

Abstract
Background
Lateral center-edge angle (LCEA), originally described and validated on AP radiographs, has been used increasingly in CT-based studies, but it is unclear whether the measure is reliable and whether it correlates with that on AP radiographs.
Question/Purposes
We therefore determined: (1) the interobserver and intraobserver reliabilities of the LCEA measured on AP radiographs; (2) the interobserver and intraobserver reliabilities of the LCEA measured on CT scans; and (3) the intermodality correlation of the LCEA between CT and AP radiography.
Methods
We reviewed the AP radiographs and CT scans of 22 patients treated for slipped capital femoral epiphyses. CT scans were reoriented to a neutral pelvic tilt and inclination. Three evaluators measured the LCEA on the unaffected hip on the AP and CT coronal images that corresponded to the center of the acetabulum on the axial slice.
Results
We found an interobserver intraclass correlation (ICC) analysis of 0.84 for the AP radiographs and 0.88 for the CT scans. The intraobserver ICC for the AP radiographs was 0.96, and for the CT scans 0.98. The intermodality ICC for the CT scans and AP radiographs was 0.79, with a lower bound of 0.61 and an upper bound of 0.87.
Conclusions
Our data suggest the LCEA measured on a CT scan is reliable and correlates with the LCEA on AP radiographs.
Introduction
The lateral center-edge angle (LCEA), first described by Wiberg in 1939 [26], continues to be used to quantify superolateral femoral head coverage [6, 9, 15, 16, 20, 25]. Traditionally, the LCEA has been measured on AP radiographs for quantification of acetabular dysplasia with angles less than 20° considered to indicate dysplasia [17, 18, 25]. Furthermore, surgeons have used the LCEA as an assessment parameter of acetabular over-coverage as found in femoroacetabular impingement (FAI) associated pincer morphology, and defined angles greater than 40° to be abnormal [6, 15, 20, 24]. Despite the inherent increased exposure to radiation, CT assessments of abnormal morphologic features in FAI are reportedly useful in preoperative assessments and planning, and for intraoperative decision-making and performing surgery [12]. Consequently, the LCEA measurement (described and validated on AP radiographs) is being measured increasingly on CT scans [2, 8, 10, 12, 13, 21]. However, the use of these measures in CT have not been tested for interobserver or intraobserver reliability or correlated to the LCEA on AP radiographs. In addition, unlike a single biplanar image seen with AP radiographs, a coronal CT involves multiple coronal slices through the acetabulum. Consequently, it has not been well established regarding which coronal slice should be used on CT scans to measure the LCEA and the technique to identify this slice. This makes LCEA findings on CT scans difficult to conduct, interpret, and/or compare with the extensive literature findings of the LCEA on AP radiographs [6, 9, 15–18, 20, 25].
Recent advances in imaging software now enable postprocessing digital reformatting of CT images. This allows for potential opportunistic use of abdominal CTs performed for patients with nonorthopaedic abdominal complaints to be reformatted into standard pelvic CTs, which potentially can provide invaluable data on morphologic features of the hip in a population without orthopaedic complaints [9, 14]. A well-documented technique and an understanding of the correlation and reliability of LCEA measurements on CT scans to AP radiographs would increase the impact of this potential untapped data resource.
We therefore determined: (1) the interobserver and intraobserver reliabilities of the LCEA that is measured on AP radiographs; (2) the interobserver and intraobserver reliabilities of the LCEA that is measured on CT scans; and (3) the intermodality correlation of the LCEA between CT scans and AP radiographs.
Patients and Methods
After institutional review board approval, we reviewed our database of 33 patients with slipped capital femoral epiphysis (SCFE) and identified 22 who had AP radiographs and CT scans of the pelvis. We excluded one patient with bilateral SCFE. There were nine female patients and 13 male patients in the cohort. The average age of the cohort was 13 years (range, 10–16 years).
Standard AP radiographs were taken of patients with suspected SCFE by a board-certified radiographer, with the patient supine and positioned four feet (120 cm) from the X-ray machine (40–125 kVp range, Sociedad Española de Electromedicina y Calidad [SEDECAL] IDEAL, SHF 520, SEDECAL). Using Advantage Workstation 4.3 software (General Electric Co, Fairfield, CT, USA), each pelvic CT scan was temporarily reconstructed, three-dimensionally, to standardize the position of the pelvis with a neutral pelvic tilt and inclination and then reconstructed to 2-mm thickness standard axial and coronal slices [1].
Through a chart review and radiographic assessment (including Kline’s line) we determined which hip was unaffected. This information was provided to three independent reviewers, including one pediatric musculoskeletal radiologist (PK), who measured the LCEAs on the patients’ unaffected hips on AP images and CT scans. On the AP radiographs, the LCEAs were measured with the following method (Fig. 1): (1) To account for pelvic inclination, a line was drawn connecting the right and left ischial tubercles; (2) a perfect-circle clear plastic disc was placed directly on the computer screen (Fig. 2). Using the zoom function, the femoral head was enlarged until the perfect-circle clear plastic disc matched the femoral head contour. The central hole found in the perfect-circle clear plastic disc was used to find the center of the femoral head; then (3) a line from the center of the femoral head that was perpendicular to the line drawn in Step 1 and a line from the center of the femoral head to the most lateral point of the acetabulum were drawn. The angle between these two lines represented the LCEA.
Fig. 1.

The method for measuring the LCEA on an AP radiograph is shown. The dotted circle represents where the perfect-circle clear plastic disc would be placed to find the center of the femoral head. The arrow points to the line representing the pelvic inclination, found by drawing a line that connects the right and left ischial tubercles.
Fig. 2.

An example of the use of the perfect-circle clear plastic disc (commonly found packaged with writable CD or DVD packages as the first and last discs) in finding the center of the femoral head is shown.
Using CT, the LCEA was measured with the following method: (1) The coronal image that correlated with the center of the acetabulum on the axial slice was identified (Fig. 3A); (2) the perfect-circle clear plastic disc was placed on the screen to find the center of the femoral head; then (3) with the pelvic CT scan in a neutral position, a vertical line from the center of the femoral head was drawn. An additional line was drawn from the same starting point to the lateral-most point of the acetabulum. The angle between these two lines represented the LCEA (Fig. 3B).
Fig. 3A–B.
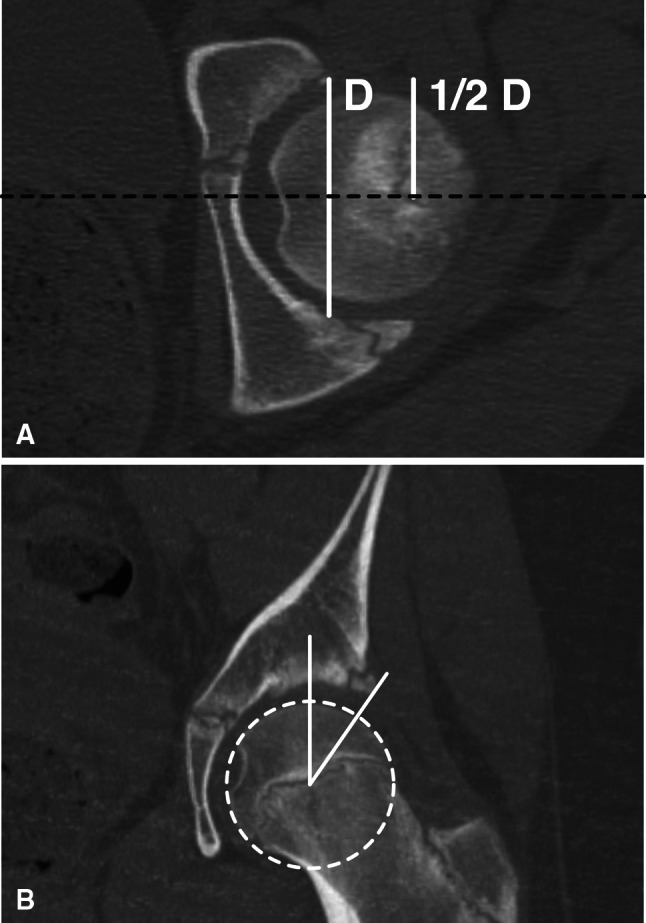
(A) The method for identifying the coronal CT slice to measure the LCEA is shown. The coronal slice, corresponding to the center of the acetabulum on the axial slice, is identified (dotted line) by taking half the distance (1/2D) from the anterior rim of the acetabulum to the posterior rim of the acetabulum (D). (B) The method for measuring the LCEA on the coronal CT slice that was identified in illustration A is shown. The dotted circle represents where the perfect-circle clear plastic disc would be placed to find the center of the femoral head.
Each evaluator first conducted LCEA measurements on either CT scans or AP radiographs for the entire cohort. In 2 weeks LCEA measurements on the opposite modality (CT or AP) were conducted. Evaluators were blinded to the other evaluators’ findings and their own findings for the first modality. One evaluator (SM) repeated the measurements in 2 weeks to assess intraobserver reliability.
Intraobserver and interobserver reliabilities for each measure were assessed using intraclass correlation (ICC) analysis. ICC has a range between 0.0 and 1.0, with values closer to 1.0 representing stronger agreement. We used the two-way mixed model (absolute agreement), as the evaluators in this study were not randomly selected and were measuring identical radiographs. All statistical analyses were conducted using SPSS software (Version 12.0, IBM®, Chicago, IL, USA).
Results
The interobserver ICC for the AP radiographs was 0.84 (95% CI, 0.70–0.92) (p < 0.001). The intraobserver ICC for the AP radiographs was 0.96 (95% CI, 0.91–0.98) (p < 0.001).
The interobserver ICC for the CT scans was 0.88 (95% CI, 0.68–0.95) (p < 0.001), and the intraobserver ICC for the CT scans was 0.98 (95% CI, 0.95–0.99) (p < 0.001).
The overall intermodality ICC for the CT scans and AP radiographs was 0.79 (95% CI, 0.61–0.87) (p < 0.001). The mean difference and standard error were 3.03 and 0.42, respectively. The intermodality ICC for evaluator one was 0.89 (p < 0.001), for evaluator two was 0.75 (p < 0.001) and for evaluator three was 0.74 (p < 0.001).
Discussion
More than 70 years after its creation, the LCEA continues to be an important tool in assessing superolateral femoral head coverage [26]. With the increasing use of advanced imaging, including CT for preoperative planning and diagnosis [12], the adaption and validation of new methods for LCEA measurement are essential to its continued use for diagnostic and treatment-planning purposes. We therefore determined: (1) the interobserver and intraobserver ICCs of the LCEA measured on an AP radiograph; (2) the interobserver and intraobserver ICCs of the LCEA measured on a CT scan; and (3) the intermodality correlation of the LCEA between CT scans and AP radiographs.
Several limitations were apparent in this study. First, the patient cohort was comprised of pediatric patients with SCFE and open physes, which potentially increased the difficulty and variability in measuring the LCEAs. To address this, only patients with unilateral SCFEs were included, and we measured the LCEA only on the unaffected hip. This cohort was specifically chosen since we had a group of patients with SCFE in our practice who had plain radiographs and CT scans. A second limitation stems from the recent widespread adoption of digital radiography, with the unavoidable variation of viewing software. This has inadvertently led to inconsistencies in measurement software tools. Various radiographic measurements, including the LCEA, require a perfect circle function to find the center, or identify the contour of the femoral head, which is not available at our institution [7, 24]. To address this limitation, we used a perfect-circle clear plastic disc to find the center of the femoral head. Although practical and seemingly intuitive, to the best of our knowledge this has not been reported yet. However, the perfect-circle clear plastic disc method was used consistently by all the reviewers on CT scans and AP radiographs, and, therefore, was not a factor in the comparison of measurements made in our study.
We found an interobserver ICC of 0.84 and intraobserver ICC of 0.96 for measuring the LCEA on AP radiographs. In comparison, the interobserver ICCs reported in the literature range from 0.51 to 0.96 and the intraobserver ICCs range from 0.77 to 0.97 (Table 1) [3, 4, 6, 9, 11, 16, 19, 20, 22, 23].
Table 1.
Published interobserver and intraobserver data for the LCEA on AP radiographs
| Study | Intraobserver ICC | Interobserver ICC |
|---|---|---|
| Bouttier et al. [3] | 0.77–0.94 | 0.82 |
| Carroll et al. [4] | 0.78–9.98 | 0.76–0.87 |
| Colvin et al. [6] | 0.92–0.96 | |
| Fowkes et al. [9] | 0.83 | |
| Hansen et al. [11] | 0.90–0.91 | 0.80–0.81 |
| Mast et al. [16] | 0.86–0.97 | 0.73 |
| Nelitz et al. [19] | 0.88–0.92 | 0.85–0.88 |
| Philippon et al. [20] | 0.92 | |
| Tan et al. [22] | 0.85–0.96 | 0.51 |
| Tannast et al. [23] | 0.97–0.98 | 0.92 |
| Current study | 0.96 | 0.84 |
LCEA = lateral center-edge angle; AP = anteroposterior; ICC = intraclass correlation coefficient.
The slightly greater ICC we observed for CT scans versus AP radiographs may be attributable to the less ambiguous lateral point found on a CT slice, and the standardization of the pelvic tilt and inclination of the CT scans. In addition, the interobserver and intraobserver ICCs indicated a reasonable reliability of the method in finding a specific coronal slice for evaluation. Despite the multitude of studies [2, 8, 10, 12, 13, 21] that have measured LCEAs on CT scans, only Heyworth et al. [12] conducted an interobserver reliability analysis, reporting an ICC of 0.78, and only Jacobsen et al. [13] conducted an intraobserver reliability analysis that reported an ICC range of 0.85 to 0.87.
The intermodality ICC of 0.79 indicated what we interpreted as reasonable reliability between measurements of LCEAs on CT scans and AP radiographs. Chen et al. [5] similarly observed that determining the LCEA was reliable when measured on MR images and reported a correlation between LCEAs on AP radiographs and on MR images. The intermodality ICC, coupled with the interobserver and intraobserver reliabilities, showed that an LCEA measured on a CT scan is reliable, feasible, and correlates well with LCEAs on AP radiographs.
As advanced imaging modalities (including CT and MRI) continue to be used for further assessments of coverage or morphology of the hip for improved understanding of femoroacetabular impingement, it will be important to use the data from this study to understand the reliability of indices, such as the LCEA, as we translate them from biplanar radiographs to information obtained from advanced imaging.
Footnotes
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.Abel MF, Sutherland DH, Wenger DR, Mubarak SJ. Evaluation of CT scans and 3-D reformatted images for quantitative assessment of the hip. J Pediatr Orthop. 1994;14:48–53. doi: 10.1097/01241398-199401000-00011. [DOI] [PubMed] [Google Scholar]
- 2.Armiger RS, Armand M, Lepisto J, Minhas D, Tallroth K, Mears SC, Waites MD, Taylor RH. Evaluation of a computerized measurement technique for joint alignment before and during periacetabular osteotomy. Comput Aided Surg. 2007;12:215–224. doi: 10.1080/10929080701541855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bouttier R, Morvan J, Mazieres B, Rat AC, Ziegler LE, Fardellone P, Fautrel B, Guillemin F, Pouchot J, Roux C, Coste J, Saraux A. Reproducibility of radiographic hip measurements in adults. Joint Bone Spine. 2012 March 23. [Epub ahead of print]. [DOI] [PubMed]
- 4.Carroll KL, Murray KA, MacLeod LM, Hennessey TA, Woiczik MR, Roach JW. Measurement of the center edge angle and determination of the Severin classification using digital radiography, computer-assisted measurement tools, and a Severin algorithm: intraobserver and interobserver reliability revisited. J Pediatr Orthop. 2011;31:e30–e35. doi: 10.1097/BPO.0b013e31821adde9. [DOI] [PubMed] [Google Scholar]
- 5.Chen L, Boonthathip M, Cardoso F, Clopton P, Resnick D. Acetabulum protrusio and center edge angle: new MR-imaging measurement criteria. A correlative study with measurement derived from conventional radiography. Skeletal Radiol. 2009;38:123–129. doi: 10.1007/s00256-008-0583-8. [DOI] [PubMed] [Google Scholar]
- 6.Colvin AC, Koehler SM, Bird J. Can the change in center-edge angle during pincer trimming be reliably predicted? Clin Orthop Relat Res. 2011;469:1071–1074. doi: 10.1007/s11999-010-1581-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Delaunay S, Dussault RG, Kaplan PA, Alford BA. Radiographic measurements of dysplastic adult hips. Skeletal Radiol. 1997;26:75–81. doi: 10.1007/s002560050197. [DOI] [PubMed] [Google Scholar]
- 8.Dolan MM, Heyworth BE, Bedi A, Duke G, Kelly BT. CT reveals a high incidence of osseous abnormalities in hips with labral tears. Clin Orthop Relat Res. 2011;469:831–838. doi: 10.1007/s11999-010-1539-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fowkes LA, Petridou E, Zagorski C, Karuppiah A, Toms AP. Defining a reference range of acetabular inclination and center-edge angle of the hip in asymptomatic individuals. Skeletal Radiol. 2011;40:1427–1434. doi: 10.1007/s00256-011-1109-3. [DOI] [PubMed] [Google Scholar]
- 10.Haddad FS, Garbuz DS, Duncan CP, Janzen DL, Munk PL. CT evaluation of periacetabular osteotomies. J Bone Joint Surg Br. 2000;82:526–531. doi: 10.1302/0301-620X.82B4.10174. [DOI] [PubMed] [Google Scholar]
- 11.Hansen BJ, Harris MD, Anderson LA, Peters CL, Weiss JA, Anderson AE. Correlation between radiographic measures of acetabular morphology with 3D femoral head coverage in patients with acetabular retroversion. Acta Orthop. 2012;83:233–239. doi: 10.3109/17453674.2012.684138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Heyworth BE, Dolan MM, Nguyen JT, Chen NC, Kelly BT. Preoperative three-dimensional CT predicts intraoperative findings in hip arthroscopy. Clin Orthop Relat Res. 2012;470:1950–1957. doi: 10.1007/s11999-012-2331-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jacobsen S, Romer L, Soballe K. Degeneration in dysplastic hips: a computer tomography study. Skeletal Radiol. 2005;34:778–784. doi: 10.1007/s00256-005-0019-7. [DOI] [PubMed] [Google Scholar]
- 14.Kang AC, Gooding AJ, Coates MH, Goh TD, Armour P, Rietveld J. Computed tomography assessment of hip joints in asymptomatic individuals in relation to femoroacetabular impingement. Am J Sports Med. 2010;38:1160–1165. doi: 10.1177/0363546509358320. [DOI] [PubMed] [Google Scholar]
- 15.Kutty S, Schneider P, Faris P, Kiefer G, Frizzell B, Park R, Powell JN. Reliability and predictability of the centre-edge angle in the assessment of pincer femoroacetabular impingement. Int Orthop. 2012;36:505–510. doi: 10.1007/s00264-011-1302-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mast NH, Impellizzeri F, Keller S, Leunig M. Reliability and agreement of measures used in radiographic evaluation of the adult hip. Clin Orthop Relat Res. 2011;469:188–199. doi: 10.1007/s11999-010-1447-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Murphy SB, Ganz R, Muller ME. The prognosis in untreated dysplasia of the hip: a study of radiographic factors that predict the outcome. J Bone Joint Surg Am. 1995;77:985–989. doi: 10.2106/00004623-199507000-00002. [DOI] [PubMed] [Google Scholar]
- 18.Murphy SB, Kijewski PK, Millis MB, Harless A. Acetabular dysplasia in the adolescent and young adult. Clin Orthop Related Res. 1990;261:214–223. [PubMed] [Google Scholar]
- 19.Nelitz M, Guenther KP, Gunkel S, Puhl W. Reliability of radiological measurements in the assessment of hip dysplasia in adults. Br J Radiol. 1999;72:331–334. doi: 10.1259/bjr.72.856.10474491. [DOI] [PubMed] [Google Scholar]
- 20.Philippon MJ, Wolff AB, Briggs KK, Zehms CT, Kuppersmith DA. Acetabular rim reduction for the treatment of femoroacetabular impingement correlates with preoperative and postoperative center-edge angle. Arthroscopy. 2010;26:757–761. doi: 10.1016/j.arthro.2009.11.003. [DOI] [PubMed] [Google Scholar]
- 21.Tallroth K, Lepisto J. Computed tomography measurement of acetabular dimensions: normal values for correction of dysplasia. Acta Orthop. 2006;77:598–602. doi: 10.1080/17453670610012665. [DOI] [PubMed] [Google Scholar]
- 22.Tan L, Aktas S, Copuroglu C, Ozcan M, Ture M. Reliability of radiological parameters measured on anteroposterior pelvis radiographs of patients with developmental dysplasia of the hip. Acta Orthop Belg. 2001;67:374–379. [PubMed] [Google Scholar]
- 23.Tannast M, Mistry S, Steppacher SD, Reichenbach S, Langlotz F, Siebenrock KA, Zheng G. Radiographic analysis of femoroacetabular impingement with Hip2Norm-reliable and validated. J Orthop Res. 2008;26:1199–1205. doi: 10.1002/jor.20653. [DOI] [PubMed] [Google Scholar]
- 24.Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis.What the radiologist should know. AJR Am J Roentgenol. 2007;188:1540–1552. doi: 10.2214/AJR.06.0921. [DOI] [PubMed] [Google Scholar]
- 25.Werner CM, Ramseier LE, Ruckstuhl T, Stromberg J, Copeland CE, Turen CH, Rufibach K, Bouaicha S. Normal values of Wiberg’s lateral center-edge angle and Lequesne’s acetabular index: a coxometric update. Skeletal Radiol. 2012;41:1273–1278. doi: 10.1007/s00256-012-1420-7. [DOI] [PubMed] [Google Scholar]
- 26.Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint: With special referance to the complication of osteoarthritis. Acta Chir Scand Suppl. 1939;83(suppl 58):1–135. [Google Scholar]