

Abstract
Purpose.
To qualitatively classify and compare types of iris insertion among American Caucasians, American Chinese, and mainland Chinese.
Methods.
Prospective multicenter cross-sectional study. Sex- and age-matched Caucasian, American Chinese, and mainland Chinese cohorts were enrolled. Ultrasound biomicroscopy (UBM) images of the anterior chamber were acquired. Qualitative classification of iris insertion into basal, middle, and apical categories was performed. Proportions of each type of insertion were compared among racial groups. Multivariate logistic regression was carried out adjusting for potential confounders.
Results.
Data from 117, 129, and 112 subjects were available for American Caucasian, American Chinese, and mainland Chinese subjects, respectively. The most common type of iris insertion in the superior quadrant was basal insertion in both ethnic Chinese and Caucasians. In the inferior, nasal, and temporal quadrants, Chinese showed significantly higher proportions of nonbasal insertion (P = 0.048, P < 0.0001, P < 0.0001, respectively). After adjusting for confounders, nonbasal insertion was significantly associated with Chinese ethnicity in nasal and temporal quadrants (nasal, OR: 3.1, temporal, OR: 4.8). Increasing proportions of nonbasal insertion were found with advancing age in both Chinese and Caucasians.
Conclusions.
Chinese have significantly higher proportions of nonbasal iris insertion in the nasal and temporal quadrants when compared with Caucasians, even after adjusting for ASOCT-measured anterior segment biometry and iris characteristics. Longitudinal studies in patients who have PAC/PACG are needed to fully elucidate the relationship between iris insertion and angle closure development.
Keywords: UBM, interethnic comparison, iris insertion, angle closure, PACG
Chinese have significantly higher proportions of nonbasal iris insertions in the inferior, nasal, and temporal quadrants when compared to Caucasians, after adjusting for ASOCT measured anterior chamber biometry and iris profile.
Introduction
Worldwide, glaucoma is the second leading cause of ocular morbidity and vision loss, affecting 60 million people.1 Asians are the largest group affected, comprising 47% of all types of glaucoma and more than 85% of primary angle closure glaucoma (PACG).1 Women are also more disproportionally affected than men, comprising nearly 60% of all glaucoma and 70% of PACG.1 Although PACG is estimated to account for only 25% of all glaucomatous disease, these patients on average suffer considerably greater vision loss than those with the open angle form.2,3
Continuous efforts to identify risk factors associated with angle closure have found anatomical features, such as smaller anterior chamber depth (ACD) and anterior chamber width (ACW),4–8 larger lens vault (LV),9 thicker lens,9 thicker peripheral iris, and larger iris cross-sectional area to be associated with increased risk for angle closure.10,11 Dynamic behavior of the iris during light-to-dark changes might also be contributory.12,13 However, additional factors are yet to be identified to fully explain the markedly increased risk of angle closure in people with East Asian ancestry.
Ultrasound biomicroscopy (UBM) has been shown to be an excellent tool in assessing anterior chamber structures.14–16 In this study, we sought to compare the difference in iris insertion among American Caucasians, American Chinese, and mainland Chinese using UBM acquired images. Interethnic deviations in types of iris insertion may provide guidance in developing future longitudinal studies of iris profile in patients who have PAC/PACG in order to identify novel risk factors for angle closure. This can potentially provide guidance for clinical screening, management, and prevention of angle closure in the future.
Methods
Subjects
Institutional review board/ethics committee approval was obtained from the University of California, San Francisco, and Zhongshan Ophthalmic Center in Guangzhou. This study adhered to the Tenets of the Declaration of Helsinki. Written informed consent was obtained for all individuals who enrolled in this study.
The study sample was composed of three cohorts: American Caucasians, American Chinese residing in San Francisco, and mainland Chinese residing in Guangzhou, China. The subjects were enrolled over the period from May 2008 through December 2010. Each cohort was designed to have approximately 120 subjects, including 30 people (15 male and 15 female) in each of the fifth to eighth decades of life. All subjects in San Francisco were consecutively recruited from the general ophthalmology clinics. Participants at the Guangzhou site were drawn from an ongoing population-based study. Inclusion criteria included age between 40 and 80 years, self-reported Caucasian or Chinese ancestry for both parents (the term “Caucasian” for the purpose of this study included only European-derived white people), and willingness and ability to participate in all study activities. Exclusion criteria included bilateral pseudophakia or aphakia or any prior intraocular surgery or laser treatment with the potential to alter the natural anatomy of the anterior segment, corneal or conjunctival abnormalities that preclude an adequate view of the anterior chamber on the UBM images, use of any glaucoma medications, active ocular infection where contact eye examinations might be contraindicated, and high refractive error, defined as spherical equivalent (SE) less than −8 or greater than +4 diopters.
Image Acquisition
The anterior segment of all subjects was imaged using UBM (model P45; Paradigm Medical, Salt Lake City, UT). All UBM examinations performed at Guangzhou, China, were conducted by a single examiner (DW), who is an experienced UBM operator and was trained by MH. The exact same protocol was followed by SCL, an experienced UBM operator since his fellowship, under the direction of DW, who came to the United States to be the coordinator of the study at San Francisco. All subjects were imaged under standardized dark conditions with illuminations below 1 lux in the supine position. After topical anesthesia instillation, an eyecup was placed and saline or hydroxypropyl methylcellulose (Gonak; Akorn, Inc., Somerset, NJ) was used as the coupling agent. The probe was placed perpendicular to the ocular surface, and images of all four quadrants were obtained, with care to avoid pressure on the globe. Variation in accommodation was minimized by asking participating subjects to fixate on a target on the ceiling with the contralateral eye. Only images in which the scleral spur, drainage angle, ciliary body, and a half chord of the iris, which refers to half of the length between the iris insertion and the pupillary margin, could be clearly visualized were accepted. The subjects who refused the UBM examination or were not able to cooperate during UBM examination were excluded.
Image Analysis
Images from the right eye were used for analysis. The left eye's data were used when the right eye did not meet the eligibility criteria. Two masked researchers (YEW, YL) reviewed images from all subjects to classify the iris insertion into three categories, graded according to the location of the iris insertion into the ciliary body, based on the criteria described by Jiang et al.16 Basal iris insertion was defined as the iris insertion located near the base of the ciliary body; middle iris insertion was defined as the iris insertion located around the middle portion the ciliary body; and apical iris insertion was defined as the iris inserted toward the apex of the ciliary body (Figure). The types of iris insertion for each of the four quadrants of the anterior chamber were assessed separately and in a masked fashion without knowledge of patient demographics or quadrant location. Representative images were selected as standard illustrations. For the purpose of reproducibility and interobserver variability tests, 72 images, 24 from each cohort, were selected randomly, and independently assessed by two observers (YEW, YL). To control for intraobserver variability, one observer (YEW) performed the assessment again two weeks later. The intraobserver agreement in evaluating iris insertion was high in all four quadrants (Table 1, range of κ values, 0.83–0.91). The interobserver agreement in iris classification was also high in all quadrants (Table 1, range of κ values, 0.74–0.91). Both results are consistent with previously reported values.15,16
Table 1.
Reproducibility of Iris Insertion Identification in a Subset of 24 Eyes by Quadrant
| Quadrant | Interobserver κ | 95% CI |
| Superior | 0.90 | 0.72–1.09 |
| Nasal | 0.91 | 0.75–1.08 |
| Inferior | 0.83 | 0.61–1.05 |
| Temporal | 0.74 | 0.46–1.00 |
| Quadrant | Intraobserver κ | 95% CI |
| Superior | 0.80 | 0.54–1.06 |
| Nasal | 0.91 | 0.75–1.08 |
| Inferior | 0.91 | 0.74–1.08 |
| Temporal | 0.74 | 0.47–1.00 |
Interobserver and intraobserver variability were tested using Kappa statistics.
Figure. .
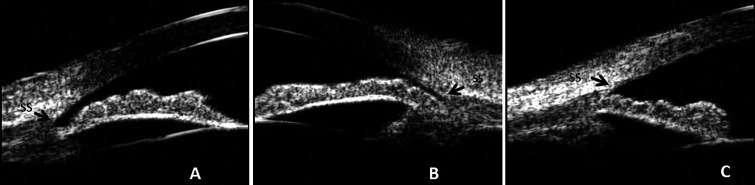
Iris root insertion classification based on ultrasound biomicroscopy imaging. (A) Apical insertion; (B) middle insertion; (C) basal insertion. Black arrow denotes the scleral spur.
Other Related Examinations
All subjects underwent a detailed slit-lamp examination by a well-qualified ophthalmologist, where both vertical and horizontal cup-to-disc ratios and gonioscopy were included. An autorefractor (Automatic Refractor/Keratometer, Model 599; Humphrey Zeiss, Dublin, CA) was used to measure noncycloplegic refraction. All raw refractive data were converted to SE (sphere plus one-half of cylinder) for analysis. A-scan ultrasound (E-Z Scan A/B 5500+; Sonomed, Inc., Lake Success, NY) was used to measure axial length (AL), anterior chamber depth (ACD), and lens thickness (LT). Anterior segment optical coherence tomography (ASOCT) (Visante OCT; Carl Zeiss Meditec, Inc., Dublin, CA) was performed to measure anterior chamber biometry including ACD, anterior chamber width (ACW), anterior chamber area (ACA), anterior chamber volume (ACV), and iris parameters, including iris thickness at 750 μm from the scleral spur (IT750), iris area (Iarea), and iris curvature (Icurv). Images were taken in the horizontal meridian with iris measurements available for only the nasal and temporal quadrants. Custom software, the Zhongshan Angle Assessment Program (ZAAP; State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China), was used for all image analysis.
Statistical Analysis
Proportions of each type of iris insertion observed in the UBM images were calculated and compared by Pearson χ2 tests. ANOVA and Student's t-tests were used for continuous data. All tests were two-tailed. P values less than 0.05 were deemed statistically significant. Logistic regression of iris insertion type was performed to adjust for age, sex, ethnicity, AL, SE, ACD, ACW, ACV, IT750, Icurv, and Iarea. All analyses were performed with statistical software JMP 10.0 (SAS, Inc., Cary, NC).
Results
There were a total of 117, 129, and 112 American Caucasian, American Chinese, and mainland Chinese subjects, respectively, who had UBM images available for this study. Two subjects were excluded for use of glaucoma medications, and no subject was excluded for corneal or conjunctival abnormities. UBM images were of right eyes except in cases in which the right eye did not meet the inclusion criteria. Left eye UBM data were used in six (5%), three (2.3%), and five (4.5%) participants from each cohort, respectively. All three groups had a similar average age. The American Caucasian cohort had a mean age of 59.7 ± 11.6 years, and the American Chinese and mainland Chinese cohorts had mean ages of 59.4 ± 12.0 and 59.63 ± 11.7 years, respectively (P = 0.98, Table 2). Proportions of males and females were also similar among the three cohorts (P = 0.43, Table 2). Refractive error and ocular measurements by A-scan ultrasound were also compared across the three groups using ANOVA; there were significant differences in the SE (P < 0.0001), AL (P < 0.0001), LT (P = 0.002), and ACD (P < 0.0001) (Table 2) among the 3 groups.
Table 2.
Demographics and Ocular Measurements From A-Scan Ultrasound in American Caucasian, American Chinese, and Mainland Chinese
|
American Caucasian,
n
= 117 |
American Chinese,
n
= 129 |
Mainland Chinese,
n
= 112 |
P
Value |
|
| Age, y | 59.7 ± 11.6 | 59.4 ± 12.0 | 59.4 ± 11.7 | 0.98 |
| Sex, M/F | 63/54 | 62/67 | 51/61 | 0.43* |
| SE, D | −1.42 ± 3.9 | −2.10 ± 3.8 | −0.07 ± 2.2 | <0.0001† |
| AL, mm | 24.3 ± 1.7 | 24.5 ± 2.02 | 23.4 ± 1.0 | <0.0001† |
| LT, mm | 4.51 ± 0.4 | 4.49 ± 0.5 | 4.70 ± 0.4 | 0.0002† |
| ACD, mm | 3.42 ± 0.3 | 3.23 ± 0.4 | 2.94 ± 0.4 | <0.0001† |
Demographic data and ocular measurements compared among three ethnic groups using ANOVA. Data are presented as mean ± SD except for sex, which is presented as male-to-female ratio. Numbers in bold denote statistical significance (P < 0.05).
P value from Pearson χ2 test among all three groups.
When pairwise comparisons were done, mainland Chinese were found to be significantly different from the other two cohorts. No significant differences were detected between American Caucasians and American Chinese.
Proportions of different types of iris insertion were compared between Caucasians and ethnic Chinese cohorts using Pearson χ2 tests. Because results did not differ significantly between American Chinese and mainland Chinese cohorts (all P values > 0.05, Table 3), we combined the two ethnic Chinese groups for the purpose of further analysis in this study. In the superior quadrant, basal insertion was the most common type in both Caucasians and Chinese (P = 0.60, Table 3). In the nasal quadrant, Caucasians had more than 52% basal insertions, whereas the most frequently observed type of insertion in the Chinese cohort was the middle type (P < 0.0001, Table 3). In the inferior quadrant, Caucasians had approximately 41% of middle and 50% of basal insertions. This was also significantly different from that of the Chinese, in whom nearly 55% were the middle type (P = 0.04, Table 3). Similar results were found in the temporal quadrant, where Caucasians had almost 49% of the basal type, whereas Chinese had approximately 63% middle and 21% basal insertions (P < 0.0001, Table 3). Since the apical insertion type was found to be rare in all four quadrants, especially in the Caucasian cohort, the apical and middle insertion types were combined and redefined as the nonbasal type for further analysis. After this combination, Chinese were found to have a significantly higher percentage of nonbasal insertion in all quadrants but the superior one (superior, P = 0.55; nasal, P < 0.0001; inferior, P = 0.01; temporal, P < 0.0001).
Table 3.
Iris Root Insertion Classification in American Caucasian, American Chinese, and Mainland Chinese
|
Quadrant |
Classification |
American Caucasian,
n
= 117,
n
(%) |
American Chinese,
n
= 129,
n
(%) |
Mainland Chinese,
n
= 112,
n
(%) |
3-Group Comparison
P
Value* |
Chinese Groups Comparison
P
Value† |
| Superior | Basal | 67 (57.3) | 69 (53.5) | 61 (54.6) | 0.86 | 0.89 |
| Middle | 42 (35.9) | 48 (37.2) | 39 (34.8) | |||
| Apical | 8 (6.8) | 12 (9.3) | 12 (10.7) | |||
| Nasal | Basal | 62 (52.9) | 35 (27.1) | 35 (31.3) | 0.0004 | 0.72 |
| Middle | 42 (35.9) | 78 (60.5) | 62 (55.4) | |||
| Apical | 13 (11.1) | 16 (12.4) | 15 (13.4) | |||
| Inferior | Basal | 58 (49.8) | 43 (33.3) | 44 (40.0) | 0.04 | 0.19 |
| Middle | 48 (41.0) | 71 (55.0) | 60 (54.6) | |||
| Apical | 11 (9.4) | 15 (11.6) | 6 (5.5) | |||
| Temporal | Basal | 57 (48.7) | 23 (17.8) | 27 (24.1) | <0.0001 | 0.43 |
| Middle | 52 (44.4) | 83 (64.3) | 69 (61.6) | |||
| Apical | 8 (6.8) | 23 (17.8) | 16 (14.3) |
Percentage distribution of iris insertion type among three ethnic groups was compared using Pearson χ2 tests. Data are presented as counts (proportion).
P values are for comparisons among all three ethnic groups.
P values are for comparisons between American Chinese and mainland Chinese. P values in bold denote statistical significance (P < 0.05). Differences in pairwise comparisons for American Caucasian versus American Chinese, and American Caucasian versus mainland Chinese in nasal and temporal quadrants are significant with Bonferroni adjustment (P < 0.016). Differences in the superior and inferior quadrants are not significant.
When anterior segment biometry measured by ASOCT (horizontal scan) was compared, significantly shallower ACD and smaller ACW, ACA, and ACV were found in eyes with nonbasal insertion in the nasal, inferior and temporal quadrants independently (Table 4). Iris characteristics were also compared based on iris insertion (basal versus nonbasal) in the nasal and temporal quadrants separately. IT750, Iarea, and Icurv were all found to be significantly different between the two cohorts in both quadrants. The nonbasal cohort showed thicker peripheral irides (Table 4, IT750, P = 0.02 for nasal, P = 0.02 for temporal), larger iris area (Table 4, P = 0.009 for nasal, P = 0.004 for temporal), and larger iris curvature (Table 4, P = 0.0003 for nasal, P < 0.0001 for temporal). Sex composition did not differ between the basal and nonbasal cohorts (Table 4, superior, P = 0.15; nasal, P = 0.84; inferior, P = 0.48; temporal P = 0.89).
Table 4.
Differences in Demographic, Anterior Segment Biometry, and Iris Characteristics Between Basal Insertion and Nonbasal Insertion Cohorts by Quadrant
|
Basal Insertion Cohort |
Nonbasal Insertion Cohort |
P
Value |
|
| Sex, M/F | |||
| S | 90/107 | 86/75 | 0.15 |
| N | 64/68 | 112/114 | 0.84 |
| I | 68/77 | 108/105 | 0.48 |
| T | 52/55 | 124/127 | 0.89 |
| ACD, mm | |||
| S | 2.74 ± 0.42 | 2.69 ± 0.36 | 0.37 |
| N | 2.78 ± 0.37 | 2.69 ± 0.37 | 0.04 |
| I | 2.80 ± 0.39 | 2.67 ± 0.39 | 0.003 |
| T | 2.85 ± 0.38 | 2.67 ± 0.39 | 0.0001 |
| ACW, mm | |||
| S | 11.89 ± 0.51 | 11.86 ± 0.51 | 0.58 |
| N | 11.98 ± 0.52 | 11.81 ± 0.49 | 0.004 |
| I | 11.95 ± 0.51 | 11.82 ± 0.50 | 0.03 |
| T | 12.00 ± 0.49 | 11.82 ± 0.51 | 0.003 |
| ACA, mm2 | |||
| S | 21.73 ± 4.76 | 21.06 ± 4.12 | 0.19 |
| N | 22.27 ± 4.79 | 20.96 ± 4.26 | 0.02 |
| I | 22.35 ± 4.54 | 20.82 ± 4.37 | 0.003 |
| T | 22.97 ± 4.39 | 20.78 ± 4.39 | <0.0001 |
| ACV, mm3 | |||
| S | 150.04 ± 43.17 | 145.0 ± 37.05 | 0.27 |
| N | 155.25 ± 43.52 | 143.56 ± 38.35 | 0.02 |
| I | 155.33 ± 41.55 | 142.75 ± 39.33 | 0.008 |
| T | 160.89 ± 40.59 | 142.28 ± 39.47 | 0.0003 |
| IT750, mm | |||
| N | 0.42 ± 0.07 | 0.44 ± 0.07 | 0.02 |
| T | 0.42 ± 0.07 | 0.44 ± 0.07 | 0.01 |
| Iarea, mm2 | |||
| N | 1.48 ± 0.21 | 1.55 ± 0.24 | 0.009 |
| T | 1.46 ± 0.22 | 1.55 ± 0.23 | 0.004 |
| Icurv, mm | |||
| N | 0.21 ± 0.15 | 0.28 ± 0.13 | 0.0003 |
| T | 0.19 ± 0.14 | 0.28 ± 0.14 | <0.0001 |
Data are presented as mean ± SD. P values are for Student's t-tests. P values in bold denote statistical significance (P < 0.05). Anterior segment and iris parameters were assessed by anterior segment optical coherence tomography. Data were obtained from a single image taken in the horizontal meridian. ASOCT measurements were compared based on subjects' iris insertion type in a particular quadrant (basal versus nonbasal). S, superior quadrant; N, nasal quadrant; I, inferior quadrant; T, temporal quadrant.
The difference in iris insertion type between Caucasian and ethnic Chinese was further verified with a multivariate logistic regression model adjusting for potential confounding factors, including age, sex, ethnicity, AL, SE, ACD, ACW, ACV, IT750, Icurv, and Iarea (Table 5). Because ASOCT measured iris parameters only in the horizontal meridian, the regression analysis was carried out for the nasal and temporal quadrants only. Our results showed that in both the nasal and temporal quadrants, Chinese ethnicity (nasal, odds ratio [OR]: 3.1, P = 0.002; temporal, OR: 4.8, P < 0.0001), shallower ACD (nasal, P = 0.04; temporal, P = 0.006), smaller ACW (nasal, P = 0.0002; temporal, P = 0.006), smaller ACV (nasal, P = 0.0004; temporal, P = 0.0003), larger Icurv (nasal, P < 0.0001; temporal, P < 0.0001), and larger Iarea (nasal, P = 0.02; temporal, P = 0.03) are all significantly associated with nonbasal iris insertion. Older age was found to be associated with nonbasal iris insertion in the temporal quadrant only (nasal, P = 0.26; temporal, P = 0.01).
Table 5.
Logistic Regression for Associated Factors With Types of Iris Insertion in Nasal and Temporal Quadrant Among all Study Subjects
|
Nasal |
Temporal |
|||||||
|
β* |
P
Value |
OR† |
95% CI‡ |
β* |
P
Value |
OR† |
95% CI‡ |
|
| Age | 0.02 | 0.21 | 1.01 | 0.99–1.04 | 0.04 | 0.007 | 1.04 | 1.01–1.07 |
| Sex | −0.02 | 0.91 | 1.03 | 0.60–1.78 | −0.03 | 0.82 | 1.07 | 0.58–1.97 |
| Ethnicity | −0.57 | 0.001 | 3.14 | 1.60–6.31 | −0.8 | <0.0001 | 4.80 | 2.31–10.3 |
| AL | 0.11 | 0.36 | 1.12 | 0.90–1.47 | 0.19 | 0.21 | 1.21 | 0.94–1.71 |
| SE | 0.03 | 0.53 | 1.03 | 0.94–1.14 | 0.05 | 0.41 | 1.05 | 0.94–1.20 |
| ACD | −2.94 | 0.02 | 0.05 | 0.004–0.58 | −4.46 | 0.001 | 0.01 | 0.0007–0.16 |
| ACW | −2.32 | 0.0002 | 0.1 | 0.03–0.32 | −1.90 | 0.005 | 0.15 | 0.04–0.54 |
| ACV | 0.06 | 0.0002 | 1.06 | 1.03–1.10 | 0.07 | 0.0001 | 1.07 | 1.04–1.12 |
| IT750 | 0.60 | 0.78 | 1.83 | 0.02–139.7 | 2.22 | 0.37 | 9.23 | 0.08–1,220.5 |
| Iarea | 2.15 | 0.01 | 8.58 | 1.74–45.5 | 2.07 | 0.02 | 7.94 | 1.40–49.2 |
| Icurv | 7.13 | <0.0001 | 1250.8 | 61.7–32,051.3 | 7.10 | <0.0001 | 1210.4 | 48.0–39,799.5 |
For sex, male was coded as 1 and female as 2 in regression models. For ethnicity, American Caucasians were coded as 0 and ethnic Chinese coded as 1. Numbers in bold denote the association is statistically significant (P < 0.05).
Beta coefficient.
OR. Unit odds ratio is presented for continuous variables.
95% confidence interval (CI) for OR. ACA is not included in the model because it is highly correlated with ACV.
To further elucidate the relationship between age and iris insertion, we divided the study population into four age groups with 10-year increments. An apparently increasing number of nonbasal insertion was observed in all four quadrants with increasing age based on Pearson χ2 tests, although statistical significance was detected only in the superior and temporal quadrants (superior, 13.82% [40–49 years old], 41.11% [50–59 years old], 48.9% [60–69 years old], 57.8% [70–80 years old], P = 0.003; nasal, 53.4%, 62.2%, 66.7%, 70.0%, P = 0.12; inferior, 48.9%, 61.0%, 61.1%, 66.67%, P = 0.10; temporal, 55.7%, 67.8%, 74.4%, 82.2%, P = 0.001). We further analyzed this observation by comparing the proportion of nonbasal insertion in the top age group with the bottom age group using Pearson χ2 tests for each ethnicity separately. In Caucasians, higher percentages of nonbasal insertion were identified in all quadrants in the top age group, and statistical significance was found in the superior (57.7% vs. 27.6%; P = 0.02) and temporal (69.3% vs. 37.9%, P = 0.02) quadrants. Similarly, in ethnic Chinese, a significantly higher proportion of the nonbasal insertion was detected in all four quadrants in the older group (superior, 54.7% vs. 33.9%, P = 0.01; nasal, 76.8% vs. 59.3%, P = 0.04; inferior, 70.0% vs. 50.9%, P = 0.03; temporal, 90.0% vs. 64.4%, P = 0.0009).
Discussion
In this prospective multicenter study, American Caucasians and Chinese Americans residing in the San Francisco Bay Area were compared with their age- and sex-matched Chinese counterparts residing in Guangzhou, China, with regard to types of iris insertion. To the best of our knowledge, our study is the first to compare iris insertion between Caucasians and ethnic Chinese using qualitative assessments of UBM images. We found that the proportion of the basal, middle, and apical types of iris insertion differ between American Caucasians and ethnic Chinese, specifically in the nasal, inferior, and temporal quadrants of the anterior chamber. In Caucasians, the most common type of iris insertion in all quadrants was the basal type, followed by middle insertion, with apical insertion averaging to less than 10% across all four quadrants. In the Chinese cohort, the most common type of iris insertion in the superior quadrant was found to be basal, which is consistent with a study published by Jiang et al.16 In the inferior, nasal, and temporal quadrants, however, the most common type of iris insertion observed was the middle type, followed by basal insertion, with apical insertion the least common. Our findings in the temporal and nasal quadrants are largely in keeping with what was reported previously, where nonbasal types of insertion were found to be either more abundant than or on par with the basal insertion.16 Nevertheless, our findings in the inferior quadrant differ from those reported previously, where basal insertion was found to be most common. This discrepancy may be attributed to the smaller sample size of the previous study, and the difference in UBM machines used.
Based on our logistic regression results, we report for the first time that nonbasal iris insertion was significantly associated with shallower ACD, smaller ACW and ACV, and larger iris area and curvature; whereas AL, SE, and IT750 do not seem to affect iris insertion significantly. More importantly, ethnicity was also significantly related to iris insertion after adjusting for these anterior chamber measurements and iris parameters in the nasal and temporal quadrants. Specifically, nonbasal iris insertion was found to be significantly related to Chinese ethnicity, which suggests that nonbasal insertion may be an inherent iris characteristic in ethnic Chinese. ASOCT measurements of the vertical meridian are needed to perform similar analysis in the superior and inferior quadrants.
Two types of appositional angle closure in eyes with PACG based on the topology of the iris root were described previously by Sakuma et al.17 The B-type angle closure starts near the scleral spur, with the iris root inserted more toward the base of the anterior chamber angle, as in our basal insertion. The S-type angle closure, however, starts near Schwalbe's line, with the iris inserted more toward the apex of the ciliary body, as in our nonbasal insertion.17 Dorairaj et al.18 further described these two types of angle closure. In the B type, peripheral iris and iris root move evenly toward the trabecular meshwork (TM); whereas in the S type, peripheral iris moves independently of the iris root toward the TM. Because Chinese eyes were found to have a significantly higher percentage of nonbasal insertion in our study, the type of angle closure that develops in Chinese eyes is more likely to be the S type described above. Unfortunately, due to small sample sizes, the significance of apical insertion (a subtype of nonbasal insertion) could not be evaluated adequately.
The prevalence of PACG and PACS among Chinese has been reported to be approximately 1.4% and 8% to 11%, respectively,19–21 both of which are lower than the frequency of nonbasal insertion found in our study. This suggests that other factors in Chinese eyes besides iris insertion, such as previously described smaller anterior chamber,4,5,7,22 thicker iris,11,23 and greater thickening of the peripheral iris during light-to-dark changes,12 smaller trabecular-iris space area (TISA), and greater reduction of TISA during light-to-dark transition,22 may attribute to their higher risk for angle closure development. Additional factors also may be identified by evaluating ciliary body profile. On the other hand, nonbasal insertion might be a protective factor against angle closure inherent to Chinese eyes. As pointed out by Dorairaj et al.,18 the S-type angle closure can potentially leave a space between the peripheral iris and the trabecular meshwork, which can presumably preserve partial function of the trabecular meshwork. The nonbasally inserted iris, therefore, may act as a protective measure in Chinese eyes as a result of adaptation. Future cross-sectional and longitudinal studies of patients who have PAC/PACG or are PACS are necessary to obtain an accurate picture of the relationship between iris insertion and angle closure. Furthermore, because types of iris insertion differ significantly between Chinese and Caucasian individuals, the mechanism by which angle closure develops in these two racial groups may also differ. Future studies analyzing the potentially different biomechanical behavior between basally and nonbasally inserted irides are necessary to elucidate this potential variation.
Significantly higher proportions of nonbasal iris insertion were found in subjects of the top age group than the bottom one in all four quadrants of the Chinese eyes, as well as the superior and temporal quadrants of the Caucasian eyes. This observation could potentially be attributed to the loosening of the ciliary body from the sclera due to decreasing mechanical support secondary to a reduction of constituent collagen in the sclera with older age.24 In addition, age-related increase of connective tissue in the ciliary body stroma, increasing width, and antero-inward displacement of ciliary muscles may also contribute to the apparent “migration” of the iris insertion toward the apex.25,26 This finding may explain the increasing incidence of angle closure with older age, although future longitudinal studies following the anatomy of the iris insertion with aging is needed to fully understand this relationship.
There are several limitations to our current study. Subjects recruited in San Francisco were clinic-based. Although efforts were made to rule out patients with ocular abnormalities via comprehensive examination and exclusion criteria, selection bias might be inevitable. Family history of glaucoma and visual fields were not recorded for this present study, which may bias our findings. We are obtaining both factors in our other on-going studies for future analyses. Iris color was not an inclusion criterion, which may affect our analyses, particularly of the iris profile. Future studies analyzing Caucasians by iris color grouping may be necessary. Due to the multicenter nature of our study, it is almost inevitable to have more than one operator for UBM image acquisition. Although both of our operators are well-trained and qualified ophthalmologists, and the UBM operator in Guangzhou also coordinated the study in the United States, differences may still exist in imaging techniques, which in turn may influence image interpretation and analysis. Although previously reported, the classification of the qualitative assessment of the iris insertion was subjectively determined. Quality of the images and difficulty in identifying certain anatomical features of the angle may affect the classification results. Particularly, the differentiation between basal iris insertion and appositional closure of an angle whose iris insertion is not basal can be challenging in selected cases. Sample size for each iris insertion type is relatively small; future studies of larger sample sizes especially for the “apical” insertion type are necessary to better extrapolate our findings. Last, all of our analysis was performed with UBM images taken in the dark. The addition of images taken in the light may help us to learn the potentially different dynamic behavior of the iris for different types of iris insertion.
In summary, our study reports for the first time different proportions of the basal, middle, and apical iris insertion types between Caucasians and ethnic Chinese, specifically in the inferior, nasal, and temporal quadrants. This difference between ethnic groups remains significant after adjusting for multiple ASOCT-measured anterior chamber and iris variables. Future longitudinal studies analyzing additional iris characteristics, biomechanical behavior of the iris, and ciliary body profile, as well as studies done in patients who have PAC/PACG are needed to further elucidate the relationship between iris insertion and angle closure development.
Acknowledgments
Supported by National Eye Institute Grant EY002162 (SCL) and National Natural Science Foundation of China Grant 81260147 (YL).
Disclosure: Y.E. Wang, None; Y. Li, None; D. Wang, None; M. He, None; L. Wu, None; S.C. Lin, None
References
- 1. Cook C, Foster P. Epidemiology of glaucoma: what's new? Can J Ophthalmol. 2012; 47: 223–226 [DOI] [PubMed] [Google Scholar]
- 2. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol. 2001; 85: 1277–1282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006; 90: 262–267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Wang D, Huang G, He M, Wu L, Lin S. Comparison of anterior ocular segment biometry features and related factors among American Caucasians, American Chinese and mainland Chinese. Clin Experiment Ophthalmol. 2012; 40: 542–549 [DOI] [PubMed] [Google Scholar]
- 5. Leung CK, Palmiero PM, Weinreb RN, et al. Comparisons of anterior segment biometry between Chinese and Caucasians using anterior segment optical coherence tomography. Br J Ophthalmol. 2010; 94: 1184–1189 [DOI] [PubMed] [Google Scholar]
- 6. Nongpiur ME, Sakata LM, Friedman DS, et al. Novel association of smaller anterior chamber width with angle closure in Singaporeans. Ophthalmology. October 2010; 117: 1967–1973 [DOI] [PubMed] [Google Scholar]
- 7. Foo LL, Nongpiur ME, Allen JC, et al. Determinants of angle width in Chinese Singaporeans. Ophthalmology. 2012; 119: 278–282 [DOI] [PubMed] [Google Scholar]
- 8. Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normal eyes and eyes with primary angle-closure glaucoma. Br J Ophthalmol. 1970; 54: 161–169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Nongpiur ME, He M, Amerasinghe N, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011; 118: 474–479 [DOI] [PubMed] [Google Scholar]
- 10. Wang BS, Narayanaswamy A, Amerasinghe N, et al. Increased iris thickness and association with primary angle closure glaucoma. Br J Ophthalmol. 2011; 95: 46–50 [DOI] [PubMed] [Google Scholar]
- 11. Wang D, He M, Wu L, Yaplee S, Singh K, Lin S. Differences in iris structural measurements among American Caucasians, American Chinese and mainland Chinese. Clin Experiment Ophthalmol. 2012; 40: 162–169 [DOI] [PubMed] [Google Scholar]
- 12. Wang D, He M, Wu L, et al. Dark-light change of iris parameters and related factors among American Caucasians, American Chinese, and Mainland Chinese. Curr Eye Res. 2012; 37: 599–605 [DOI] [PubMed] [Google Scholar]
- 13. Cheung CY, Liu S, Weinreb RN, et al. Dynamic analysis of iris configuration with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2010; 51: 4040–4046 [DOI] [PubMed] [Google Scholar]
- 14. Dada T, Sihota R, Gadia R, Aggarwal A, Mandal S, Gupta V. Comparison of anterior segment optical coherence tomography and ultrasound biomicroscopy for assessment of the anterior segment. J Cataract Refract Surg. 2007; 33: 837–840 [DOI] [PubMed] [Google Scholar]
- 15. Spaeth GL, Azuara-Blanco A, Araujo SV, Augsburger JJ. Intraobserver and interobserver agreement in evaluating the anterior chamber angle configuration by ultrasound biomicroscopy. J Glaucoma. 1997; 6: 13–17 [PubMed] [Google Scholar]
- 16. Jiang Y, He M, Huang W, Huang Q, Zhang J, Foster PJ. Qualitative assessment of ultrasound biomicroscopic images using standard photographs: the Liwan eye study. Invest Ophthalmol Vis Sci. 2010; 51: 2035–2042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Sakuma T, Sawada A, Yamamoto T, Kitazawa Y. Appositional angle closure in eyes with narrow angles: an ultrasound biomicroscopic study. J Glaucoma. 1997; 6: 165–169 [PubMed] [Google Scholar]
- 18. Dorairaj SK, Tello C, Liebmann JM, Ritch R. Narrow angles and angle closure: anatomic reasons for earlier closure of the superior portion of the iridocorneal angle. Arch Ophthalmol. 2007; 125: 734–739 [DOI] [PubMed] [Google Scholar]
- 19. Cheng JW, Cheng SW, Ma XY, Cai JP, Li Y, Wei RL. The prevalence of primary glaucoma in mainland China: a systematic review and meta-analysis. J Glaucoma. 2013; 22: 301–306 [DOI] [PubMed] [Google Scholar]
- 20. He M, Foster PJ, Ge J, et al. Prevalence and clinical characteristics of glaucoma in adult Chinese: a population-based study in Liwan District, Guangzhou. Invest Ophthalmol Vis Sci. 2006; 47: 2782–2788 [DOI] [PubMed] [Google Scholar]
- 21. Liang YB, Friedman DS, Zhou Q, et al. Prevalence of primary open angle glaucoma in a rural adult Chinese population: the Handan eye study. Invest Ophthalmol Vis Sci. 2011; 52: 8250–8257 [DOI] [PubMed] [Google Scholar]
- 22. Wang D, Qi M, He M, Wu L, Lin S. Ethnic difference of the anterior chamber area and volume and its association with angle width. Invest Ophthalmol Vis Sci. 2012; 53: 3139–3144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Quigley HA, Silver DM, Friedman DS, et al. Iris cross-sectional area decreases with pupil dilation and its dynamic behavior is a risk factor in angle closure. J Glaucoma. 2009; 18: 173–179 [DOI] [PubMed] [Google Scholar]
- 24. Rada JA, Achen VR, Penugonda S, Schmidt RW, Mount BA. Proteoglycan composition in the human sclera during growth and aging. Invest Ophthalmol Vis Sci. 2000; 41: 1639–1648 [PubMed] [Google Scholar]
- 25. Pardue MT, Sivak JG. Age-related changes in human ciliary muscle. Optom Vis Sci. 2000; 77: 204–210 [DOI] [PubMed] [Google Scholar]
- 26. Sheppard AL, Davies LN. The effect of ageing on in vivo human ciliary muscle morphology and contractility. Invest Ophthalmol Vis Sci. 2011; 52: 1809–1816 [DOI] [PubMed] [Google Scholar]