

Abstract
Objectives. We investigated whether deep tube wells installed to provide arsenic-free groundwater in rural Bangladesh have the added benefit of reducing childhood diarrheal disease incidence.
Methods. We recorded cases of diarrhea in children younger than 5 years in 142 villages of Matlab, Bangladesh, during monthly community health surveys in 2005 and 2006. We surveyed the location and depth of 12 018 tube wells and integrated these data with diarrhea data and other data in a geographic information system. We fit a longitudinal logistic regression model to measure the relationship between childhood diarrhea and deep tube well use. We controlled for maternal education, family wealth, year, and distance to a deep tube well.
Results. Household clusters assumed to be using deep tube wells were 48.7% (95% confidence interval = 27.8%, 63.5%) less likely to have a case of childhood diarrhea than were other household clusters.
Conclusions. Increased access to deep tube wells may provide dual benefits to vulnerable populations in Matlab, Bangladesh, by reducing the risk of childhood diarrheal disease and decreasing exposure to naturally occurring arsenic in groundwater.
Diarrheal disease remains the second largest cause of death for children worldwide, making it a major threat to child health.1 Research from a 6-village study area in Bangladesh suggests that deep tube wells may help reduce this disease burden because they access the deep aquifer, which has lower levels of arsenic and may have lower levels of fecal contamination.2 We have expanded on this work by looking at the effect of deep tube well use across a broader study area and by considering whether distance to a deep tube well plays a role in childhood diarrheal disease risk among deep tube well users.
During the 1970s and 1980s, rural Bangladeshis made a nearly universal shift from drinking surface water to drinking ground water. The efforts of the United Nations International Children’s Emergency Fund, the Bangladesh Department of Public Health and Engineering, and nongovernmental organizations led to the installation of millions of tube wells throughout the country.3 Most of these tube wells tap into the shallow aquifer (< 140 ft) and provide drinking water that is generally considered safe. Tube wells are installed with a hand percussion drilling method that drives polyvinyl chloride pipe to the aquifer; thus installation is inexpensive and feasible for even relatively poor households. The Bangladeshi government and the international community’s campaign in the 1970s and 1980s to promote the use of groundwater for drinking was effective: the majority of rural residents were drinking tube well water by the early 1990s. Coupled with general improvements in hygiene and sanitation, the shift from drinking surface water to drinking groundwater is suggested to have influenced the decline in diarrhea-induced deaths observed in Bangladesh.4
Although the proliferation of tube wells addressed problems associated with drinking contaminated surface water, it exposed individuals to a new health risk. Naturally occurring arsenic levels exceeding the World Health Organization’s and the government of Bangladesh’s drinking water standards (10 μg/L and 50 μg/L, respectively) were identified in the 1990s. An estimated one half of the country’s population was exposed to levels exceeding the World Health Organization standard, and nearly one third was drinking water exceeding the Bangladesh standard.5
By 2000, an article in the Bulletin of the World Health Organization had declared a “public health emergency,” noting studies that an estimated 1 in 10 people with prolonged exposure to drinking water containing 500 micrograms per liter of arsenic will eventually die of cancer.6 Even at lower doses, long-term exposure to arsenic-contaminated drinking water can lead to health problems ranging from skin problems to cancer.7,8 In response to these developments, nearly 5 million wells were tested for arsenic under the Bangladesh Arsenic Mitigation and Water Supply Program. Tube wells exceeding the Bangladesh arsenic standard were painted red, whereas safe wells were painted green. This was intended to provide residents with information about the relative danger or safety of tube well water supplies and to allow informed behavioral change. Bangladeshis’ primary mitigation response was to switch from a shallow high-arsenic well to the nearest shallow low-arsenic well. However, it has been suggested that local hydrogeology and poor sanitation have led to higher levels of fecal contamination in shallow low-arsenic wells,9 leading to concern that residents who switch from shallow high-arsenic wells to shallow low-arsenic wells may face higher diarrheal disease risk.10 In fact, an increase in diarrhea was recently shown among rural households using shallow low-arsenic wells.11
Exposure to either high-arsenic concentrations or high fecal contaminants in shallow wells indicates a need for alternative drinking water sources. After switching to a low-arsenic shallow well, the second most common arsenic mitigation strategy is to obtain drinking water from a deep tube well tapping into an aquifer that is usually more than 500 feet deep. Since 2000, an estimated 165 000 deep tube wells have been installed throughout Bangladesh. Most deep tube wells are public and are installed with aid from the Bangladesh Arsenic Mitigation and Water Supply Program, the Department of Public Health and Engineering, and nongovernmental organizations.12,13 Private ownership of deep tube wells is rare because of high installation costs. Public deep tube wells are, therefore, often located near a rural road or walking path where villagers will have easy access.
Use of a deep tube well may increase walking distance for water collection, given their location in public areas rather than near households. Prior research indicates that villagers may be willing to walk only up to 150 meters to obtain drinking water.14 Additionally, it is possible that longer distances to a deep tube well increase the chances of fecal contamination of stored water supplies, as people who walk farther for water may collect more water at any given time and store it for longer to minimize trips to the well. Any risk of contamination during storage, however, may be balanced by the decreased likelihood of contamination during water extraction from a deep tube well.
Such a protective association between deep tube well use and childhood diarrhea incidence has been identified in a study in 6 villages in rural Bangladesh,2 but the sample was small in that study. We built on those findings by measuring the relationship between deep tube well use and childhood diarrheal disease in an expanded study area. We also investigated the role played by distance to a deep tube well.
METHODS
The study area was the 142 villages of Matlab, a rural region in Bangladesh with a population of 220 000. Households are situated in patrilineal clusters called “baris.” Matlab is the field site for the International Centre for Diarrhoeal Disease Research, Bangladesh, whose hospital is located in Matlab, where residents receive treatment for severe diarrhea and other health conditions free of charge. A health and demographic surveillance system, in place since 1966, maintains records of all births and migration into the study area.
Between 2000 and 2006 the International Centre for Diarrhoeal Disease Research, Bangladesh, conducted a community-level childhood diarrheal disease survey. Community health research workers collected monthly diarrheal disease data by asking mothers whether any child younger than 5 years in the household experienced diarrhea (defined as 3 or more loose or watery stools) during the past 24 hours. The health and demographic surveillance system also conducted a socioeconomic survey in 2005, collecting household-level asset and maternal education information.
In addition, between 2002 and 2004, the International Centre for Diarrhoeal Disease Research, Bangladesh, conducted a comprehensive survey of Matlab’s 12 018 tube wells. Surveyors collected tube well locations using global positioning system receivers and information on tube well depth from well owners, who generally know the length of polyvinyl chloride pipe used to install the well. Then, in 2009, community health research workers supplemented their monthly data collection by asking people to identify any deep community tube well in or adjacent to their bari. Deep tube wells were assigned the same geographic coordinates as the closest bari and were added to the existing tube well database.
We measured whether childhood diarrheal disease incidence in 2005 and 2006 was different for baris using deep versus shallow tube wells. We included 5279 baris in the analysis. Although diarrheal disease data were available starting in 2000, the majority of deep tube wells in the study area were installed in 2005, making it difficult to separate the effect of time (i.e., the generally declining rates of diarrheal disease in Matlab) from the effect of deep tube well use on diarrhea. We did not extend our study beyond 2006 because the total community-level diarrhea survey was replaced by a sample of households in 2007.
Definition of Deep Tube Well Use and Variable Construction
We measured the distance from each bari to the nearest deep tube well in a geographic information system. We assigned baris with a deep tube well a distance of zero. We defined deep and shallow tube well use according to the following assumptions (Figure 1): (1) if a deep tube well was installed in a bari, then we assumed residents of the bari used that deep tube well, regardless of shallow well arsenic concentration; and (2) if individuals resided in a bari without access to a low-arsenic tube well (< 50 μ/L) but had access to a deep tube well within 150 meters from their bari, then we assumed those individuals used a deep tube well. If neither of these assumptions were met, we assumed individuals used a shallow tube well. We derived these assumptions from previous studies suggesting that individuals are willing to walk up to 150 meters for drinking water.2,14 To test the accuracy of these assumptions, we built a logistic regression model using these assumptions to predict deep tube well use in the 6 villages Escamilla et al. surveyed, where they asked people which tube wells they got their drinking water from.2 We correctly classified deep tube well use for 76% of the 179 baris that appear in both study areas.
FIGURE 1—
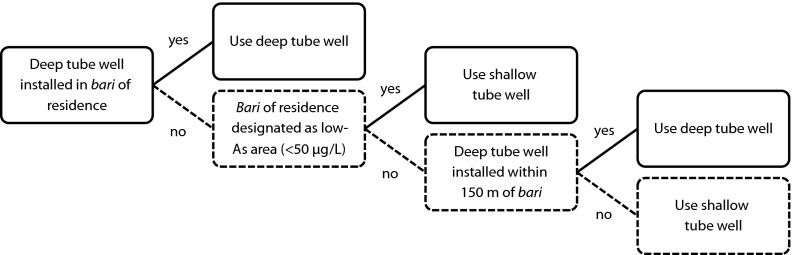
Schematic representation of deep tube well use definition.
To control for the potential confounding role played by socioeconomic status, we created maternal education and wealth indices using data collected in the 2005 health and demographic surveillance system. We constructed the wealth index variable using principal components analysis. The score reflects a composite of 5 variables representing ownership of household assets (bed, bicycle, blanket, lamp, and watch) and 1 variable representing household wall material. We divided the composite index into quintiles.11,15 Maternal education represents the average number of years of education of all mothers in a bari.
Statistical Analysis
We fit a longitudinal logistic regression model to the data using generalized estimating equations under the assumption of an exchangeable correlation matrix. The outcome of interest was occurrence of childhood diarrhea in the year, which was a binary variable.
We used the wealth index, maternal education, population of children younger than 5 years, and year as covariates and a binary variable for deep tube well use as the main predictor of interest. We conducted all statistical analyses with the R statistical software, using the geepack package (R Foundation for Statistical Computing, Vienna, Austria).16,17
RESULTS
We documented 1920 and 1294 cases of childhood diarrhea in 2005 and 2006, respectively, and we estimated between-year correlation of diarrhea occurrence in baris at 0.494 (SE = 0.0542). Overall, we found the distribution of counts of childhood diarrhea to be wider and more variable for shallow tube well users than for deep tube well users (Figure 2). After controlling for maternal education, wealth index, population, and year, we found deep tube well use to be significantly associated with lower childhood diarrheal disease occurrence (Figure 3). Baris that we assumed used deep tube wells were 48.7% (95% confidence interval [CI] = 27.8%, 63.5%) less likely to have a case of childhood diarrhea in the year than were baris that we assumed used shallow tube wells (Figure 3).
FIGURE 2—

Distributions of childhood diarrhea counts for shallow and deep tube well users: Matlab, Bangladesh, 2005–2006.
Note. Width of plots corresponds to probability densities, white dots represent medians, and black rectangles correspond to interquartile ranges of observed distributions. The longer tails associated with the distribution of childhood diarrhea cases among shallow tube well users across both years indicate that disease incidence is both higher and more variable among baris (patrilineal clusters) that primarily used shallow tube wells than is that among those that primarily used deep tube wells.
FIGURE 3—

Full longitudinal logistic regression model odds ratios: Matlab, Bangladesh, 2005–2006.
Note. CI = confidence interval; OR = odds ratio. Baris (patrilineal clusters) assumed to be using shallow tube wells are the reference category.
We assessed the relationship between distance to the nearest deep tube well among deep tube well users and disease occurrence through the incorporation of an interaction term, but we did not find the interaction between distance and use to be significant. In other words, if we assume individuals from a given bari to make use of a deep tube well within 150 meters of the bari, the distance required to travel from the bari to the deep tube well does not significantly affect disease risk. When we interpreted it as a separate term, we found the distance to the nearest tube well to be significantly associated with diarrheal disease; however, this statistically significant association is of little epidemiological relevance, as the effect size was close to zero and significance was probably associated with deep tube well use, which includes distance in its definition.
DISCUSSION
The use of deep tube wells has a protective effect against childhood diarrhea incidence. The risk of diarrhea occurrence among children living in baris that we assumed were using deep tube wells was less than that for those that we assumed were using shallow wells. Although we did not ask bari residents to identify their drinking well, a strong correspondence with known tube well use in the 6-village sample Escamilla et al.2 used supported our tube well assignment when residents explicitly identified their respective drinking wells.
A secondary finding indicates that, at least within 150 meters, distance does not have an effect on childhood diarrheal disease incidence among users of deep tube wells. This suggests that, even if longer walking distances increase water storage time, they do not necessarily increase the risk of enteric disease. It is possible, however, that distance to a deep tube well will affect diarrheal disease at distances greater than 150 meters. This finding reinforces the importance of improved water supply in diarrheal disease risk mitigation and may assist public health practitioners in locating ideal future deep tube well locations by allowing them to site deep public wells within 150 meters of the maximal number of individuals.
This study contributes to the growing body of literature on the role of arsenic mitigation on diarrheal disease risk.10,11,18–20 Findings vary, with recent studies suggesting that switching to shallow low-arsenic wells increases risk10,21 and that water quality at the source is less important than is water storage.18 Although sanitation and hygiene practices such as water storage are important,22 the quality of water at the supply remains integral to the process of ensuring safe drinking water.23 Additionally important to water quality at the source is the extent and ease of access for user populations. Although we investigated the potentially confounding effects of travel distance up to 150 meters, future studies should explore other aspects of access, including ease of use and greater distances, for predicting optimal installation locations.
These findings suggest that deep tube wells are protective for childhood diarrhea; however, further development of the deep tube well infrastructure in rural Bangladesh requires several considerations. The continued involvement of both nongovernmental organizations and the government is needed, as it is not economically feasible for most rural Bangladeshi families to install deep tube wells.24 Community training on deep tube well maintenance is also needed to avoid unsafe practices such as priming with water from a contaminated source.19 The sustainability of deep groundwater quality must also be evaluated.25 Groundwater flow modeling suggests that deep irrigation pumping could induce downward flow from high-arsenic regions, resulting in deep groundwater arsenic contamination. However, these studies also suggest that deep hand-pumped wells could provide arsenic-free water for hundreds of years if use is restricted to domestic rather than agricultural supply.26,27 If deep groundwater quality is sustainable, deep tube well interventions may target low-arsenic regions with poor water quality and high diarrhea incidence.
The main limitation of this study is our assumption regarding deep tube well use. We assumed that people would use a deep tube well if they lived in a bari with a deep tube well or if they lived in a bari without access to a shallow low-arsenic tube well but within 150 meters of a deep tube well. These assumptions correctly classified 76% of the baris from a small subsample of the study area for which interview data are available.
We ran a sensitivity analysis to determine how our definition of deep tube well use might affect inferences if incorrectly specified. Specifically, we randomly selected 25% of the sample baris for which to reclassify deep tube well use. We then reran the analysis using a modified use variable that incorporated the reclassification of 25% of the baris. Results were consistent with those obtained using the original data, except that the protective effect of deep tube well use was lower (odds ratio = 0.789; 95% CI = 0.642, 0.971) although still significantly below 1.0 (data available as a supplement to the online version of this article at http://www.ajph.org). Thus, the inferences we made using our data appear to be robust for detecting a significant protective effect of deep tube well use when the misclassification rate is approximately 25%; however, the magnitude of the effect size will be sensitive to the accuracy of deep tube well use classification.
Our findings indicate a fortunate side effect in policy implementation. Although the goal of the Bangladesh Arsenic Mitigation and Water Supply Program, the Department of Public Health and Engineering, and nongovernmental organizations has been to provide water with lower arsenic levels, deeper tube wells also have served to decrease levels of diarrhea among children in a rural study area. This analysis has important implications for health policy throughout Bangladesh and in parts of South and Southeast Asia, where diarrhea and groundwater arsenic remain great public health concerns. Increasing access to deep tube wells in rural Bangladesh requires careful consideration to ensure sustainability but could have the dual effect of reducing both exposure to arsenic contamination and childhood diarrheal disease.
Acknowledgments
This study was conducted with the support of core donors that provide unrestricted support to International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B) for its operations and research. Current donors providing unrestricted support include the Australian International Development Agency, the government of the People’s Republic of Bangladesh, the Canadian International Development Agency, the Swedish International Development Cooperative Agency, and the Department for International Development, UK. We gratefully acknowledge these donors for their support and commitment to ICDDR,B’s research efforts. The project was also supported by the National Institutes of Health (grants NIH R03-AI076748, NIH 5 T32AI07001-36), the National Institute of Environmental Health Sciences (grant NIEHS T32ES007018), the National Science Foundation (grant NSF BCS-0924479), and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grants 5 R24 HD050924, 5 T32 HD007168).
We thank the anonymous referees for their valuable comments.
Human Participant Protection
The University of North Carolina institutional review board approved this study.
References
- 1.You D, Wardlaw T, Salama P, Jones G. Levels and trends in under-5 mortality, 1990–2008. Lancet. 2010;375(9709):100–103 [DOI] [PubMed] [Google Scholar]
- 2.Escamilla V, Wagner B, Yunus M, Streatfield PK, Van Geen A, Emch M. Effect of deep tubewell use on childhood diarrhoea in Bangladesh. Bull World Health Organ. 2011;89(7):521–527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ebi LK, Mills D, Smith JB. A case study of unintended consequences: arsenic in drinking water in Bangladesh. : Ebi KL, Smith J, Burton I, Integration of Public Health With Adaptation to Climate Change: Lessons Learned and New Directions. London: Taylor & Francis; 2005:72–90 [Google Scholar]
- 4.Caldwell BK, Caldwell JC, Mitra SN, Smith W. Tubewell and arsenic in Bangladesh: challenging a public health success story. Int J Popul Geogr. 2003;9(1):23–38 [Google Scholar]
- 5. Bangladesh Department of Public Health Engineering. Arsenic Contamination of Groundwater in Bangladesh. Keyworth, UK: British Geological Survey. Final technical report WC/00/19.
- 6.Smith AH, Lingas EO, Rahman M. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency. Bull World Health Organ. 2000;78(9):1093–1103 [PMC free article] [PubMed] [Google Scholar]
- 7.Ahsan H, Chen Y, Parvez Fet al. Arsenic exposure from drinking water and risk of premalignant skin lesions in Bangladesh: baseline results from the health effects of arsenic longitudinal study (HEALS). Am J Epidemiol. 2006;163(12):1138–1148 [DOI] [PubMed] [Google Scholar]
- 8.Argos M, Kalra T, Rathouz Pet al. Arsenic exposure from drinking water, and all-cause and chronic-disease mortalities in Bangladesh (HEALS): a prospective cohort study. Lancet. 2010;376(9737):252–258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Leber J, Rahman MM, Ahmed KM, Mailloux B, van Geen A. Contrasting influence of geology on E. coli and arsenic in aquifers of Bangladesh. Ground Water. 2011;49(1):111–123 [DOI] [PubMed] [Google Scholar]
- 10.Van Geen A, Ahmed KM, Akita Yet al. Fecal contamination of shallow tubewell in Bangladesh inversely related to arsenic. Environ Sci Technol. 2011;45(4):1199–1205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wu J, van Geen A, Kazi Matin Aet al. Increase in diarrheal disease associated with arsenic mitigation in Bangladesh. PLoS ONE. 2011;6(12):e29593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ahmed MF, Ahuja S, Alauddin Met al. Ensuring safe drinking water in Bangladesh. Science. 2006;314(5806):1687–1688 [DOI] [PubMed] [Google Scholar]
- 13.Department of Public Health Engineering, Japan International Cooperation Agency. Report on Situation Analysis of Arsenic Mitigation. Dhaka, Bangladesh; 2009.
- 14.Van Geen A, Ahsan H, Horneman AHet al. Promotion of well-switching to mitigate the current arsenic crisis in Bangladesh. Bull World Health Organ. 2002;80(9):732–737 [PMC free article] [PubMed] [Google Scholar]
- 15.Emch M, Yunus M, Escamilla V, Feldacker C, Ali M. Local population and regional environmental drivers of cholera in Bangladesh. Environ Health. 2010;9:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hojsgaard S, Halekoh U, Yan J. The R Package geepack for Generalized Estimating Equations. J Stat Softw. 2005;15(2):1–11 [Google Scholar]
- 17. R Development Core Team. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing; 2010. Available at: http://www.R-project.org. Accessed November 28, 2011.
- 18.Mondal D, Polya D, Giri AKet al. Mitigation of geogenic arsenic bearing groundwaters: assessing the importance of risk substitution arising from waterborne pathogens. Abstract presented at 19th Goldscmidt Conference; June 21–26, 2009. Cambridge, UK: Goldschmidt Conference Abstracts; 2009 [Google Scholar]
- 19.Howard G, Ahmed MF, Shamsuddin AJ, Mahmud SG, Deere D. Risk assessment of arsenic mitigation options in Bangladesh. J Health Popul Nutr. 2006;24(3):346–355 [PMC free article] [PubMed] [Google Scholar]
- 20.Wu J, Yunus M, Streatfield PKet al. Impact of tubewell access and depth on childhood diarrhea in Matlab, Bangladesh. Environ Health. 2011;10:109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Van Geen A, Ahmed K, Akita Yet al. Could arsenic mitigation lead to increased diarrheal disease in Bangladesh? Abstract presented at the American Geophysical Union Fall Meeting; San Francisco, CA; 2010. Abstract No. H11D-0828 [Google Scholar]
- 22.Esrey SA, Potash JB, Roberts L, Shiff C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull World Health Organ. 1991;69(5):609–621 [PMC free article] [PubMed] [Google Scholar]
- 23.Hoque BA, Hallman K, Levy Jet al. Rural drinking water at supply and household levels: quality and management. Int J Hyg Environ Health. 2006;209(5):451–460 [DOI] [PubMed] [Google Scholar]
- 24.Jakariya MM, Von Bromssen M, Jacks G, Chowdhury AMR, Ahmed KM, Bhattacharya P. Searching for a sustainable arsenic mitigation strategy in Bangladesh: experience from two upazilas. Int J Environ Pollut. 2007;31(1–2):415–430 [Google Scholar]
- 25.Van Geen A, Ahmed KM, Seddique AA, Shamsudduha M. Community wells to mitigate the arsenic crisis in Bangladesh. Bull World Health Organ. 2003;81(9):632–638 [PMC free article] [PubMed] [Google Scholar]
- 26.Burgess WG, Hoque MA, Michael HA, Voss CI, Breit GN, Ahmed KM. Vulnerability of deep groundwater in the Bengal aquifer system to contamination by arsenic. Nat Geosci. 2010;3(1):83–87 [Google Scholar]
- 27.Michael HA, Clifford VI. Evaluation of the sustainability of deep groundwater as an arsenic-safe resource in the Bengal basin. Proc Natl Acad Sci USA. 2008;105(25):8531–8536 [DOI] [PMC free article] [PubMed] [Google Scholar]