

Abstract
INTRODUCTION:
Surgery has the potential to remove the entire hydatid cyst and can lead to complete cure. Presence of hydatid cysts in multiple abdominal organs imposes special challenges for laparoscopic management. The patient position and port placement for one organ may not be adequate for other and proper exposure in hydatid cyst is of paramount importance to prevent spillage and complete removal of the cyst. Single incision multi-trocar technique has a unique advantage of allowing surgeon to work in different quadrants of abdomen using the same incision and ports. We report in this paper the first Laparo-endoscopic single-site hepatic cyst excision with partial splenectomy for hydatid cyst in liver and spleen using conventional laparoscopic instruments.
PATIENT AND TECHNIQUE:
The procedure was performed on a 64 year old female diagnosed to have Hydatid cyst in segment VIII of liver and another cyst in lower pole of spleen a transverse 3 cm incision was made 6 cm above umbilicus and was deepened up to fascia. Two 10mm and one 5mm ports were inserted. Procedure was completed in 160 minutes without any intra-operative complication. There were no post-operative complication and patient was discharged on day 5.
CONCLUSION:
Single incision multi-trocar surgery has cosmetic advantage over standard laparoscopic approach. It is even more marked when two procedures are combined in different quadrants of abdomen. As this is a rare combination procedure so it remains to be determined if this technique offers additional advantages of decreased analgesia, decreased hospital stay or cost effectiveness.
Keywords: Hydatid cyst, hydatid disease of spleen, partial splenectomy, single incision multi-trocar surgery, single incision surgery
INTRODUCTION
Surgery has the potential to remove the entire hydatid cyst and can lead to complete cure.[1,2] In simple, accessible cyst, surgery can be successfully performed in up to 90% of patients. Author and others have already shown that laparoscopic approach for uncomplicated hydatid cysts of the liver is a safe and effective option with favourable long-term results.[3–5] Laparoscopic partial splenectomy can be done to treat splenic hydatid cysts while preserving splenic immunologic functions and causing less pain and better cosmetic results.[6]
Presence of hydatid cysts in multiple abdominal organs imposes special challenges for laparoscopic management. The patient position and port placement for one organ may not be adequate for the other and proper exposure in hydatid cyst is of paramount importance to prevent spillage and complete removal of the cyst. Single incision multi-trocar technique has a unique advantage of allowing surgeon to work in different quadrants of abdomen using the same incision and ports.
We report in this paper the first Laparo-endoscopic single-site hepatic cyst excision with partial splenectomy for hydatid cyst in liver and spleen using conventional laparoscopic instruments.
PATIENT AND TECHNIQUE
A 64-year-old female presented to us with complaint of abdominal pain for 2 months. She had no co-morbidities. Computed tomography (CT) scan of abdomen showed hydatid cyst (4.7 × 5.1 cm) in segment VIII of liver and another cyst (6.3 × 7.6 cm) in lower pole of spleen [Figure 1]. She was started on Albendazole 800 mg BD 3 days prior to surgery. Vaccination against Pneumococcus and Haemophilus influenza B was given keeping in mind the possibility of total splenectomy. Single incision multi-trocar hepatic cyst excision with partial splenectomy was planned for her and informed consent was obtained.
Figure 1.
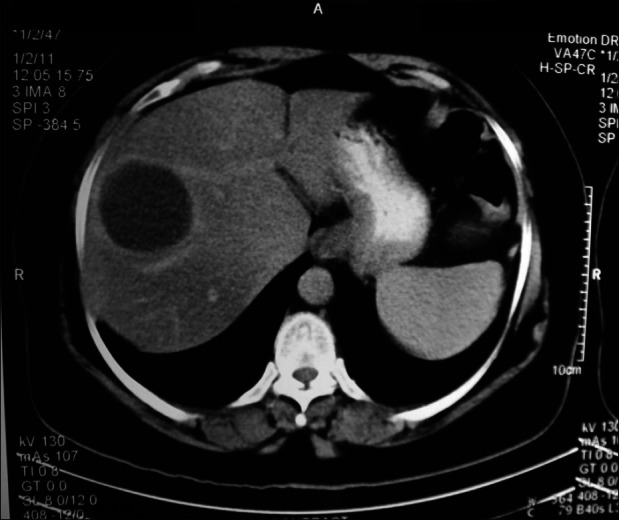
CT scan of the patient
Patient position and team setup
Patient was placed in supine position with legs split. Table was tilted in different directions to gain gravity aided exposure as and when required. Sand bag was placed on left side later in surgery under left lower chest during partial splenectomy. Surgeon was in between legs first and later to the right of patient. Cameraman was on right side of patient. One monitor was placed at head end of patient and another on left side.
Abdominal access technique and port placement
A transverse 3 cm incision was made 6 cm above umbilicus and was deepened up to fascia. Fascia was cleared all around by blunt and sharp dissection. Veress needle was inserted into fascia and pneumoperitoneum of 12 mmHg was created using carbon dioxide gas. Two 10 mm and one 5 mm ports were inserted through the fascia making multiple punctures via same incision and maintaining 1 cm distance between these ports [Figure 2].
Figure 2.
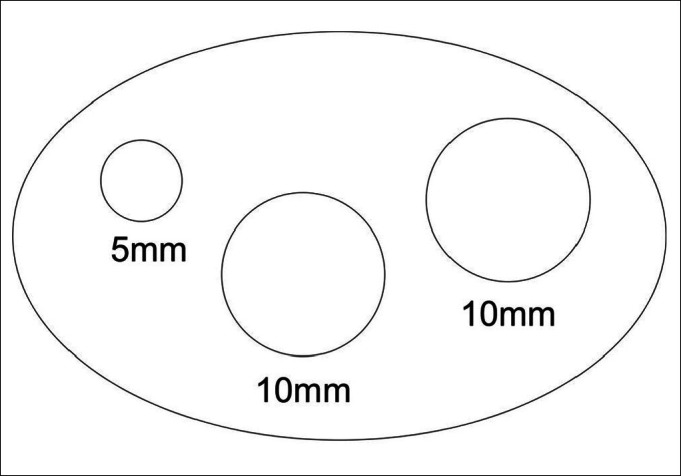
Port placement
Surgical details
Liver hydatid cyst was seen on its superior surface in segment VIII. Gauze pieces soaked in cetrimide 0.5% were placed all around the cyst to contain accidental spillage. Ten millimetre suction with translucent tubing was kept ready near the most prominent point of cyst and a small opening was made. Seropurulent fluid was sucked out immediately as much as possible. Incision was enlarged using ultrasonic shears and 10 mm suction cannula was inserted into the cavity sucking out all hydatid fluid, daughter cysts as well as laminar membrane [Figure 3]. Cavity was irrigated using cetrimide 0.5% thrice, allowed to remain in contact for 10 min and then sucked out. Surrounding areas were also irrigated similarly. Whole of the cavity was de-roofed using ultrasonic shears and inside of cavity was inspected. No residual cysts, laminar membrane or bile leak was found.
Figure 3.
Evacuation of liver cyst
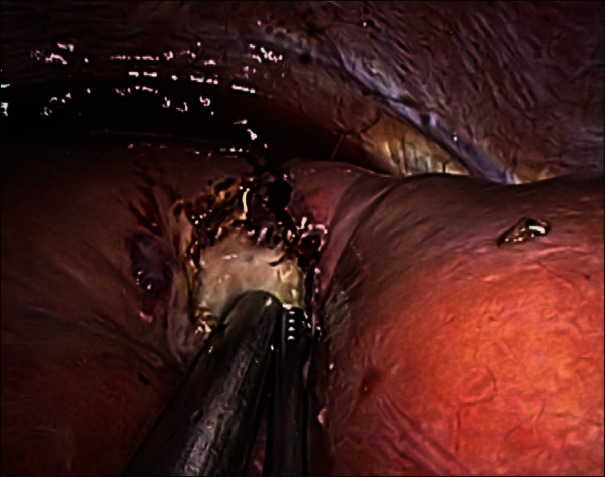
The splenic cyst wall was thick and densely adherent medially to transverse colon. The splenic flexure and part of transverse colon were separated by sharp dissection. Further dissection was not performed to avoid colonic injury. The cyst was opened on its cranial side near normal splenic tissue [Figure 4]. Extraction of the hydatid cyst along with multiple daughter cysts was done. Nearly total cystectomy was performed except that small pericyst was left medially which was adherent to the colonic wall and small part on the hilum of the spleen. The cut end of hydatid cyst was sutured with PDS No. 1 for haemostasis and Argon photo coagulator was used for some part.
Figure 4.
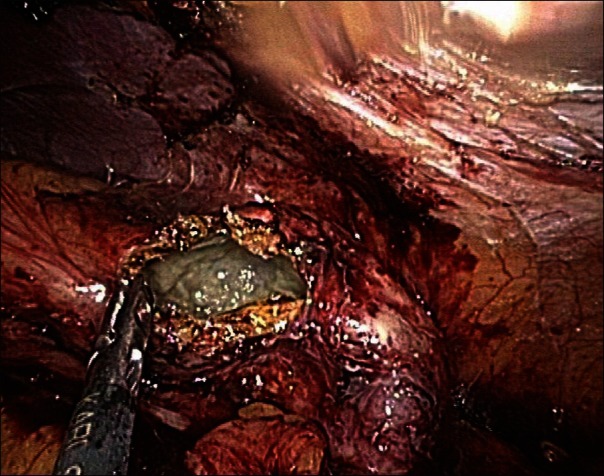
Opened splenic hydatid cyst
Specimen was removed using endobag [Figure 5]. No drain was kept. All the defects in fascia were repaired using polypropylene No. 1 suture. Skin was closed using polyglactin 3-0 subcutaneous suture. Bupivacaine 0.25% was injected locally at the end of surgery.
Figure 5.

Specimen delivered out using endobag
The surgery was successfully performed in 160 min under general endotracheal anaesthesia. No intra-operative or post-operative complications were recorded. Oral liquids were started on day 1 and soft diet on day 2. Patient was discharged on 5th post-operative day. For analgesia, diclofenac suppository was given on day of surgery and twice on first two post-operative days. Thereafter she did not require any analgesia. Patient was put on Albendazole 800 mg twice daily for three months. At the end of 1 month wound scar was hardly noticeable.
DISCUSSION
The face of minimal access surgery has seen many changes in recent years. The port sizes are becoming smaller and their numbers are decreasing. Alternatively, more complex surgeries are now falling within the domain of minimal access surgery. Single incision surgeries are the result of the constant pursuit of surgeons all over the globe to perform scarless surgeries. It may not be scarless but it has the potential to improve cosmesis, decrease post-operative pain and hospital stay and yet be performed with already existing and widely distributed technology. Patients also accept it quickly when told that one incision will be used instead of four or five.
Appendectomies have been done with a single puncture as early as 1992.[6] As the experience with the technique has increased, more complex surgeries are being reported. Single incision laparoscopic splenectomy has been already reported.[7] Where as on one hand single incision laparoscopic approach restricts the movement of instruments in relation to each other, on the other hand, it opens a whole new dimension of range of mobility as far as access to different quadrants of abdomen is concerned. The camera as well as all other instruments inserted through single incision can be rotated together and hence it avoids requirement of additional ports.
For excision of hydatid cyst of liver and partial splenectomy in a single case, altogether different port positions are required. This will increase the number of ports by at least 2 or 3. But in our single incision multi-trocar approach it just required the turn of instruments from liver to spleen and change of patient position. Although umbilicus is the usual site for single incision laparoscopic procedures but here we chose epigastric single incision in order to approach segment 7 and 8 of liver.
Bas et al. have concluded in 2009 that laparoscopic partial splenectomy can be seen as an option to treat splenic hydatid cysts while preserving splenic immunologic functions and causing less pain and better cosmetic results.[6] Hence even though total splenectomy was feasible through this approach, we performed partial splenectomy to preserve splenic tissue.
We used a small single epigastric incision for introduction of multiple trocars. Excluding the use of specialised device for port placement brings down the procedure cost significantly. Inserting ports at slight distance from each other increases the range of movement of instruments and creates a degree of triangulation. The instruments may be changed between ports for different steps.
Many surgeons use curved or articulating instruments for such surgeries but we used routine straight instruments only. Special instruments are costly and require significant learning curve. Routine laparoscopic instruments are much familiar to use, need no extra learning curve and surgeon has excellent control over them. Routine metallic ports used by us are much sturdier and long lasting as compared with most available low profile ports. The length of these ports was not found to interfere during procedure.
CONCLUSION
Single incision multi-trocar surgery has cosmetic advantage over standard laparoscopic approach. It is even more marked when two procedures are combined in different quadrants of abdomen. As this is a rare combination procedure so it remains to be determined if this technique offers additional advantages of decreased analgesia, decreased hospital stay or cost effectiveness.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Khuroo MS. Hydatid disease: Current status and recent advances. Ann Saudi Med. 2002;22:56–64. doi: 10.5144/0256-4947.2002.56. [DOI] [PubMed] [Google Scholar]
- 2.Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev. 2004;17:107–35. doi: 10.1128/CMR.17.1.107-135.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khoury G, Abiad F, Geagea T, Nabout G, Jabbour S. Laparoscopic treatment of hydatid cysts of the liver and spleen. Surg Endosc. 2000;14:243–5. doi: 10.1007/s004640000048. [DOI] [PubMed] [Google Scholar]
- 4.Kathkouda N, Hurwitz M, Gugenheim J, Mavor E, Mason RJ, Waldrep DJ, et al. Laparoscopic management of benign solid and cystic lesions of the liver. Ann Surg. 1999;229:460–6. doi: 10.1097/00000658-199904000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Palanivelu C, Senthilkumar R, Jani K, Rajan PS, Sendhilkumar K, Parthasarthi R, et al. Palanivelu hydatid system for safe and efficacious laparoscopic management of hepatic hydatid disease. Surg Endosc. 2006;20:1909–13. doi: 10.1007/s00464-005-0274-7. [DOI] [PubMed] [Google Scholar]
- 6.Bas G, Alimoglu O, Sahin M, Uranues S. Laparoscopic partial splenic resection in hydatid disease. Eur Surg. 2009;41:90–3. [Google Scholar]
- 7.Barbaros U, Dinccag A. Single-incision laparoscopic splenectomy: The first two cases. J Gastrointest Surg. 2009;13:1520–3. doi: 10.1007/s11605-009-0869-8. [DOI] [PubMed] [Google Scholar]