoder PJ. Predicting spoken language level in children with autism spectrum disorders. Autism. 2001;5(4):341. doi: 10.1177/1362361301005004002. [DOI] [PubMed] [Google Scholar]
- Toth K, Munson J, Meltzoff NA, Dawson G. Early predictors of communication development in young children with autism spectrum disorder: Joint attention, imitation, and toy Play. Journal of Autism and Developmental Disorders. 2006;36(8):993–1005. doi: 10.1007/s10803-006-0137-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uzgiris IC. Two functions of imitation during infancy. International Journal of Behavioral Development. 1981;4(1):1–12. [Google Scholar]
- Warren SF, Yoder PJ, Gazdag GE, Kim K. Facilitating prelinguistic communication skills in young children with developmental delay. Journal of Speech & Hearing Research. 1993;36:83–97. doi: 10.1044/jshr.3601.83. [DOI] [PubMed] [Google Scholar]
- Yoder P, Warren SF, Kim K, Gazdag G. Facilitating prelinguistic communication skills in young children with developmental delay II. Journal of Speech and Hearing Research. 1994;37:841–851. doi: 10.1044/jshr.3704.841. [DOI] [PubMed] [Google Scholar]
- Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scales. 4. San Antonio, TX: Pearson Education, Inc; 2002. [Google Scholar]