

Abstract
Objective
Risk factors for falling in elderly people remain uncertain, and the effects of spinal factors and physical ability on body balance and falling have not been examined. The objective of this study was to investigate how factors such as spinal sagittal alignment, spinal range of motion, body balance, muscle strength, and gait speed influence falling in the prospective cohort study.
Methods
The subjects were 100 males who underwent a basic health checkup. Balance, SpinalMouse® data, grip strength, back muscle strength, 10-m gait time, lumbar lateral standing radiographs, body mass index, and fall history over the previous year were examined. Platform measurements of balance included the distance of movement of the center of pressure (COP) per second (LNG/TIME), the envelopment area traced by movement of the COP (E AREA), and the LNG/E AREA ratio. The thoracic/lumbar angle ratio (T/L ratio) and sagittal vertical axis (SVA) were used as an index of sagittal balance.
Results
LNG/TIME and E AREA showed significant positive correlations with age, T/L ratio, SVA, and 10-m gait time; and significant negative correlations with lumbar lordosis angle, sacral inclination angle, grip strength and back muscle strength. Multiple regression analysis showed significant differences for LNG/TIME and E AREA with T/L ratio, SVA, lumbar lordosis angle and sacral inclination angle (R2 = 0.399). Twelve subjects (12 %) had experienced a fall over the past year. Age, T/L ratio, SVA, lumbar lordosis angle, sacral inclination angle, grip strength, back muscle strength, 10-m gait time, height of the intervertebral disc, osteophyte formation in radiographs and LNG/E AREA differed significantly between fallers and non-fallers. The group with SVA > 40 mm (n = 18) had a significant higher number of subjects with a single fall (6 single fallers/18: p = 0.0075) and with multiple falls (4 multiple fallers/18: p = 0.0095).
Conclusion
Good spinal sagittal alignment, muscle strength and 10-m gait speed improve body balance and reduce the risk of fall. Muscle strength and physical ability are also important for spinal sagittal alignment. Body balance training, improvement of physical abilities including muscle training, and maintenance of spinal sagittal alignment can lead to prevention of fall.
Keywords: Fall, Spinal sagittal alignment, Body balance, Muscle strength, Physical ability
Introduction
Falling is an aging-related problem that has increased with aging of society. Elderly people have higher extrinsic and intrinsic risk factors for falling compared to younger people [1, 2], and fall may cause limb and spinal fractures [3, 4]. Thus, falling is a major cause of reduced activity of daily living (ADL) and quality of life (QOL) in the elderly, and may result in increased mortality [5]. Decreased ADL and QOL may also increase the number of bedridden elderly people, with consequent increases in nursing and medical expenses and associated social problems [6–8].
There have been several reports on risk factors for falling in the elderly, but some issues remain unclear [9]. A risk of falling due to body imbalance has been reported based on the results of force platform balance measures [10–12]. Some studies have also suggested a relationship of muscle strength with falling [13], whereas others have not found this relationship [14, 15]; thus, the importance of this factor is yet to be determined. In elderly people, spinal sagittal alignment is likely to be anteversion, and poor spinal sagittal alignment may lead to falling. However, whether sagittal alignment of the whole spine and the range of motion (ROM) of the spine cause poor body balance and falling have not been established. Furthermore, most spine-related studies have focused on females with osteoporosis, while fewer studies have been performed in male subjects. Thus, the objective of this study was to examine body balance, spinal sagittal alignment, spinal ROM, muscle strength, gait speed, and radiographic findings as risk factors related to falling in middle-aged and elderly males in the prospective cohort study.
Subjects and methods
The subjects were healthy volunteers who attended a “basic health checkup” supported by a local government in 2007. This checkup has been held in the town of Yakumo in Hokkaido, Japan, annually for 27 years and is well known among the local people. The checkup program comprises voluntary orthopedic and physical functional examinations for the inhabitants, as well as internal medical examinations and psychological tests. Every year an announcement outlining the aims of the health screening program is mailed to the inhabitants, and their willingness to participate is confirmed by return mail. The inclusion criteria in this study were defined as: (1) age ≥50 years old; (2) male subjects who underwent physical functional examinations and radiographic examinations of the lumbar spine; and (3) subjects who were informed about the study and gave consent to participation in the study.
A total of 315 persons (male, 110; female, 205) underwent a physical functional examination with lumbar radiography in the 2007 health checkup. Females and ten male subjects were excluded from the study: two due to a history of spinal surgery, three with a history of spinal compression fracture, two with otological disease, and three who did not agree to participate in the study. None of the other male subjects had dysfunction of the central or peripheral nervous system (which would prevent platform measurement patterns seen in normal adults) [16] or rheumatoid arthritis, and none were receiving hemodialysis. Therefore, the current study was prospectively performed in 100 male subjects who received examinations using a G-620 stable force platform (Anima, Tokyo, Japan) for balance and SpinalMouse® (Idiag, Volkerswill, Switzerland) for sagittal balance and spinal mobility. The average age of these subjects was 70 years old (range 54–91). Balance, SpinalMouse® data, grip strength, back muscle strength, 10-m gait time, lumbar lateral standing radiographs, body mass index (BMI) and fall history in the previous year were examined as described below. The study was approved by the Committee on Ethics in Human Research of Nagoya University.
Radiographic evaluation
The lumbar lordosis angle (T12–L5) and sacral inclination angle were measured using lumbar lateral standing radiographs in a free-standing posture with fingers on the clavicles and shoulders at 45° of forward elevation [17], and osteophyte formation and disc height were determined as markers of degeneration. Osteophyte formation was evaluated using the Nathan classification (0–4) and the total score (osteophyte score, 0–20) for L1/2–L5/S1 in this classification was also determined [18]. The degree of disc height narrowing was scored based on the scale of Miyakoshi et al. [19], in which 0, 1 and 2 reflect a 0–20, 20–50 and >50 % reduction in disc height, respectively, compared with the L1–L2 disc. The total score from the L2–L3 to L5–S1 discs was defined as the disc score. A disc score of 0 corresponds to no disc degeneration. To assess the effect of potential interobserver error in grading disc narrowing and osteophytes, 20 radiographs with images of 100 discs and intervertebral osteophytes were evaluated independently by five spinal surgeons. The intraclass correlation coefficients in this analysis were 0.96 for disc height narrowing and 0.93 for osteophytes, and both were highly significant.
Regarding sagittal alignment, Jackson defined the thoracic/lumbar angle ratio (T/L ratio) as reflecting the sagittal balance and suggested ranges of 0.15–0.75 for this ratio [20–22]. The value of the T/L ratio was obtained by dividing the thoracic kyphosis angle (neutral position) by the lumbar lordosis angle (neutral position). We also investigated the T/L ratio in Japanese volunteers and found that values of 0.4–1.1 reflected “congruent sagittal alignment” [23, 24]. Elderly persons with a large T/L ratio are likely to lean forward because thoracic kyphosis is not compensated by lumbar lordosis [25].
The sagittal vertebral axis (SVA) has also been proposed as a measure of sagittal alignment [26]. The SVA is defined as the horizontal offset from the posterosuperior corner of S1 to the vertebral body of C7. In asymptomatic adults, Jackson reported a mean SVA offset of 50 ± 25 mm [26]. Recently Schwab et al. [27, 28] proposed a new adult deformity classification and defined SVA > 40 mm as indicating poor sagittal balance and greater SVA indicating poorer sagittal alignment. Therefore, SVA was included in the evaluation and the relationship of subjects with SVA > 40 mm and fallers was examined.
Strictly, examination of the whole spine radiograph with the hip joints is required to evaluate sagittal balance, but this cannot be achieved in a basic health checkup, as described in the “Discussion” section. Therefore, we used the SpinalMouse® for evaluating parameters of spinal alignment in this study.
Evaluation using SpinalMouse®
Spinal range of motion (ROM) and spinal angle were measured using SpinalMouse®, which is an electronic computer-aided device that measures sagittal spinal ROM and intersegmental angles non-invasively using the so-called surface technique. Intraclass coefficients of 0.92–0.95 have been determined for curvature measurement with SpinalMouse® [29]. In the current study, each angle was measured three times in a neutral standing position, maximum bending position, and maximum extension position, and average data were used. The neutral position of SpinalMouse® was the same as that in the radiographic evaluation. The evaluation items included the thoracic kyphosis angle (T1–T12), lumbar lordosis angle (T12–L5), sacral inclination angle, SVA, thoracic ROM, lumbar ROM, and total spinal ROM (Fig. 1). The thoracic kyphosis and lumbar lordosis angles are expressed as positive values in this study. Correlations of the lumbar lordosis angle and sacral inclination angle with lumbar radiograph findings were examined to confirm the reproducibility of SpinalMouse® measurements. Evaluation of SpinalMouse® data revealed significant correlations with lumbar radiographic data for the lumbar lordosis angle (r = 0.794, p < 0.0001) and sacral inclination angle (r = 0.646, p < 0.0001). These significant correlations confirm the reliability of the SpinalMouse® measurements of these angles. Therefore, the SpinalMouse® data were used for sagittal alignment in the analysis performed in this study.
Fig. 1.

SpinalMouse measurements. The thoracic kyphosis angle (T1–T12), lumbar lordosis angle (T12–L5), and sacral inclination angle were measured by SpinalMouse. Spinal ROM was also calculated in the maximum bending position and maximum extension position. T/L ratio and SVA were evaluated as global sagittal balance. TS thoracic kyphosis angle, LS lumbar lordosis angle, S sacrum inclination angle, SVA sagittal vertical axis
Platform measurements of balance
Body balance was assessed using a G-620 stable force platform, which is designed to assess the movement of the center of pressure (COP) as the center of gravity in a horizontal plane, using three vertical load sensors at the corners of an isosceles triangle. The balance test procedure has been described in detail elsewhere [2, 30, 31]. Briefly, the recording was carried out in the corner of a gymnasium. All participants were instructed to stand on the foot plate without their shoes and with their arms at their sides and feet close together. The examination was performed twice, each lasting 30 s with eyes open or closed, and three posturographic variables were assessed: distance of movement of the COP per second (LNG/TIME), envelopment area traced by movement of the COP (E AREA), and the ratio of LNG to E AREA (LNG/E AREA).
Back muscle strength, grip strength, and 10-m gait time
Back muscle strength was determined from the maximal isometric strength of the trunk muscles in a standing posture with 30° lumbar flexion using a digital back muscle strength meter (T.K.K.5402, Takei Co., Japan) [32]. Grip strength was tested with both hands in a standing position and averaged. The average force from two trials was recorded. The maximum strength in each trial was measured and these values showed high reproducibility (r = 0.990, p < 0.0001). The 10-m gait time was evaluated as one of the physical abilities of elderly people [25, 33]. It was measured by a therapist who accompanied each subject to evaluate his maximum speed without running. All subjects were assessed by one examiner who was blinded to the results of other evaluations.
History of fall
A “Fall Record Book” was used to investigate the history of falls. This book was issued by the local government to the town people for use at the checkup. The town people are very familiar with this approach and it has become a custom for them to write down the date, place and causes of a fall and the details of accompanying injuries and bone fracture. The families of elderly people are asked to help with recording of this information. In this study, the presence or absence of a fall in the previous year was determined using the Fall Record Book.
Statistical analysis
All data are shown as mean ± standard deviation (SD). Correlations between variables were analyzed using Pearson correlation coefficient analysis and simple regression analysis. Multiple regression analyses were conducted to determine which variables best correlated with balance. An unpaired t test was used to evaluate differences between groups of subjects with different histories of fall. A Fisher exact test was used for comparison between subjects with SVA > 40 mm and the fall group. Probability values of less than 0.05 were considered to be statistically significant.
Results
The characteristics of the subjects are shown in Table 1. T/L ratio had a significant positive correlation with SVA; and grip strength, back muscle strength and 10-m gait speed showed significant negative correlations with T/L ratio and SVA (Table 2). The results of simple regression analysis of factors related to the movement of the COP are shown in Table 3. Age, T/L ratio, SVA, lumbar lordosis angle, sacral inclination angle, grip strength, back muscle strength, 10-m gait time, and disc score in a lumbar radiograph showed significant relationships with LNG/TIME and E AREA. Multiple regression analysis of LNG/TIME and E AREA (Table 4) for the items that showed significance in the simple regression analysis (using data collected with eyes closed) showed significant correlations with T/L ratio, SVA, lumbar lordosis angle, and sacral inclination angle, but no correlation with age, muscle strength, gait speed, or disc score. Regarding history of fall in the previous year, 12 subjects had fallen once or more (12 %), of whom 6 had fallen twice or more (6 %). There was a significant difference in age, T/L ratio, SVA, sacral inclination angle, grip strength, 10-m gait time disc score and osteophyte formation in radiography, and LNG/E AREA between subjects with one or more falls and those with no previous falls (Table 5). Regarding multiple falls, there was also a significant difference in all these items except for disc score and osteophyte formation, and in back muscle strength and lumbar lordosis angle between subjects who experienced two and more falls and those who had only one or no previous falls (Table 5). The group with SVA > 40 mm (n = 18) had a significantly higher number of subjects with a single fall (6 single fallers/18: p = 0.0075) and with multiple falls (4 multiple fallers/18: p = 0.0095).
Table 1.
Background of the subjects
| Variables | Mean | SD | Range |
|---|---|---|---|
| Age (years) | 70.2 | 7.1 | 54–91 |
| BMI (kg/m2) | 23.8 | 3.0 | 14.4–32.8 |
| T/L ratio | 3.5 | 5.0 | 0.25–29.0 |
| SVA (mm) | 6.7 | 29.0 | −78 to 70 |
| Thoracic kyphosis angle (T1–T12) (°) | 39.0 | 10.9 | 4–68 |
| Lumbar lordosis angle (T12–L5) (°) | 16.5 | 10.0 | −12 to 39 |
| Sacral inclination angle (°) | 5.6 | 7.4 | −13 to 23 |
| Thoracic spinal ROM (°) | 23.6 | 11.8 | 3–51 |
| Lumbar spinal ROM (°) | 48.0 | 13.9 | 18–81 |
| Total spinal ROM (°) | 113.7 | 19.3 | 61–160 |
| Grip strength (kg) | 36.7 | 8.0 | 10.5–54.5 |
| Back muscle strength (kg) | 92.0 | 30.0 | 32–168.5 |
| 10-m gait time (s) | 5.1 | 1.0 | 3.4–8.5 |
| Disc score (total) | 1.1 | 1.5 | 0–6 |
| Osteophyte score (total) | 8.0 | 3.9 | 0–16 |
| Platform measurements of balance | |||
| LNG/TIME (cm/s) | |||
| Eyes open | 1.9 | 0.73 | 0.89–4.6 |
| Eyes closed | 2.7 | 1.2 | 1.0–7.8 |
| E AREA (cm2) | |||
| Eyes open | 3.2 | 1.7 | 1.0–11.1 |
| Eyes closed | 4.4 | 2.6 | 1.3–15.3 |
| LNG/E AREA (1/cm) | |||
| Eyes open | 20.1 | 6.8 | 6.9–38.5 |
| Eyes closed | 20.7 | 7.1 | 9.3–37.2 |
T/L ratio thoracic/lumbar angle ratio, SVA sagittal vertical axis, ROM range of motion, LNG/TIME distance of movement of the center of pressure (COP) per second, E AREA envelopment area traced by movement of the COP, LNG/E AREA ratio of LNG to E AREA
Table 2.
Correlations among sagittal balance, muscle strength and gait speed
| Variables | SVA (mm) | Grip strength (kg) | Back muscle strength (kg) | 10-m gait speed (m/s) |
|---|---|---|---|---|
| T/L ratio | 0.446*** | −0.298* | −0.310* | −0.310* |
| SVA (mm) | −0.321* | −0.369** | −0.334* | |
| Grip strength (kg) | 0.623*** | −0.551*** | ||
| Back muscle strength (kg) | −0.512*** |
Data are Pearson’s correlation coefficients (r)
T/L ratio thoracic/lumbar angle ratio, SVA sagittal vertical axis
* p < 0.005; ** p < 0.0005; *** p < 0.0001
Table 3.
Correlations of LNG/TIME and E AREA with clinical variables
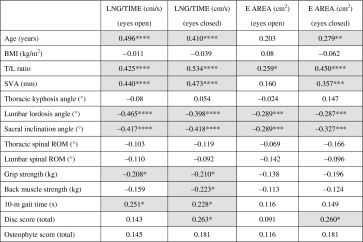
Comparisons in shaded cells were significant
T/L ratio Thoracic/lumbar angle ratio, SVA sagittal vertical axis, ROM range of motion, LNG/TIME distance of movement of the center of pressure (COP) per second, E AREA envelopment area traced by movement of the COP
* p < 0.05; ** p < 0.01; *** p < 0.005, or **** p < 0.0001 (Pearson correlation coefficient (r))
Table 4.
Multiple regression analysis of the association of LNG/TIME (eyes closed) and E AREA (eyes closed) with clinical variables
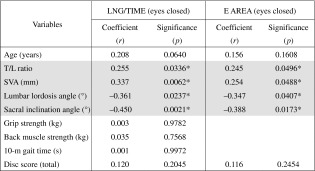
Comparisons in shaded cells were significant
T/L ratio thoracic/lumbar angle ratio, SVA sagittal vertical axis, LNG/TIME distance of movement of the center of pressure (COP) per second, E AREA envelopment area traced by movement of the COP
* Statistically significant
Table 5.
Significant differences between subjects with a history of fall and non-fallers
| Fall (≥ 1 time) | Multiple falls (≥ 2 times) | |||||
|---|---|---|---|---|---|---|
| Faller (≥ 1 time) (n = 12) | Non-Faller (n = 88) | Significance (p) | Multiple falls (n = 6) | One or no falls (n = 94) | Significance (p) | |
| Age (years) | 75.7 ± 8.5 | 69.4 ± 6.6 | 0.0036 | 78.7 ± 6.5 | 69.6 ± 6.8 | 0.0020 |
| T/L ratio | 7.6 ± 8.7 | 3.6 ± 4.7 | 0.0146 | 8.5 ± 6.3 | 3.8 ± 5.3 | 0.0400 |
| SVA (mm) | 27.3 ± 40.9 | 3.8 ± 26.0 | 0.0077 | 39.0 ± 38.8 | 4.6 ± 27.2 | 0.0043 |
| Lumbar lordosis angle (°) | 8.0 ± 10.6 | 17.7 ± 10.3 | 0.0280 | |||
| Sacral inclination angle (°) | 1.3 ± 7.5 | 6.2 ± 7.2 | 0.0298 | −0.5 ± 6.4 | 6.0 ± 7.3 | 0.0343 |
| Grip strength (kg) | 30.9 ± 12.8 | 37.5 ± 6.8 | 0.0064 | 27.9 ± 12.5 | 37.3 ± 7.4 | 0.0047 |
| Back muscle strength (kg) | 63.8 ± 28.9 | 93.6 ± 29.4 | 0.0298 | |||
| 10-m gait time (s) | 5.8 ± 1.4 | 5.0 ± 0.93 | 0.0137 | 6.4 ± 1.6 | 5.0 ± 0.94 | 0.0016 |
| Disc score (total) | 1.9 ± 2.3 | 1.0 ± 1.3 | 0.0437 | |||
| Osteophyte score (total) | 10.1 ± 4.2 | 7.6 ± 3.8 | 0.0399 | |||
| LNG/E AREA (1/cm) (eyes open) | 24.3 ± 8.1 | 19.5 ± 6.4 | 0.0204 | |||
| LNG/E AREA (1/cm) (eyes closed) | 24.6 ± 9.3 | 20.2 ± 6.6 | 0.0416 | 27.5 ± 9.3 | 20.3 ± 6.8 | 0.0159 |
Data are shown as mean ± standard deviation
Other clinical variables had no significant correlations with fall
T/L ratio thoracic/lumbar angle ratio, ROM range of motion, LNG/E AREA the ratio of LNG to E AREA
Discussion
Bone fractures accompanying falling of the elderly further decrease ADL and QOL, and may reduce life expectancy [2, 34]. Among injuries of the elderly, 70 % are related to falling [35] and the severity of the injuries increases with age [36]. Advanced age, number of underlying diseases, motor paralysis, impaired vision, decreased muscle strength, body imbalance, and history of falling have been reported as risk factors for fall [9, 34]. A study of 12 female osteoporosis patients with thoracic kyphosis showed poor balance and an increased propensity to fall on a fall efficacy scale [37]. But, unfortunately, detailed data on spinal sagittal alignment and ROM were not included, and the history of fall was not examined.
The results of our study firstly showed that fallers had poorer body balance, spinal sagittal alignment, muscle strength and gait speed, compared to non-fallers. The relationship between falling and body imbalance in this study supported several previous reports [10–12]. Poor spinal sagittal alignment was related to body imbalance, which may partly account for the association of poor spinal sagittal alignment with falls. This association may also be partly due to an altered vision field. When the body trunk bends forward the direction of the vision line goes downward, which impairs the ability to grasp the circumstances quickly and may cause loss of balance and lead to a fall. While walking, people have to look forward and straiten their spine to have a wider vision to avoid falling. Regarding back muscle strength and physical abilities, the fact that they influenced maintenance of spinal sagittal alignment may account for the relationships of decreased muscle strength and gait speed with the risk of falling. Furthermore, since elderly people tend to shuffle when walking, in part because of a gradual decrease in muscle strength of the whole body, they may be more likely to stumble.
On prevention of falling, previous reports have shown that body balance training improved balance control [7, 38, 39] and that the frequency of fall may be decreased by balance training in elderly females [40–42]. In addition to balance training, our results show that maintenance of spinal alignment to prevent a posture in which the head is bent forward excessively, and improvement of muscle strength and physical abilities are recommended for prevention of falling. Maintaining spinal sagittal alignment may be difficult, but increased back muscle strength may prevent worsening of the situation. Synergistically, a reduced frequency of fall decreases the risk of spinal compression fracture and maintains spinal sagittal alignment. Our previous data showed that both spinal sagittal alignment and muscle strength can influence maintenance of QOL in middle-aged and elderly persons [25, 33]. Thus, the efforts for reduction of the risk of falling can further improve ADL and QOL and will be particularly beneficial for elderly people.
This study has several limitations. Comparison of the results with female patients with osteoporosis would have been useful, but this could not be achieved in the health checkup. Subjects were required to change their clothes to simple ones or undress to permit ideal measurements with SpinalMouse®. However, the health checkup includes internal medicine, urology, ophthalmology and otolaryngology tests, which limits the time and tolerance of subjects for the SpinalMouse® examination. For these reasons, the local government holding the health checkup did not permit a SpinalMouse® examination for females. However, there is a current focus on studies on spinal compression fracture in female patients with osteoporosis, and therefore conducting more studies in males is important. Second, strictly, a whole spine radiograph including the hip joints is required for evaluating sagittal alignment. The pelvic angle or pelvic tilt has recently been suggested to be necessary for evaluating spino-pelvic alignment [20, 22, 26, 43, 44]. Pelvic tilt is an important parameter if there is compensation in the pelvis for a loss of balance. However, in this health checkup, the cost was supported by a small local government and addition of more radiographic examinations and facilities for whole spine radiographs was too expensive. Therefore, evaluation of the relationships between the spine and hip joints was limited by cost. However, the strength of the study is the evaluation of spinal ROM and spinal alignment including sacral slope and SVA simultaneously with other factors in a health checkup. SVA has been shown to have a significant correlation with pelvic tilt [43, 45] and has recently been proposed as the main item for evaluating global sagittal balance in the SRS-Schwab Adult Deformity Classification [28, 46]. It is certain that the patient with over 40 mm of SVA has widely unbalanced posture, and this limit may be more acceptable for the patient with a high pelvic incidence (PI) and a retroverted pelvis than for the patient with a small PI. Unfortunately, SVA could not be evaluated with PI in this study. Furthermore, SVA <40 mm might not be appropriate for definition of the lower limit of sagittal balance for the healthy volunteers who attended this basic health checkup.
In conclusion, spinal alignment, spinal ROM, body balance, muscle strength, 10-m gait time, and lumbar radiograph findings were firstly evaluated in 100 middle-aged and elderly males with no underlying diseases that affected the spine or the movement of the COP in a public health checkup. Body balance, muscle strength, gait speed, and worsened spinal sagittal alignment were significantly associated with fall. Maintenance of spinal sagittal alignment is related to muscle strength, and these factors both stabilize body balance and are mutually related. Therefore, improvement of physical abilities through muscle training and maintenance of spinal sagittal alignment, in addition to body balance training, may be important to prevent falling and maintain ADL of elderly people.
Acknowledgments
The authors thank Ms. Saho Horiuchi for her assistance throughout this study.
Conflict of interest
None.
References
- 1.Piirtola M, Era P. Force platform measurements as predictors of falls among older people—a review. Gerontology. 2006;52:1–16. doi: 10.1159/000089820. [DOI] [PubMed] [Google Scholar]
- 2.Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348:42–49. doi: 10.1056/NEJMcp020719. [DOI] [PubMed] [Google Scholar]
- 3.Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med. 2002;18:141–158. doi: 10.1016/S0749-0690(02)00002-2. [DOI] [PubMed] [Google Scholar]
- 4.Luukinen H, Koski K, Hiltunen L, Kivela SL. Incidence rate of falls in an aged population in northern Finland. J Clin Epidemiol. 1994;47:843–850. doi: 10.1016/0895-4356(94)90187-2. [DOI] [PubMed] [Google Scholar]
- 5.Masud T, Morris RO. Epidemiology of falls. Age Ageing. 2001;30(Suppl 4):3–7. doi: 10.1093/ageing/30.suppl_4.3. [DOI] [PubMed] [Google Scholar]
- 6.Chrischilles E, Shireman T, Wallace R. Costs and health effects of osteoporotic fractures. Bone. 1994;15:377–386. doi: 10.1016/8756-3282(94)90813-3. [DOI] [PubMed] [Google Scholar]
- 7.Melzer I, Elbar O, Tsedek I, Oddsson L. A water-based training program that include perturbation exercises to improve stepping responses in older adults: study protocol for a randomized controlled cross-over trial. BMC Geriatr. 2008;8:19. doi: 10.1186/1471-2318-8-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Province MA, Hadley EC, Hornbrook MC, Lipsitz LA, Miller JP, Mulrow CD, Ory MG, Sattin RW, Tinetti ME, Wolf SL. The effects of exercise on falls in elderly patients. A preplanned meta-analysis of the FICSIT Trials. Frailty and injuries: cooperative studies of intervention techniques. JAMA. 1995;273:1341–1347. doi: 10.1001/jama.1995.03520410035023. [DOI] [PubMed] [Google Scholar]
- 9.Guideline for the prevention of falls in older persons American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention. J Am Geriatr Soc. 2001;49:664–672. doi: 10.1046/j.1532-5415.2001.49115.x. [DOI] [PubMed] [Google Scholar]
- 10.Maki BE, Holliday PJ, Topper AK. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J Gerontol. 1994;49:M72–M84. doi: 10.1093/geronj/49.2.M72. [DOI] [PubMed] [Google Scholar]
- 11.Pajala S, Era P, Koskenvuo M, Kaprio J, Tormakangas T, Rantanen T. Force platform balance measures as predictors of indoor and outdoor falls in community-dwelling women aged 63–76 years. J Gerontol A Biol Sci Med Sci. 2008;63:171–178. doi: 10.1093/gerona/63.2.171. [DOI] [PubMed] [Google Scholar]
- 12.Thapa PB, Gideon P, Brockman KG, Fought RL, Ray WA. Clinical and biomechanical measures of balance as fall predictors in ambulatory nursing home residents. J Gerontol A Biol Sci Med Sci. 1996;51:M239–M246. doi: 10.1093/gerona/51A.5.M239. [DOI] [PubMed] [Google Scholar]
- 13.Buchner DM, Cress ME, de Lateur BJ, Esselman PC, Margherita AJ, Price R, Wagner EH. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol A Biol Sci Med Sci. 1997;52:M218–M224. doi: 10.1093/gerona/52A.4.M218. [DOI] [PubMed] [Google Scholar]
- 14.Daubney ME, Culham EG. Lower-extremity muscle force and balance performance in adults aged 65 years and older. Phys Ther. 1999;79:1177–1185. [PubMed] [Google Scholar]
- 15.Melzer I, Benjuya N, Kaplanski J. Postural stability in the elderly: a comparison between fallers and non-fallers. Age Ageing. 2004;33:602–607. doi: 10.1093/ageing/afh218. [DOI] [PubMed] [Google Scholar]
- 16.Tokita T, Maeda M, Miyata H. The role of the labyrinth in standing posture regulation. Acta Otolaryngol. 1981;91:521–527. doi: 10.3109/00016488109138537. [DOI] [PubMed] [Google Scholar]
- 17.Horton WC, Brown CW, Bridwell KH, Glassman SD, Suk SI, Cha CW. Is there an optimal patient stance for obtaining a lateral 36″ radiograph? A critical comparison of three techniques (Phila Pa 1976) Spine. 2005;30:427–433. doi: 10.1097/01.brs.0000153698.94091.f8. [DOI] [PubMed] [Google Scholar]
- 18.Nathan H, Islael J. Osteophyte of the vertebral column: an anatomical study of their development according to age, race, and sex with considerations as to their etiology and significance. J Bone Joint Surg Am. 1962;44:243–268. [Google Scholar]
- 19.Miyakoshi N, Itoi E, Murai H, Wakabayashi I, Ito H, Minato T. Inverse relation between osteoporosis and spondylosis in postmenopausal women as evaluated by bone mineral density and semiquantitative scoring of spinal degeneration (Phila Pa 1976) Spine. 2003;28:492–495. doi: 10.1097/01.BRS.0000048650.39042.58. [DOI] [PubMed] [Google Scholar]
- 20.Jackson RP, Hales C. Congruent spinopelvic alignment on standing lateral radiographs of adult volunteers (Phila Pa 1976) Spine. 2000;25:2808–2815. doi: 10.1097/00007632-200011010-00014. [DOI] [PubMed] [Google Scholar]
- 21.Jackson RP, Kanemura T, Kawakami N, Hales C. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain (Phila Pa 1976) Spine. 2000;25:575–586. doi: 10.1097/00007632-200003010-00008. [DOI] [PubMed] [Google Scholar]
- 22.Jackson RP, Peterson MD, McManus AC, Hales C. Compensatory spinopelvic balance over the hip axis and better reliability in measuring lordosis to the pelvic radius on standing lateral radiographs of adult volunteers and patients (Phila Pa 1976) Spine. 1998;23:1750–1767. doi: 10.1097/00007632-199808150-00008. [DOI] [PubMed] [Google Scholar]
- 23.Imagama S, Kawakami N, Kanemura T. Evaluation of fixed sagittal imbalance and the effects of intrasacral fixation. J Musculoskel System. 2006;19:633–644. [Google Scholar]
- 24.Kanemura T, Kawakami N, Matsubara Y. Sagittal spinopelvic alignment in adult Japanese volunteers. J Jn Scoliosis Soc. 2001;16:160–164. [Google Scholar]
- 25.Imagama S, Matsuyama Y, Hasegawa Y, Sakai Y, Ito Z, Ishiguro N, Hamajima N. Back muscle strength and spinal mobility are predictors of quality of life in middle-aged and elderly males. Eur Spine J. 2010 doi: 10.1007/s00586-010-1606-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study (Phila Pa 1976) Spine. 1994;19:1611–1618. doi: 10.1097/00007632-199407001-00010. [DOI] [PubMed] [Google Scholar]
- 27.Schwab F, Farcy JP, Bridwell K, Berven S, Glassman S, Harrast J, Horton W. A clinical impact classification of scoliosis in the adult (Phila Pa 1976) Spine. 2006;31:2109–2114. doi: 10.1097/01.brs.0000231725.38943.ab. [DOI] [PubMed] [Google Scholar]
- 28.Schwab F, Lafage V, Farcy JP, Bridwell K, Glassman S, Ondra S, Lowe T, Shainline M. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification (Phila Pa 1976) Spine. 2007;32:2723–2730. doi: 10.1097/BRS.0b013e31815a58f2. [DOI] [PubMed] [Google Scholar]
- 29.Post RB, Leferink VJ. Spinal mobility: sagittal range of motion measured with the SpinalMouse, a new non-invasive device. Arch Orthop Trauma Surg. 2004;124:187–192. doi: 10.1007/s00402-004-0641-1. [DOI] [PubMed] [Google Scholar]
- 30.Masui T, Hasegawa Y, Matsuyama Y, Sakano S, Kawasaki M, Suzuki S. Gender differences in platform measures of balance in rural community-dwelling elders. Arch Gerontol Geriatr. 2005;41:201–209. doi: 10.1016/j.archger.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 31.Masui T, Hasegawa Y, Yamaguchi J, Kanoh T, Ishiguro N, Suzuki S. Increasing postural sway in rural-community-dwelling elderly persons with knee osteoarthritis. J Orthop Sci. 2006;11:353–358. doi: 10.1007/s00776-006-1034-9. [DOI] [PubMed] [Google Scholar]
- 32.Sakai Y, Matsuyama Y, Hasegawa Y, Yoshihara H, Nakamura H, Katayama Y, Imagama S, Ito Z, Ishiguro N, Hamajima N. Association of gene polymorphisms with intervertebral disc degeneration and vertebral osteophyte formation (Phila Pa 1976) Spine. 2007;32:1279–1286. doi: 10.1097/BRS.0b013e318059af8a. [DOI] [PubMed] [Google Scholar]
- 33.Imagama S, Hasegawa Y, Matsuyama Y, Sakai Y, Ito Z, Hamajima N, Ishiguro N. Influence of sagittal balance and physical ability associated with exercise on quality of life in middle-aged and elderly people. Arch Osteoporos. 2011;6:13–20. doi: 10.1007/s11657-011-0052-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319:1701–1707. doi: 10.1056/NEJM198812293192604. [DOI] [PubMed] [Google Scholar]
- 35.Alexander BH, Rivara FP, Wolf ME. The cost and frequency of hospitalization for fall-related injuries in older adults. Am J Public Health. 1992;82:1020–1023. doi: 10.2105/AJPH.82.7.1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma. 2001;50:116–119. doi: 10.1097/00005373-200101000-00021. [DOI] [PubMed] [Google Scholar]
- 37.Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR. Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporos Int. 2005;16:1004–1010. doi: 10.1007/s00198-004-1791-2. [DOI] [PubMed] [Google Scholar]
- 38.Hue OA, Seynnes O, Ledrole D, Colson SS, Bernard PL. Effects of a physical activity program on postural stability in older people. Aging Clin Exp Res. 2004;16:356–362. doi: 10.1007/BF03324564. [DOI] [PubMed] [Google Scholar]
- 39.Melzer I, Benjuya N, Kaplanski J. Effect of physical training on postural control of elderly. Harefuah. 2005;144(839–844):911. [PubMed] [Google Scholar]
- 40.Madureira MM, Takayama L, Gallinaro AL, Caparbo VF, Costa RA, Pereira RM. Balance training program is highly effective in improving functional status and reducing the risk of falls in elderly women with osteoporosis: a randomized controlled trial. Osteoporos Int. 2007;18:419–425. doi: 10.1007/s00198-006-0252-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sihvonen S, Sipila S, Taskinen S, Era P. Fall incidence in frail older women after individualized visual feedback-based balance training. Gerontology. 2004;50:411–416. doi: 10.1159/000080180. [DOI] [PubMed] [Google Scholar]
- 42.Sihvonen SE, Sipila S, Era PA. Changes in postural balance in frail elderly women during a 4-week visual feedback training: a randomized controlled trial. Gerontology. 2004;50:87–95. doi: 10.1159/000075559. [DOI] [PubMed] [Google Scholar]
- 43.Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity (Phila Pa 1976) Spine. 2009;34:E599–E606. doi: 10.1097/BRS.0b013e3181aad219. [DOI] [PubMed] [Google Scholar]
- 44.Schwab F, Lafage V, Boyce R, Skalli W, Farcy JP. Gravity line analysis in adult volunteers: age-related correlation with spinal parameters, pelvic parameters, and foot position (Phila Pa 1976) Spine. 2006;31:E959–E967. doi: 10.1097/01.brs.0000248126.96737.0f. [DOI] [PubMed] [Google Scholar]
- 45.Lafage V, Schwab F, Skalli W, Hawkinson N, Gagey PM, Ondra S, Farcy JP. Standing balance and sagittal plane spinal deformity: analysis of spinopelvic and gravity line parameters (Phila Pa 1976) Spine. 2008;33:1572–1578. doi: 10.1097/BRS.0b013e31817886a2. [DOI] [PubMed] [Google Scholar]
- 46.Schwab F, Ungar B, Blondel B, Buchowski J, Coe J, Deinlein D, DeWald C, Mehdian H, Shaffrey C, Tribus C, Lafage V (2012) Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study (Phila Pa 1976). Spine 37(12):1077–1082 [DOI] [PubMed]