

Abstract
Background
The incidence of melanoma continues to increase in many countries, and primary prevention of melanoma includes avoidance of sunburn as well as adequate sun protection behaviour. The aim of this study was to examine the prevalence of self-reported sun protection behaviours and sunburn in users of the Internet, and to identify the demographic, clinical and attitudinal/motivational correlates of sun protection behaviours.
Methods
Self-report data were gathered on behalf of GenoMEL (www.genomel.org) using an online survey available in 10 different languages, and 8,178 individuals successfully completed at least 80% of survey items, with 73% of respondents from Europe, 12% from Australia, 7% from the USA, 2% from Israel, and 6% from other countries.
Results
Half of all respondents and 27% of those with a previous melanoma reported at least one severe sunburn during the previous 12 months. The strongest factors associated with sun protection behaviour were perceived barriers to protection (β=−0.44/β=−0.37), and respondents who reported a positive attitude towards suntans were less likely to protect (β=−0.16/β=−0.14). Reported use of protective clothing and shade, as well as avoidance of midday sun exposure, were more strongly related to reduced risk of sunburn than sunscreen use.
Conclusions
Despite widespread dissemination of public health messages about the importance of sun protection, a substantial proportion of this international sample, including respondents with a previous melanoma, reported inadequate sun protection behaviours resulting in severe sunburn.
Impact
Future strategies to decrease sunburn should target the practical, social and psychological barriers associated with non-uptake of sun protection.
Keywords: Sun exposure, Sunburn, Sun protection, Melanoma
INTRODUCTION
Over the past several decades, melanoma incidence has increased in many fair-skinned populations (1). This is most likely a result of several factors but in particular increases in two important risk factors for melanoma, sun exposure and associated sunburn (2–5). Sun avoidance during periods of peak ultraviolet radiation and the adoption of protective measures when exposed are factors influencing sunburn that theoretically could reduce melanoma risk. Promotion of these protective health behaviours is therefore essential in skin cancer prevention.
Previous studies have identified a number of factors associated with sun protective behaviour. Skin sun-sensitivity is an important factor as those who burn easily are more likely to use sun protection (6, 7). Those with blonde or red hair colour are somewhat more likely to engage in protective behaviour than people with dark hair. Persons who downplay the risk of sunbathing and those who think it is worth becoming burnt to obtain a tan tend to use less sunscreen (8, 9). In contrast, individuals with better knowledge, higher skin cancer awareness and those who perceive themselves as being at risk of developing skin cancer are more inclined to report greater use of sunscreen and other sun protection measures (7). Common reasons not to use sunscreen are that its application is perceived as time consuming and inconvenient, and that sunscreen use reduces the likelihood of getting a desired tan (7, 10).
We report a study that was carried out with the intent of informing the development of an Internet-based prevention tool to increase awareness of personal susceptibility to skin cancer and improve engagement in skin cancer-related behaviours. It is based on theoretical assumptions regarding predictors of sun protection behaviour, as predicated in psychological models of health behaviour; i.e. the Health Belief Model (HBM) and Protection Motivation Theory (PMT; (11–13). In short, we postulated that individuals would report greater engagement in sun protective behaviour if they believed themselves to be susceptible to skin cancer; believed skin cancer to have potentially serious consequences; believed sun protection behaviour to be beneficial in reducing either their vulnerability to, or the severity of, skin cancer; and if they believed the anticipated benefits to outweigh any barriers to taking action. Further, we expected perception of the respondents' ability to successfully protect themselves from the sun (i.e. self-efficacy) and amount of worry about skin cancer to influence behaviour. Severe sunburn due to excessive exposure to ultraviolet radiation and sun protection behaviours were measured along with motivational and attitudinal factors relevant to protection behaviour in a large international sample. A previous study using this data focusing on intentional tanning has been published previously (14). The aims of the current paper were to determine and report on the prevalence of self-reported sun protection behaviours and severe sunburn experiences in users of the Internet; to identify the demographic, clinical and attitudinal/motivational determinants of sun protection behaviour; and to examine the association between sun protection behaviour and number of severe sunburn experiences over a one-year period.
METHOD
Study sample and recruitment
The sample was comprised of members of the Internet-using general population recruited between January 2007 and September 2008. Recruiting centres were located in 12 countries (Australia, Germany, Israel, Italy, Latvia, the Netherlands, Poland, Slovenia, Spain, Sweden, the UK and the USA) participating in the melanoma genetics consortium, GenoMEL. In each participating country, recruitment was encouraged by use of the Internet through e-mail `cascades' (using personal e-mail address lists, university lists, company lists, etc), and links placed on other health-related websites, as well as posted press releases (in conjunction with cancer charities, university press offices, national authorities responsible for UV radiation and/or public health issues) and paper flyers sent with regular mail. Potential participants were encouraged to visit the GenoMEL website (15), where they could find more information regarding the study, as well as the study questionnaire. Individuals aged < 16 years were advised to discuss their participation with an adult before completing the questionnaire. The study was approved by the relevant ethics institutions in each of the participating countries.
Questionnaire
A web-based questionnaire was developed for data collection via the GenoMEL website. The self-report questionnaire was purposely designed for the study in English, although many of the individual items have been used previously and tested for reliability (16, 17). Questionnaire translation was carried out by two independent bilingual professionals, and additionally tested for clarity and readability by a number of lay people. Efforts were made to ensure that the survey was as user-friendly as possible. A list of the questionnaire items can be obtained on request from GenoMEL (info@genomel.org). In addition to questions about age and gender, the questionnaire consisted of three major sections: epidemiologically established objective melanoma risk factors, behavioural risk factors, and motivational/attitudinal factors.
Objective risk factors were assessed via multiple-choice items eliciting data on hair colour (red/blonde/light brown/dark brown/black), freckling (none/a few/many), eye colour (blue/green/grey/green-grey/blue-grey/brown), skin colour (based on 7 pictures of hands with varying levels of pigmentation), skin type (Fitzpatrick's skin type classification; (18), personal and family history of melanoma (defined as one or more affected first-degree relatives), experience of severe sunburn (with blisters, or redness and pain lasting 2 days or more) before the age of 16 years (childhood sunburn is strongly related to adult sunburn, and a recent pooled meta-analysis of case-control studies showed a stronger association between childhood sunburn and melanoma incidence than adult sunburn (4)), and number of `large moles', defined as moles with a diameter larger than or equal to 6 mm or ¼ inch (none/1–2/3–5/6–10/more than 10). These items were used to calculate a risk factor score based on the total number of risk factors ranging from 0 to 9. The strategy of totalling the number of objective risk factors into one score is linked to our ambition to develop an Internet-based prevention tool in the future, to increase the use of sun protection. Although several of the risk factors both overlap and are not equally large contributors to melanoma risk, the score constitutes a straightforward approach of presenting objective risk factors to laymen. Two alternative ways of calculating a risk score was also explored e.g. a weighted melanoma risk calculation in line with what has been presented by Gantz el al. (19), and a calculation based on risk ratios derived from a pooled meta-analysis of case-control studies (4). Both these scales were highly correlated with the total number of risk factor score, both 0.76 (Spearman's Rho). All participants were asked to indicate were they currently lived, and based on their response they were categorised into five regions of residence, based on latitude. The categories were from high latitude to lower: Northern Europe between N55–69° (Sweden N55–69°, Latvia N56–58°), Northern/Central Europe between N49–59° (Germany N50–55°, Poland N49–55°, the UK N50–59°, the Netherlands N51–53.5°), Southern Europe/North USA between N36–50° (Spain N36–43.5°, Italy N38–47°, Slovenia N46.5–47°, the Northern states in USA N40–50°), West Asia/Southern USA/Southern Australia between N30–40° and S29–43° (Israel N30–35°, the Southern States in the USA N30–40°, the Southern and West states in Australia S29–43°), and Northern Australia between S10–29° (the northern states in Australia S10–29°).
Behavioural factors were assessed via items regarding sun exposure, severe sunburn, sun protective behaviours, and skin surveillance (i.e. skin self-examination and clinical skin examination). In this paper, we report on severe sunburn and sun protective behaviours only. To assess severe sunburn experiences, respondents were asked to indicate how many times (Never/Once/2–3 times/4–5 times/6–10 times/11 or more) they had experienced a severe sunburn in the past 12 months (defined as a painful redness of the skin caused by sun exposure or sun bed use) in a range of settings, including: at the beach, in the mountains, at a sports arena, in the garden/balcony, in the park, at work, at the beach in home country, at the beach abroad in a hot country, or when using a sun bed during the past year. A total score for frequency of severe sunburns was calculated by summing responses to all items. Respondents were also asked to indicate the proportion of time during which they used a range of sun protection measures when outdoors and in the sun, with six response options (Never – 0 % of the time; Rarely – 10 – 20 % of the time; Occasionally – 30 – 40 % of the time; About half of the time; Regularly – 60 – 80 % of the time; Always – 90 – 100 % of the time). Sun protection behaviours assessed were: use of sunscreen with a high sun protection factor (SPF 15 or more), sunscreen with a low sun protection factor (SPF less than 15), protective clothing, shade, and avoidance of midday sun. A composite score of total amount of sun protection was also created as an indication of adherence to recommended sun protection. This score was created by summing responses to all of the above mentioned items, with the exception of use of sunscreens with an SPF<15, and dividing the sum by the number of items included (i.e. four). In addition to this measure participants were categorized into three groups based on use of recommended sun protective behaviour. When constructing the categorization of sun protection behaviour we examined the association between use of each separate way of protection and sunburn. It became clear that a moderate use of protection was either associated with no or a small reduction in sunburn. Therefore our categorisation included those: infrequent or moderately protected, regularly protected, and consistently protected. Regularly protected was defined as those reporting Regular (60–80% of the time) use of at least one of the recommended ways to protect from the sun (i.e. Sunscreen SPF 15+, Clothes, Shade or Avoidance of midday sun), and Consistently protected were defined as those reporting Always (90–100%) using at least one of the recommended ways to protect from the sun (i.e. Sunscreen SPF 15+, Clothes, Shade or Avoidance of midday sun).
Motivational and attitudinal factors included perceived severity of melanoma (3 items, Cronbach coefficient alpha (α) = 0.68), perceived personal vulnerability to melanoma (2 items, α = 0.72), worry about melanoma (3 items, α = 0.67), perceived benefits of preventive behaviour (9 items, α = 0.81), and self-efficacy in terms of sun protection (one item). Participants responded to all items using a 5-point scale ranging from 0 to 4. In addition, a number of questions was asked about difficulties to perform sun related behaviours, in particular, three types of attitudes (i.e. barriers of or facilitators to) sun protection were assessed: perceived inconvenience of sun protection (11 items, α = 0.77), perceived impact of sun protection on ability to achieve a tan (3 items, α = 0.81), and use of sun protection as part of one's daily routine (6 items, α = 0.77). The questions were formulated as a statement, and respondents were to indicate to what degree they agree with this statement on a scale with five response alternatives (strongly disagree, disagree, neither disagree nor agree, agree, strongly agree). A total perceived barriers score (α = 0.85) was created by summing all three subscales (with the scale measuring having sun protection as a daily routine reversely coded). Attitudes towards level of tanning were assessed using five pictures of a man and five pictures of a woman with computer-altered level of tan, from very white skin to extreme darkly tanned skin. For both the man and the woman, the participants were asked to indicate which level of tan they perceived as `most attractive' and `most healthy', and responses to these four items were summed to produce a score measuring attitude towards suntans from negative to positive (α = 0.88).
Statistical analysis
A dichotomous sunburn variable was constructed as having had at least one severe sunburn versus no severe sunburn during the past 12 months. Logistic regression analyses were used to assess the association of different types and frequency of sun protection behaviours and sunburn reports. Odds ratio (OR) and 99% confidence intervals (CI) were presented (adjusted for age, gender, and skin type). Interaction effects for age, gender, skin type and total amount of recommended sun protection behaviour were also calculated.
Total sun protection behaviour was treated as a continuous outcome variable and linear regression analyses were used. Regression coefficients (β's) and proportion of variance explained (R2) were presented for the linear regression models. Analyses were done separately for those with and those without a previous melanoma. In these analyses, the explanatory variables were entered into the model in two steps. In step one, age, gender, latitude of residence, and number of risk factors were entered into the model. At step two, the following attitudinal/motivational correlates of sun protective behaviour were entered into the model: perceptions of vulnerability to melanoma, severity of melanoma, worry about developing melanoma, perceived benefits of sun protection, self-efficacy regarding the performance of protective behaviour, perceived barriers to prevention, and attitudes towards suntans.
All analyses were performed using SPSS version 16.0.
RESULTS
A total of 11,403 individuals initiated the online questionnaire, with 8,178 (72%) individuals successfully completing at least 80 percent of survey items. Seventy-three of the respondents were from Europe, 12% from Australia, 7% from the USA, 2% from Israel, and 6% from other countries. The majority of participants were women (73%, n=5,989), but the proportion varied substantially between countries (between 30% and 80%). Age ranged between 15 and 85 years, and the mean age of participants varied between 30.2 and 42.5 years in different countries. Seven percent of respondents had a personal history of melanoma and 8% had at least one first-degree relative with a previous melanoma. The mean number of risk factors was 4.2 (SD=1.8). Demographic characteristics and self-reported objective risk factors are presented in greater detail in Table 1.
Table 1.
Age, gender and objective melanoma risk factors distribution among the respondents.
| N | % | |
|---|---|---|
| Gender | ||
| Men | 2189 | 26.8 |
| Women | 5989 | 73.2 |
| Age | ||
| <25 | 1848 | 22.6 |
| 25–30 | 1322 | 16.2 |
| 31–40 | 2165 | 26.5 |
| 41–50 | 1402 | 17.1 |
| >50 | 1441 | 17.6 |
| Hair colour | ||
| Black/Brown | 6034 | 73.8 |
| Blond | 1739 | 21.3 |
| Red | 399 | 4.9 |
| Fitzpatrick skin type | ||
| I (%) | 405 | 5.0 |
| II (%) | 2302 | 28.2 |
| III (%) | 4914 | 60.1 |
| IV (%) | 550 | 6.7 |
| Presence of freckles | ||
| None | 3590 | 44.0 |
| A few | 3449 | 42.2 |
| Many | 1128 | 13.8 |
| Number of large moles (>6mm) | ||
| None | 1801 | 24.0 |
| 1–2 | 1231 | 16.4 |
| >=3 | 4477 | 59.6 |
| Sunburn before age 16 | ||
| Never | 1801 | 24.0 |
| 1–3 times | 4005 | 53.3 |
| Almost every summer | 1703 | 22.7 |
| Family history of melanoma | 656 | 8.0 |
| Previous melanoma | 557 | 6.8 |
| Total number of risk factors | ||
| 0–3 | 2639 | 35.3 |
| 4–5 | 3088 | 41.4 |
| >5 | 1739 | 23.3 |
Sunburn and sun protection behaviours
Figure 1 shows the estimated mean scores and 99% confidence intervals of total numbers of severe sunburns and total reported use of sun protection (i.e. sunscreen SPF 15+, clothes, shade and/or avoidance of midday sun) among respondents by country, adjusted for age, gender, skin type, hair colour, skin colour, eye colour, experience of severe sunburns before the age of 16 years, family history of melanoma, previous melanoma, degree of freckling and number of moles. There were statistically significant differences in sunburn frequency among the different countries (F12, 7219 = 16.43, p < 0.001), and pair-wise comparisons showed that respondents in Sweden reported significantly more sunburns than in all the other countries (P<0.001). Respondents in Latvia reported significantly more sunburns than respondents in the UK, the Netherlands, Italy, and the USA (p<0.001). Respondents in Poland reported significantly more sunburn than respondents in Italy (p<0.001).
Figure 1.
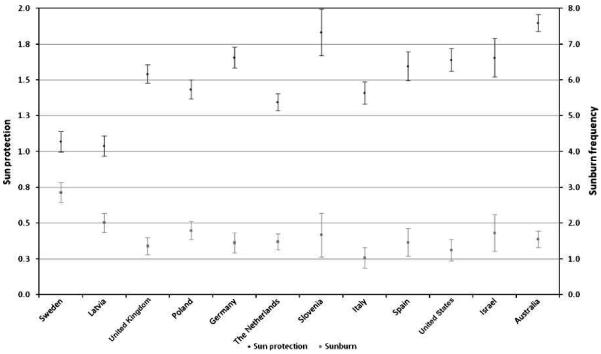
Means with 99% confidence intervals of frequency of severe sunburn (number of severe sunburns during past year) and total recommended sun protection score (min=0, max=4) in the different countries (means are corrected for age, gender, skin type, hair colour, skin colour, eye colour, family history of melanoma, own previous melanoma, experience of severe sunburns before the age of 16, and number of moles).
Half of all respondents reported at least one experience of severe sunburn during the past 12 months, and 76% of these reported more than one severe sunburn during the past 12 months. Severe sunburn was reported by more that half of the respondents with no previous history of melanoma (52%), somewhat less commonly by those with a family history of melanoma (47%, p<0.01), and least commonly by those with a previous melanoma (27%, p<0.001). Reported sunburn frequency decreased with increasing age, with 68% reporting sunburn during the past year among those less than 25 years old, 57% among those 25–30 years old, 47% among those 31–40 years old, 42% among those 41–50 years old, and 32% among those over 50 (p<0.001).
There were significant differences in total sun protection behaviour between the different countries (F12,7472 = 80.15, p < 0.001), and pair-wise comparisons showed a significantly lower degree of sun protective behaviours in Sweden and Latvia as compared to all other countries (P < 0.001). Australians reported the highest use of sun protection. Pair-wise comparisons showed significantly greater use of sun protection in Australia as compared to all other countries except Slovenia (P<0.001). A similar pattern was evident for the categorisation of participants based on total use of recommended sun protection, see Figure 2. Australia, the USA and Israel had the highest proportion of participants that reported consistent use of some sun protective behaviour. Lower proportion of recommended sun protection was reported from most European countries and the lowest proportion was reported from Sweden and Latvia.
Figure 2.
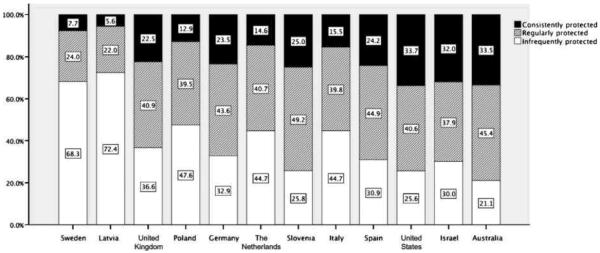
Proportion of respondents in the different countries reporting consistent, regular and infrequent use of recommended sun protective behaviour.
Sun protective behaviour and the likelihood of severe sunburn
Table 2 shows the association between each of the sun protection behaviours and severe sunburn, presented separately for those with and without a previous melanoma. Overall, reported moderate and regular use of protective clothing, shade and avoidance of midday sun significantly predicted lower reports of severe sunburn. Regular reported use of sunscreen with a SPF ≥ 15 was associated with lower likelihood of severe sunburn, compared with infrequent use. Moderate use of sunscreen with an SPF < 15 was associated with an increased likelihood of severe sunburn for those without or with a personal melanoma history. Participants with a previous melanoma reported a greater frequency of sun protection behaviour compared to those without a previous diagnosis (t = −19.25, p < 0.001); consequently, they were also less likely to have experienced severe sunburn (t = 7.69, p < 0.001).
Table 2.
Differences in use of sun protection between participants with or without a previous melanoma, and odds ratios for severe sunburn associated with use of each sun protection strategy.
| No previous melanoma (n=7621) | Previous melanoma (n=557) | ||||||
|---|---|---|---|---|---|---|---|
| Severe sunburn past year | Severe sunburn past year | ||||||
|
| |||||||
| N (%)a | % | OR (99% CI)b | N (%)a | % | OR (99% CI)b | ||
| Sunscreen SPF 15+ | Never/Rarely | 2924 (38.4) | 51.1 | 1 | 115 (20.6) | 31.3 | 1 |
| Occasionally/About half of the time | 1943 (25.5) | 56.1 | 1.15 (0.98–1.35) | 102 (18.3) | 38.1 | 1.29 (0.59–2.84) | |
| Regularly/Always | 2738 (36.0) | 48.7 | 0.83 (0.72–0.97)c | 340 (61.0) | 22.3 | 0.50 (0.25–0.97)c | |
| Sunscreen SPF <15 | Never/Rarely | 5086 (66.8) | 49.1 | 1 | 420 (75.4) | 24.1 | 1 |
| Occasionally/About half of the time | 1574 (20.7) | 57.7 | 1.42 (1.21–1.66)d | 75 (13.5) | 45.2 | 2.74 (1.35–5.54)d | |
| Regularly/Always | 950 (12.5) | 53.8 | 1.18 (0.98–1.43) | 62 (11.1) | 24.6 | 1.08 (0.47–2.51) | |
| Clothes | Never/Rarely | 4378 (57.6) | 54.7 | 1 | 196 (35.3) | 35.4 | 1 |
| Occasionally/About half of the time | 2105 (27.7) | 51.9 | 0.89 (0.77–1.02) | 176 (31.7) | 32.4 | 0.86 (0.47–1.55) | |
| Regularly/Always | 1122 (14.8) | 38.2 | 0.55 (0.46–0.67)d | 184 (33.1) | 13.2 | 0.29 (0.14–0.58)d | |
| Shade | Never/Rarely | 1929 (25.3) | 61.1 | 1 | 60 (10.8) | 44.6 | 1 |
| Occasionally/About half of the time | 3645 (47.9) | 53.5 | 0.69 (0.59–0.81)c | 214 (38.6) | 34.5 | 0.54 (0.24–1.24) | |
| Regularly/Always | 2036 (26.8) | 38.9 | 0.37 (0.31–0.44)c | 281 (50.6) | 17.7 | 0.21 (0.09–0.49)c | |
| Avoid midday sun | Never/Rarely | 3695 (48.5) | 56.3 | 1 | 139 (25.0) | 42.6 | 1 |
| Occasionally/About half of the time | 2421 (31.8) | 51.1 | 0.81 (0.70–0.94)d | 190 (34.1) | 25.1 | 0.40 (0.20–0.77)d | |
| Regularly/Always | 1498 (19.7) | 40.3 | 0.52 (0.44–0.62)d | 228 (40.9) | 19.6 | 0.29 (0.15–0.56)d | |
| Total use of Recommended Protection e | |||||||
| Infrequent or moderately protected | 3321 (43.6) | 58.7 | 1 | 101 (18.1) | 49.5 | 1 | |
| Regularly protected | 2910 (38.2) | 49.7 | 0.67 (0.58–0.77)d | 218 (39.1) | 28.5 | 0.38 (0.19–0.76)d | |
| Consistently protected | 1389 (18.2) | 38.1 | 0.40 (0.34–0.49)d | 238 (42.7) | 16.4 | 0.17 (0.08–0.36)d | |
Number of respondents reporting different level of use of ways to protect in the sun.
Odds Ratio (99% confidence interval) for having had a severe sunburn during the past year, analysis is controlled for age, gender & skin type.
Significant at p < 0.01
Significant at p < 0.001
Regularly protected was defined as those reporting Regular (60–80% of the time) use of at least one of the recommended ways to protect from the sun (i.e. Sunscreen SPF 15+, Clothes, Shade or Avoidance of midday sun), and Consistently protected were defined as those reporting Always (90–100%) using at least one of the recommended ways to protect from the sun (i.e. Sunscreen SPF 15+, Clothes, Shade or Avoidance of midday sun).
Total use of recommended protection showed a strong association with reduced risk of severe sunburn. Those who regularly and consistently protected themselves in the recommended way were much less likely to report getting a severe sunburn. Analyses of interaction effects between protective behaviour and age, gender, and skin type on severe sunburn, showed no interaction effect for gender and skin type. However, there was an interaction effect of protective behaviour and age, showing a reduction of severe sunburn prevalence with age (OR = 0.82 [for each standard deviation increase in age], 99% confidence intervals = 0.68 – 0.99, p < 0.01) among those who were consistently protected from the sun.
Associations between objective risk factors, sun protection, and attitudinal/motivational factors
Women reported more use of sun protection, greater perceived vulnerability, severity and worry about melanoma, but also higher perceived benefits of protection behaviour and less self-efficacy to protect than men (p<0.001 for all comparisons), see Table 3. Age was related to less sun protection, lower perceived vulnerability, severity and worry about melanoma, as well as lower perceived benefits with protection behaviour. A positive attitude towards suntans was negatively related to age, as were perceived barriers. Many of the objective risk factors were related to motivational/attitudinal factors so that those with a specific risk factor reported more use of sun protection, higher perceived vulnerability, severity, worry, benefits with protection behaviour, a less positive attitude towards suntans, and less barriers to sun protection. Self-efficacy to protect was not related to total number of risk factors, however, those with a previous melanoma, those who had not experienced any sunburn before the age of 16, and those with no large moles reported lower self-efficacy to protect.
Table 3.
Relationship between age, gender, and objective melanoma risk factors, sun protective behaviour and motivational/attitudinal factors (all scales range from 0 to 4).
| Total use of recommended sun protection | Perceived vulnerability | Perceived severity | Worry about developing a melanoma | Benefits of protection behaviour | Self-efficacy to protect | Attitude towards suntans | Barriers to sun protection | |
|---|---|---|---|---|---|---|---|---|
| Gender | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | n.s. |
| Men | 1.38 (0.76) | 2.03 (0.85) | 3.12 (0.62) | 2.69 (0.77) | 2.86 (0.61) | 2.43 (1.10) | 2.72 (0.76) | 1.79 (0.54) |
| Women | 1.51 (0.80) | 2.12 (0.83) | 3.25 (0.60) | 2.91 (0.69) | 2.99 (0.58) | 2.31 (1.10) | 2.78 (0.77) | 1.80 (0.56) |
| Age | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | p<0.001 | p<0.001 |
| <25 | 1.28 (0.74) | 2.00 (0.81) | 3.14 (0.61) | 2.85 (0.74) | 2.88 (0.62) | 2.30 (1.13) | 2.85 (0.77) | 2.02 (0.53) |
| 25–30 | 1.46 (0.78) | 2.05 (0.79) | 3.22 (0.58) | 2.88 (0.68) | 2.98 (0.57) | 2.37 (1.06) | 2.78 (0.74) | 1.82 (0.55) |
| 31–40 | 1.52 (0.78) | 2.14 (0.83) | 3.22 (0.60) | 2.90 (0.70) | 2.99 (0.57) | 2.36 (1.09) | 2.78 (0.73) | 1.77 (0.55) |
| 41–50 | 1.59 (0.82) | 2.18 (0.88) | 3.27 (0.61) | 2.85 (0.75) | 2.99 (0.59) | 2.40 (1.12) | 2.73 (0.81) | 1.69 (0.53) |
| >50 | 1.57 (0.83) | 2.13 (0.86) | 3.24 (0.62) | 2.77 (0.74) | 2.93 (0.58) | 2.13 (1.11) | 2.63 (0.78) | 1.65 (0.53) |
| p<0.001 | p<0.001 | p<0.001 | n.s. | n.s. | n.s. | p<0.001 | n.s. | |
| Hair colour | ||||||||
| Black/Brown | 1.45 (0.79) | 2.04 (0.82) | 3.20 (0.61) | 2.84 (0.72) | 2.95 (0.59) | 2.34 (1.11) | 2.51 (0.66) | 1.80 (0.55) |
| Blond/Red | 1.57 (0.80) | 2.27 (0.86) | 3.26 (0.61) | 2.89 (0.74) | 2.98 (0.59) | 2.35 (1.08) | 2.44 (0.68) | 1.79 (0.56) |
| Fitzpatrick skin type | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | p<0.001 | p<0.001 |
| III/IV | 1.32 (0.74) | 1.95 (0.78) | 3.18 (0.61) | 2.79 (0.72) | 2.91 (0.60) | 2.34 (1.10) | 2.59 (0.62) | 1.85 (0.54) |
| I/II | 1.80 (0.81) | 2.39 (0.87) | 3.28 (0.59) | 2.98 (0.71) | 3.05 (0.55) | 2.35 (1.10) | 2.28 (0.71) | 1.70 (0.57) |
| Presence of freckles | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | p<0.001 | p<0.001 |
| None | 1.32 (0.76) | 1.91 (0.79) | 3.17 (0.61) | 2.73 (0.74) | 2.88 (0.61) | 2.37 (1.11) | 2.56 (0.64) | 1.83 (0.55) |
| A few/Many | 1.60 (0.79) | 2.25 (0.84) | 3.25 (0.60) | 2.95 (0.69) | 3.01 (0.56) | 2.33 (1.09) | 2.43 (0.68) | 1.77 (0.55) |
| Sunburn before age 16 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. |
| Never | 1.32 (0.77) | 1.78 (0.79) | 3.13 (0.62) | 2.68 (0.74) | 2.85 (0.61) | 2.24 (1.14) | 2.57 (0.63) | 1.81 (0.55) |
| 1–3 times | 1.51 (0.78) | 2.08 (0.80) | 3.22 (0.60) | 2.87 (0.70) | 2.97 (0.57) | 2.42 (1.07) | 2.46 (0.65) | 1.78 (0.56) |
| Almost every summer | 1.62 (0.83) | 2.49 (0.83) | 3.31 (0.59) | 3.01 (0.73) | 3.04 (0.59) | 2.31 (1.12) | 2.44 (0.73) | 1.80 (0.58) |
| Number of large mole (>6mm) | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. |
| None | 1.32 (0.77) | 1.78 (0.79) | 3.13 (0.62) | 2.68 (0.74) | 2.85 (0.61) | 2.24 (1.14) | 2.57 (0.63) | 1.81 (0.55) |
| 1–2 | 1.44 (0.77) | 1.93 (0.75) | 3.17 (0.61) | 2.81 (0.68) | 2.90 (0.57) | 2.37 (1.10) | 2.48 (0.64) | 1.78 (0.56) |
| >=3 | 1.57 (0.80) | 2.27 (0.83) | 3.27 (0.60) | 2.94 (0.72) | 3.20 (0.58) | 2.39 (1.09) | 2.45 (0.69) | 1.79 (0.56) |
| Family history of melanoma | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | p<0.001 | p<0.001 |
| No | 1.45 (0.78) | 2.04 (0.81) | 3.20 (0.61) | 2.82 (0.72) | 2.94 (0.59) | 2.35 (1.10) | 2.50 (0.66) | 1.81 (0.55) |
| Yes | 1.80 (0.82) | 2.82 (0.78) | 3.44 (0.57) | 3.21 (0.69) | 3.10 (0.55) | 2.25 (1.07) | 2.33 (0.69) | 1.68 (0.58) |
| Previous melanoma | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 |
| No | 1.43 (0.77) | 2.00 (0.77) | 3.20 (0.61) | 2.81 (0.71) | 2.95 (0.59) | 2.36 (1.09) | 2.51 (0.65) | 1.81 (0.55) |
| Yes | 2.09 (0.84) | 3.41 (0.57) | 3.49 (0.56) | 3.48 (0.65) | 3.06 (0.57) | 2.14 (1.27) | 2.28 (0.78) | 1.56 (0.55) |
| Total number of risk factors | p<0.001 | p<0.001 | p<0.001 | p<0.001 | p<0.001 | n.s. | p<0.001 | p<0.001 |
| 0–3 | 1.27 (0.74) | 1.76 (0.73) | 3.14 (0.62) | 2.71 (0.74) | 2.86 (0.62) | 2.32 (1.12) | 2.62 (0.62) | 1.85 (0.55) |
| 4–5 | 1.48 (0.77) | 2.08 (0.77) | 3.22 (0.60) | 2.85 (0.69) | 2.98 (0.57) | 2.39 (1.09) | 2.47 (0.66) | 1.81 (0.54) |
| >5 | 1.84 (0.81) | 2.64 (0.83) | 3.33 (0.58) | 3.09 (0.70) | 3.06 (0.55) | 2.33 (1.10) | 2.30 (0.71) | 1.70 (0.58) |
Correlates of Sun Protection Behaviours
Means and standard deviations for the motivational and attitudinal variables and Spearman's correlation coefficient for pairs of variables are presented in Table 4. Perceived vulnerability to melanoma, perceived melanoma severity, and worry about melanoma showed moderate correlations with sun protection behaviour (correlations ranged from 0.16 to 0.20), and perceived barriers to protection showed a strong negative correlation (–0.56) with total reported sun protection.
Table 4.
Mean values and standard deviations for total sun protection behaviour and motivational factors for sun protection, and correlations between the variables (all scales have a range from 0 to 4).
| Mean | SD | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 8a | 8b | 8c | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Total use of recommended sun protection | 1.48 | 0.79 | 0.20** | 0.16** | 0.18** | 0.32** | 0.16** | −0.37** | −0.56** | −0.47** | −0.40** | 0.52** |
| 2 Perceived vulnerability | 2.10 | 0.83 | 0.21** | 0.47** | 0.14** | 0.00 | −0.07** | −0.05** | −0.02 | −0.07** | 0.07** | |
| 3 Perceived severity | 3.22 | 0.61 | 0.34** | 0.26** | 0.10** | −0.08** | −0.08** | −0.06** | −0.11** | 0.06** | ||
| 4 Worry about developing a melanoma | 2.85 | 0.72 | 0.24** | 0.04* | 0.03* | −0.03* | −0.01 | −0.02 | 0.07** | |||
| 5 Benefits of protection behaviour | 2.95 | 0.59 | 0.29** | −0.15** | −0.21** | −0.19** | −0.14** | 0.18** | ||||
| 6 Perceived self-efficacy to protect | 2.35 | 1.10 | −0.06** | −0.20** | −0.20** | −0.12** | 0.15** | |||||
| 7 Attitude towards suntans | 2.49 | 0.67 | 0.31** | 0.24** | 0.34** | −0.23** | ||||||
| 8 Barriers to sun protection | 1.80 | 0.55 | 0.93** | 0.62** | −0.83** | |||||||
| a Perceiving use of sun protection as inconvenient | 1.72 | 0.59 | 0.42** | −0.68** | ||||||||
| b Perceiving sun protection as problematic as it reduces the possibility to develop a suntan | 1.69 | 0.94 | −0.35** | |||||||||
| c Having sun protection as a part of one's daily routine | 2.01 | 0.62 |
= P < 0.01
= P < 0.001
Two separate hierarchical linear regression analyses were conducted for those with and those without a previous melanoma (Table 5). The full model explained 29% of the variance in sun protection behaviour among those with a previous melanoma and 45% among those with no previous melanoma. Gender was significantly related to sun protection with women reporting a higher degree of protection than men. For those with no previous melanoma, age was positively associated with sun protection. Latitude and number of risk factors were also associated with sun protection behaviour among those without a previous melanoma. People from lower latitudes and those with a higher number of risk factors reported protecting themselves more than those from higher latitudes and those with lower number of risk factors.
Table 5.
Regression analysis showing associations between demographic, clinical, attitudinal/motivational factors, and sun protection behaviour.
| Standardised betas | |||
|---|---|---|---|
| Previous Melanoma | Step 1 | Step 2 | |
| Step 1 Demographic and clinical factors | Age | 0.05 | −0.02 |
| Gender (men=1, women=2) | 0.19** | 0.14* | |
| Number of melanoma risk factors | 0.14* | 0.08 | |
| Latitude of residence (increasing value with increased proximity to the equator) | 0.08 | 0.03 | |
| Step 2 Attitudinal/motivational factors | Perceived vulnerability | 0.04 | |
| Perceived severity | 0.08 | ||
| Worry about developing a melanoma | 0.10 | ||
| Benefits of protection behaviour | 0.03 | ||
| Perceived self-efficacy to protect | 0.05 | ||
| Barriers of or facilitators to sun protectiona | −0.37** | ||
| Attitude towards suntans | −0.14* | ||
| R2 | 0.07 ** | 0.29 ** | |
| R2 change | 0.22** | ||
| No Previous Melanoma | |||
| Step 1 Demographic and clinical factors | Age | 0.10** | 0.01 |
| Gender (men=1, women=2) | 0.06** | 0.04** | |
| Number of melanoma risk factors | 0.21** | 0.13** | |
| Latitude of residence (increasing value with increased proximity to the equator) | 0.31** | 0.13** | |
| Step 2 Attitudinal/motivational factors | Perceived vulnerability | 0.006 | |
| Perceived severity | −0.005 | ||
| Worry about developing a melanoma | 0.04* | ||
| Benefits of protection behaviour | 0.14** | ||
| Perceived self-efficacy to protect | 0.01 | ||
| Barriers of or facilitators to sun protectiona | −0.44** | ||
| Attitude towards suntans | −0.16** | ||
| R2 | 0.16 ** | 0.45 ** | |
| R2 change | 0.29** | ||
Initially, each of the subscales measuring barriers to sun protection was entered into the model at the fourth step, but due to collinearity the total score measuring barriers/facilitators was used in the final model;
= p < 0.01
= p < 0.001.
The strongest predictor of sun protection behaviour was perceived barriers to protection and a positive attitude towards suntans. For respondents with no previous melanoma, perceived benefits of protection behaviour, and to a weaker extent worry about developing a melanoma, were also associated with sun protection behaviour.
Differences in associations between attitudinal/motivational factors and sun protection in countries of different latitude
Five separate planned regression analyses among participants without a previous melanoma were conducted to examine differences in predictors of sun protection behaviour in regions at different latitudes. The pattern of results was similar across regions and the same variables were significant predictors in all of the regions; however, the regression coefficients varied slightly. The association between perceived barriers and sun protection was strongest in USA and Australia (β=−0.50), and lowest in Northern Europe (β=−0.42). The association between a positive attitude towards tans and reduced sun protection was strongest in Northern Europe (β=−0.22) and lowest in USA (β=−0.12). The association between perceived benefits of sun protection and sun protection behaviour was strongest in USA (β=0.18) and lowest in Australia (β=0.13) and Northern Europe (β=0.14).
DISCUSSION
Internet-based interventions in medical settings have been shown to improve knowledge and minimise distress responses (20). Online information services remove geographic barriers, and there are a growing number of studies supporting the use of Internet resources to promote health behaviour change (20, 21). This study focused on a sample of Internet users because this population is the target group for a planned preventative intervention. This study showed that it was possible to target a high proportion of individuals with behavioural risk factors for melanoma using the Internet. Half of all respondents reported at least one experience of severe sunburn during the past 12 months and thus reported behaviours associated with an increased risk of melanoma. Severe sunburn was common even in melanoma patients as more than 27% of individuals with a previous melanoma diagnosis reported at least one severe sunburn in the past year. Although participants reported the adoption of sun protection measures, the frequency or thoroughness of protection was evidently insufficient to avoid severe sunburn.
In this study, we analysed correlates to sun protection behaviour, and the study showed that women were more likely to report sun protection behaviour than men and this association was stronger for those with a previous melanoma that for those without such experience. Among respondents with no previous melanoma, age was positively related to reported sun protection behaviour. However, this association was not significant when attitudinal/motivational variables were also included in the analysis. Several previous studies have found gender differences in sun protective behaviour, with women reporting more protection than men (for a review, please see Kasparian et al. (22)). Several studies have also found a decreasing use of sun protection with age, i.e. from childhood up to young adulthood (23–26), and then an increase of protection with age among adults (27, 28).
The factors most strongly associated with reduced sun protection were perceived barriers to sun protection and a positive view of suntans. Both factors predicted sun protection behaviour when demographic and clinical factors were statistically controlled, and they were significant predictors of sun protection behaviour both in participants with and without a previous melanoma. Perceiving sun protection as beneficial and something that reduce the risk of skin cancer was also related to increased use of protection. However, perceived vulnerability to melanoma, perceived melanoma severity, and worry about melanoma were less related to self-reported sun protection behaviour. The weak relations between risk perceptions and related concepts to concurrent reports of sun protection behaviour are somewhat surprising and contrary to some previous findings (29, 30), as well as being inconsistent with health behaviour models in general. But these findings were consistent across regions. In summary, our results suggest that targeting barriers (i.e. perceived inconvenience and preference to acquire a tan) and strengthening facilitators (i.e. having sun protection as part of the daily routine) would be the most important ways to promote sun protection. The data also suggest that it is important to influence the positive views of suntans. These attitudes might be difficult to change, but some studies focusing on information concerning personalised risks and risks related to appearance have shown promising results in changing people's intentions to tan and protect in the sun (31–35).
In the analysis, the proportion of explained variance was higher among those without a previous melanoma (45%) than for those with a previous melanoma diagnosis (29%). This might be due to the fact that the motivational/attitudinal variables used in the study were derived from theories regarding health behaviours, such as HBM and PMT, primarily developed to explain health behaviours in the general population and not the behaviour of specific groups of patients. It is most likely, that these models need to be refined and expanded to better explain the behaviours of individuals with the experience of a specific disease. Despite the difference in explained variance there were striking similarities between those with and those without a previous melanoma diagnosis, as both perceived barriers and attitude towards suntans were important correlates to sun protection.
Overall, sun protection was negatively associated with severe sunburn experiences, at least when using recommended ways to protect. Our findings give support for continued emphasis on clothing, the use of shaded areas, and avoidance of midday sun as the best ways to lower the risk of severe sunburns. Sunscreen was the most frequently reported way of protecting one's skin from damage caused by the sun, even though sunscreen in general is only recommended as a complement to other forms of protection (36). Our findings indicate that sunscreen is not always used in combination with other forms of protection, which may explain the low degree of reduction in sunburns associated with the use of sunscreen. Reported use of sunscreen with SPF <15 appeared to be related to an increased likelihood of sunburn. Several studies have found a positive association between sunscreen use and time spent in the sun, sometimes called the sunscreen paradox (37, 38). Instead of using sunscreen as a complement to other means of avoiding excessive sun exposure, sunscreens are often used to extend time spent in the sun. Further, sunscreen use on children has been linked to a higher number of melanocytic nevi, indicating a higher degree of sun exposure among children using sunscreens (39). Some studies have also found an increased risk of skin cancer among sunscreen users (40), although the overall epidemiological data does not support such an association (41). One possible reason for the use of sunscreens to increase time spent in the sun could be that some people try to acquire a “safe” suntan; that is, people may want to experience a certain level of sun exposure and acquire a suntan, but at the same time try to avoid getting sunburnt. Having these double goals may lead to insufficient use of sun protection and unwanted sunburns. Thus, it appears critical that future skin cancer prevention campaigns and public health education messages highlight the sunscreen paradox, and emphasise the importance of thorough and frequent applications of sunscreen (in addition to other forms of sun protection) when outdoors and in the sun for extended periods of time.
Respondents with a previous melanoma were less likely to have experienced severe sunburn and more likely to report sun protective behaviour. They were also more successful in their use of sun protection, as reported use of sun protection was more strongly related to reduced likelihood of sunburn among those with a previous melanoma. The association between motivational factors and sun protective behaviour was, however, very similar to those reported by participants without a previous melanoma.
Study strengths and limitations
One of the key strengths of the present study was the innovative use of the Internet and an online survey designed to reach a large number of people across a wide range of geographical locations. The translation of the study questionnaire into 10 different languages also increased study accessibility. The study, however, is not without limitations. Due to the varying recruitment strategies used in different countries, conclusions regarding actual population differences should be made with great caution. The differences in severe sunburn frequency in different regions, with higher frequencies of reported severe sunburn in countries with weaker ambient UV radiation, could reflect an actual difference between countries but might also be an effect of selection bias. The same is true about the finding regarding country difference in frequency of reported sun protection behaviour. It was highest in countries with a high degree of ambient UV radiation (e.g., Australia), and lowest in countries with lower UV radiation (e.g., Sweden and Latvia). Also, between 30% and 89% of survey respondents in each country were women, and the mean age of participants in different regions varied between 30.2 and 42.5 years, indicating that the study is based on a fairly young population and with substantial gender variability between countries. The relatively large proportion of individuals with a personal experience of melanoma indicates that this type of recruitment strategy generated a significant number of participants interested in and/or concerned about skin cancer-related issues. These facts also indicate a substantial self-selection bias in the sample. Further, we did not ask whether or not the participants had reviewed the educational material provided on the GenoMEL website which could potentially have influenced the answers given.
A further limitation in the study was that the questionnaire used, and the many different language version, was not tested for reliability before the study. However, many of the items had been used previously and have shown adequate reliability in previous studies. A study using a Swedish sample, found fair to good test-retest agreement for both sun related behavioural questions and motivational/attitudinal variables (16). Finally, as this is a cross-sectional study, it is not possible to draw conclusions regarding causal pathways among attitudinal/motivational variables, and reported behaviour (42, 43). It does, however, give some indication about the type of beliefs that it may be beneficial to target and try to change in a melanoma prevention intervention on the Internet, a major aim of the study.
Conclusion
A substantial proportion of the study participants in different locations around the world reported experiencing severe sunburn, indicating excessive exposure to UV radiation that put them at increased risk of skin cancer. Even among people with a previous melanoma, a substantial proportion reported severe sunburn. This study suggests a number of potential avenues for behaviour change that might lead to reductions in sunburn and thus, possibly, melanoma incidence. The results also suggest that interventions intended to reduce melanoma incidence could be more efficient if focused on reduction of barriers to protection, emphasis on the benefits of protection, and inclusion of strategies to change positive views of suntans. This study demonstrates that it is possible to reach respondents with both objective and behavioural risk factors for melanoma trough the internet, and it give information regarding factors to consider in the development of a internet-based melanoma prevention tool.
ACKNOWLEDGEMENTS
New Knowledge Directorate Ltd (www.nkd.org.uk) designed and implemented the web interface and supporting database. The study was funded by the European Commission under the 6th Framework Programme, Contract Nr: LSHC-CT-2006-018702. Richard Bränström is funded by research grants from the Swedish Council for Working Life and Social Research (Nr: 2006-1264 and 2006-0069) and Center for Health Care Science at the Karolinska Institutet, Sweden (Nr: 2008-4737). Nadine Kasparian is supported by a Post Doctoral Clinical Research Fellowship from the National Health and Medical Research Council of Australia (NH&MRC, ID 510399). Julia Newton Bishop is funded by Cancer Research UK Programme grant C588/A4994. Francisco Cuellar was funded by a scholarship (152256/158706) from CONACYT, Mexico. We would also like to thank the following people who have made a significant contribution to the completion of this study; Karolinska Institutet: Katja Brandberg, Ryan Locke; University of Leeds: Faye Elliott; Leiden University Medical Centre: Clasine van der Drift, Frans A. van Nieuwpoort, Coby Out, Femke de Snoo; University of Pennsylvania: Patricia Van Belle, David Elder, Jillian Knorr, Althea Ruffin; University of Utah: Samantha Leaf.
REFERENCES
- 1.Lens MB, Dawes M. Global perspectives of contemporary epidemiological trends of cutaneous malignant melanoma. Br J Dermatol. 2004;150:179–85. doi: 10.1111/j.1365-2133.2004.05708.x. [DOI] [PubMed] [Google Scholar]
- 2.Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 2005;41:45–60. doi: 10.1016/j.ejca.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 3.Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63:8–18. doi: 10.1016/s1011-1344(01)00198-1. [DOI] [PubMed] [Google Scholar]
- 4.Chang YM, Barrett JH, Bishop DT, et al. Sun exposure and melanoma risk at different latitudes: a pooled analysis of 5700 cases and 7216 controls. Int J Epidemiol. 2009;38:814–30. doi: 10.1093/ije/dyp166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ibrahim SF, Brown MD. Tanning and cutaneous malignancy. Dermatol Surg. 2008;34:460–74. doi: 10.1111/j.1524-4725.2007.34092.x. [DOI] [PubMed] [Google Scholar]
- 6.Banks BA, Silverman RA, Schwartz RH, Tunnessen WW. Attitudes of teenagers towards sun exposure and sunscreen use. Pediatrics. 1992;89:40–2. [PubMed] [Google Scholar]
- 7.Mermelstein RJ, Riesenberg LA. Changing knowledge and attitudes about skin cancer risk factors in adolescents. Health Psychol. 1992;11:371–6. doi: 10.1037//0278-6133.11.6.371. [DOI] [PubMed] [Google Scholar]
- 8.Geller AC, Colditz G, Oliveria S, et al. Use of sunscreen, sunburning rates, and tanning bed use among more than 10 000 US children and adolescents. Pediatrics. 2002;109:1009–14. doi: 10.1542/peds.109.6.1009. [DOI] [PubMed] [Google Scholar]
- 9.Wichstrøm L. Predictors of Norwegian adolescents' sunbathing and use of suncreen. Health Psychol. 1994;13:412–20. [PubMed] [Google Scholar]
- 10.Campbell HS, Birdsell JM. Knowledge, beliefs, and sun protection behaviors of Alberta Adults. Preventive Medicine. 1994;23:160–6. doi: 10.1006/pmed.1994.1022. [DOI] [PubMed] [Google Scholar]
- 11.Janz NK, Becker Mh. The health belief model: a decade later. Health Education Quarterly. 1984;11:1–47. doi: 10.1177/109019818401100101. [DOI] [PubMed] [Google Scholar]
- 12.Rodgers RW. A protection motivation theory of fear appeals and attitude change. The Journal of Psychology. 1975;91:93–114. doi: 10.1080/00223980.1975.9915803. [DOI] [PubMed] [Google Scholar]
- 13.Ogden J. Health beliefs. Health beliefs. Open University Press; Buckingham: 1996. [Google Scholar]
- 14.Branstrom R, Chang YM, Kasparian N, et al. Melanoma risk factors, perceived threat and intentional tanning: an international online survey. Eur J Cancer Prev. 2010;19:216–26. doi: 10.1097/CEJ.0b013e3283354847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.GenoMEL - The Melanoma Genetics Consortium. 2010 cited; Available from: http://www.genomel.org.
- 16.Branstrom R, Kristjansson S, Ullen H, Brandberg Y. Stability of questionnaire items measuring behaviours, attitudes and stages of change related to sun exposure. Melanoma Res. 2002;12:513–9. doi: 10.1097/00008390-200209000-00014. [DOI] [PubMed] [Google Scholar]
- 17.Veierod MB, Parr CL, Lund E, Hjartaker A. Reproducibility of self-reported melanoma risk factors in a large cohort study of Norwegian women. Melanoma Res. 2008;18:1–9. doi: 10.1097/CMR.0b013e3282f120d2. [DOI] [PubMed] [Google Scholar]
- 18.Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Archives of Dermatology. 1988;124:869–71. doi: 10.1001/archderm.124.6.869. [DOI] [PubMed] [Google Scholar]
- 19.Glanz K, Schoenfeld E, Weinstock MA, Layi G, Kidd J, Shigaki DM. Development and reliability of a brief skin cancer risk assessment tool. Cancer Detect Prev. 2003;27:311–5. doi: 10.1016/s0361-090x(03)00094-1. [DOI] [PubMed] [Google Scholar]
- 20.Salem D, Bogat A, Reid C. Mutual help goes on-line. Journal of Community Psychology. 1997;25:189–207. [Google Scholar]
- 21.Lustria ML, Cortese J, Noar SM, Glueckauf RL. Computer-tailored health interventions delivered over the Web: review and analysis of key components. Patient Educ Couns. 2009;74:156–73. doi: 10.1016/j.pec.2008.08.023. [DOI] [PubMed] [Google Scholar]
- 22.Kasparian N, McLoone J, Meiser B. Skin cancer-related prevention and screening behaviors: A review of the literature. Journal of Behavioral Medicine. 2009;32:406–28. doi: 10.1007/s10865-009-9219-2. [DOI] [PubMed] [Google Scholar]
- 23.Bränström R, Brandberg Y, Holm L-E, Sjöberg L, Ullén H. Beliefs, knowledge and attitudes as predictors of sunbathing habits and use of sun protection among Swedish adolescents. European Journal of Cancer Prevention. 2001;10:337–45. doi: 10.1097/00008469-200108000-00007. [DOI] [PubMed] [Google Scholar]
- 24.Balanda KP, Stanton WR, Lowe JB, Purdie J. Predictors of sun protective behaviors among school students. Behavioral Medicine. 1999;25:28–35. doi: 10.1080/08964289909596736. [DOI] [PubMed] [Google Scholar]
- 25.Coogan PF, Geller A, Adams M, Benjes LS, Koh HK. Sun protection practices in preadolescents and adolescents: a school-based survey of almost 25,000 Connecticut schoolchildren. J Am Acad Dermatol. 2001;44:512–9. doi: 10.1067/mjd.2001.111621. [DOI] [PubMed] [Google Scholar]
- 26.Severi G, Cattaruzza MS, Baglietto L, et al. Sun exposure and sun protection in young European children: an EORTC multicentric study. Eur J Cancer. 2002;38:820–6. doi: 10.1016/s0959-8049(02)00015-1. [DOI] [PubMed] [Google Scholar]
- 27.Koh HK, Bak SM, Geller AC, et al. Sunbathing habits and sunscreen use among white adults: results of a national survey. American Journal of Public Health. 1997;87:1214–7. doi: 10.2105/ajph.87.7.1214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Coups EJ, Manne SL, Heckman CJ. Multiple skin cancer risk behaviors in the U.S. population. Am J Prev Med. 2008;34:87–93. doi: 10.1016/j.amepre.2007.09.032. [DOI] [PubMed] [Google Scholar]
- 29.Grunfeld EA. What influences university students' intentions to practice safe sun exposure behaviors? J Adolesc Health. 2004;35:486–92. doi: 10.1016/j.jadohealth.2003.11.093. [DOI] [PubMed] [Google Scholar]
- 30.Jackson KM, Aiken LS. A psychosocial model of sun protection and sunbathing in young women: the impact of health beliefs, attitudes, norms, and self-efficacy for sun protection. Heath psych. 2000;19:469–78. doi: 10.1037//0278-6133.19.5.469. [DOI] [PubMed] [Google Scholar]
- 31.Olson AL, Gaffney CA, Starr P, Dietrich AJ. The impact of an appearance-based educational intervention on adolescent intention to use sunscreen. Health Educ Res. 2008;23:763–9. doi: 10.1093/her/cym005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mahler HI, Kulik JA, Gerrard M, Gibbons FX. Long-term effects of appearance-based interventions on sun protection behaviors. Health Psychol. 2007;26:350–60. doi: 10.1037/0278-6133.26.3.350. [DOI] [PubMed] [Google Scholar]
- 33.Mahler HI, Kulik JA, Harrell J, Correa A, Gibbons FX, Gerrard M. Effects of UV photographs, photoaging information, and use of sunless tanning lotion on sun protection behaviors. Arch Dermatol. 2005;141:373–80. doi: 10.1001/archderm.141.3.373. [DOI] [PubMed] [Google Scholar]
- 34.Hillhouse JJ, Turrisi R. Examination of the efficacy of an appearance-focused intervention to reduce UV exposure. J Behav Med. 2002;25:395–409. doi: 10.1023/a:1015870516460. [DOI] [PubMed] [Google Scholar]
- 35.Hillhouse J, Turrisi R, Stapleton J, Robinson J. A randomized controlled trial of an appearance-focused intervention to prevent skin cancer. Cancer. 2008;113:3257–66. doi: 10.1002/cncr.23922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.World Health Organisation Sun protection - simple precautions in the sun. 2010 cited; Available from: http://www.who.int/uv/sun_protection/en/
- 37.McCarthy EM, Ethridge KP, Wagner RF. Beach holiday sunburn: the sunscreen paradox and gender differences. Cutis. 1999;64:37–42. [PubMed] [Google Scholar]
- 38.Autier P, Doré J-F, Négrier S, et al. Sunscreen use and duration of sun exposure: a double-blind, randomized trial. Journal of the National Cancer Institute. 1999;91:1304–9. doi: 10.1093/jnci/91.15.1304. [DOI] [PubMed] [Google Scholar]
- 39.Autier P, Dore JF, Cattaruzza MS, et al. Sunscreen use, wearing clothes, and number of nevi in 6- to 7-year-old European children. European Organization for Research and Treatment of Cancer Melanoma Cooperative Group. J Natl Cancer Inst. 1998;90:1873–80. doi: 10.1093/jnci/90.24.1873. [DOI] [PubMed] [Google Scholar]
- 40.Westerdahl J, Ingvar C, Masback A, Olsson H. Sunscreen use and malignant melanoma. Int J Cancer. 2000;87:145–50. doi: 10.1002/1097-0215(20000701)87:1<145::aid-ijc22>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 41.Huncharek M, Kupelnick B. Use of topical sunscreens and the risk of malignant melanoma: a meta-analysis of 9067 patients from 11 case-control studies. American Journal of Public Health. 2002;92:1173–7. doi: 10.2105/ajph.92.7.1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Brewer NT, Weinstein ND, Cuite CL, Herrington JE. Risk perceptions and their relation to risk behavior. Ann Behav Med. 2004;27:125–30. doi: 10.1207/s15324796abm2702_7. [DOI] [PubMed] [Google Scholar]
- 43.Weinstein ND, Nicolich M. Correct and incorrect interpretations of correlations between risk perceptions and risk behaviors. Health Psychol. 1993;12:235–45. doi: 10.1037//0278-6133.12.3.235. [DOI] [PubMed] [Google Scholar]