

Abstract
Background:
Obesity is a common health problem around the world. Studies have shown inverse relationship between serum vitamin D levels with obesity among patients and healthy population. The aim of this present study is to examine the relationship between serum vitamin D levels with general and abdominal obesity among migraine patients.
Methods:
The present study is a cross-sectional and 66 migraine patients aged 19-61 years were included for analysis. Partial correlation was performed to assess association between serum 25-OH-D with general and abdominal obesity. Adjustments were performed for age, sex, and education.
Results:
No relationship was found between serum levels of vitamin D with general and abdominal obesity. However, a significant association was shown between waist circumferences (WC) with body mass index (BMI).
Conclusions:
Serum levels of 25-OH-D were not associated with WC and BMI. Furthermore, after adjustment for confounder variables, no association was observed.
Keywords: Association, migraine, obesity, vitamin D
INTRODUCTION
Obesity has been considered as a general health problem around the world.[1] In the United States, the prevalence of obesity is 35.5% among men and 35.8% among women[2] and in Iran it has been reported 42.9% among men and 56.9% among women.[1]
Obesity is related to increased risk of hyper-tension, diabetes mellitus, cardiovascular disease, arthritis, gallbladder disease, and cancer.[1]
Furthermore, recent studies have shown a possible relationship between migraine and obesity.[3,4] Obesity is associated with greater frequency and severity of migraine.[3] Mechanisms of physiological, psychological and behavioral are involved in the relationship between obesity and migraine.[3]
Vitamin D deficiency has been determined as a public-health issue.[5] The prevalence of vitamin D deficiency is 30-80% among children and adult world-wide.[6] In Iran, prevalence of vitamin D deficiency has been observed 72.1% in men and 75.1% in women.[7] In Isfahan, 19.6%, 23.9% and 26.9 of people have mild, moderate, and severe vitamin D deficiency, respectively.[8]
Vitamin D deficiency is related to musculoskeletal disorders, cancer, autoimmune disorders, cardiovascular disorders, kidney disorders, mental disorders, and skin disorders.[9] Evidence have determined an inverse relationship between vitamin D levels with headache.[5,9–15]
Number of studies have found that serum vitamin D levels are associated with obesity among population health and patients.[16–23] However, in some other studies, the relationship was not seen.[24,25] Thus, the present study was conducted to investigate the association between serum levels of vitamin D with general and abdominal obesity among patients with migraine.
METHODS
Participants
This is a cross-sectional study that was performed among 66 migraine patients aged 19-61 years in Isfahan city, Iran, in autumn 2012. Informed consent was taken from all participants.
Anthropometric measurement and other information's
At baseline, age, gender, weight, height, waist circumference (WC), body mass index (BMI), education level, medical history, the use of vitamin and mineral supplements were gathered. Weight was determined (within 0.5 kg) using analog scale in light clothes and without shoes. Height was determined (within 0.5 cm) with tape measure without shoes. General obesity was assessed using BMI. Overweight and obesity was defined as BMI ≥ 25 and BMI ≥ 30, respectively. BMI was obtained through weight (kilogram) divided into height (meter squared). BMI category was determined as : l0 ean (values < 18.5); normal weight (values 18.5-24.9); overweight (values 25-29.9) and obesity (values ≥ 30). Abdominal obesity was assessed by WC. Central obesity was determined as WC ≥ 88 for women and WC ≥ 102 for men.[1] WC were taken (within 0.5 cm) using inelastic tape at the narrowest part of body, under the ribs.
Biochemical measurement
Serum 25-OH-D3 was measured to evaluate serum vitamin D levels using enzyme-linked immunosorbent assay. Serum vitamin D levels were categorized as : v0 itamin D deficiency (values less than 12 ng/ml); vitamin D insufficiency (values between 12 ng/ml and 30 ng/ml), and vitamin D sufficiency (values more than 30 ng/ml). Calcium, phosphor, and albumin measurements were conducted for the diagnosis of primary hyperparathyroidism.
Statistical analysis
Statistical analysis was performed by the SPSS 18.0 software. Partial correlation was conducted to survey the association between serum levels of vitamin D with general and abdominal obesity. Significance levels were determined as P < 0.05.
RESULTS
In this study, 66 migraine patients with mean age of 35.9 ± 9.01 years were included for analysis. Patients with diabetes mellitus, metabolic syndrome, cardiovascular diseases and hyper-tension, and liver diseases were excluded. There were 49 women with mean age of 35.7 ± years and 17 men with mean age of 36.6 ± 10.2 years. Table 1 shows demographical characteristics of patients. Mean BMI was higher among female. However, mean WC was higher among male. Deficiency, insufficiency, and sufficiency of vitamin D were observed 13.6%, 66.7%, and 19.7% among migraine patients, respectively. 51.5% and 18.2% of adults had overweight and obesity, respectively.
Table 1.
Demographical characteristics of patients
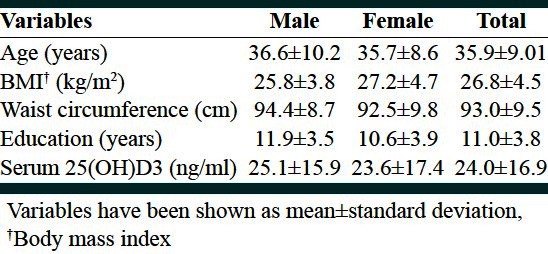
Table 2 shows serum vitamin D status among women and men. 77.6% of women and 88.2% of men have serum vitamin D levels less than 30. There was no differences between serum levels of albumin, calcium, and phosphorus among different vitamin D groups.
Table 2.
Serum vitamin D status according to gender
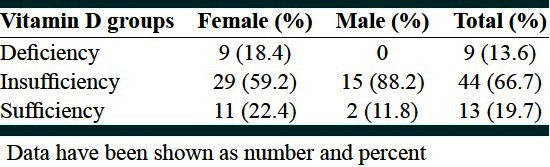
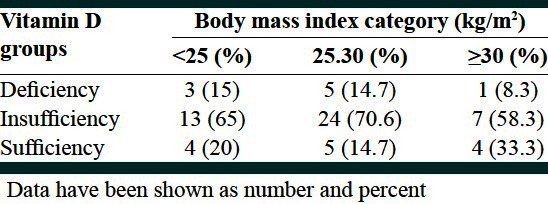
Table 3 describes serum vitamin D status in different groups according to BMI category.
Table 3.
Serum vitamin D status according to body mass index category
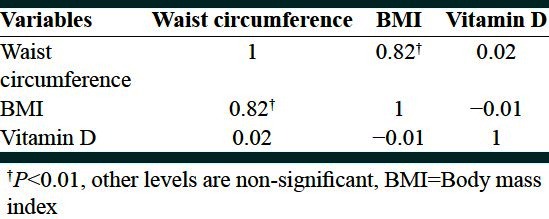
Partial correlation was used to investigate the association between serum levels of vitamin D with BMI and WC.
Table 4 shows the relationship between vitamin D with BMI and WC among patients with migraine. According to Table 4, significant association was not found between serum 25-OH-D levels with WC (P = 0.83) and BMI (P = 0.92). In this analysis, confounding variables such as sex, age, and education were adjusted. However, a significant positive relationship was determined between BMI and WC.
Table 4.
Partial correlation analysis between serum 25-OH-D, waist circumference and body mass index
DISCUSSION
Results of the present study showed that serum levels of vitamin D are not related to WC and BMI. However, a significant inverse relationship was observed between BMI and WC among patients with migraine.
Most studies have shown an inverse relationship between serum levels of vitamin D and general obesity among population health and patients.[16–23] However, in some other studies, the association was not found.[24,25] Furthermore, some studies have shown inverse relationship between serum vitamin D levels with WC,[21,22,25,26] but in some other studies the relationship was not observed.[27]
In a cross-sectional study conducted on obese or overweight patients, vitamin D status was associated with the degree of obesity, especially, in patients with BMI more than 40.Patients with vitamin deficiency had higher BMI and WC and the relationship between vitamin D with metabolic syndrome was not dependent to the degree of obesity.[26] In another study, inverse association was found between serum vitamin D (25-OH-D3 and 1,25-(OH)2-D3) with BMI. Prevalence of vitamin D deficiency was the highest among patients with BMI more than or equal to 40. This results shows one out of every three female and one out of every two male with BMI more than or equal to 40 have vitamin D deficiency.[17] In Kuala Lumpur, a study by Khor et al. was performed among children aged 7-12 years. Only in boys, inverse relationship was observed between BMI for age with vitamin D status.[28]
A study conducted among cancer patients, showed that obese patients have lower vitamin D levels compared with normal weight and overweight individuals. After adjustments for age, a unit increase in BMI was significantly related to reduced 0.42 ng/ml in serum levels of 25-OH-D3.[23] Another study, was carried out in Mashhad in rheumatoid patients. Inverse correlation was determined between BMI with serum vitamin D levels. However, when they were divided into three groups based on vitamin D status, patients with serum levels of vitamin D more than 35 nmol/l had significantly lower BMI compared to serum levels of vitamin D less than 25 nmol/l.[29]
Vilarrasa et al. observed inverse correlation between serum vitamin D levels with weight, BMI, waist to hip ratio, body fat, fat mass and fat free mass. However, after adjustment for confounder variables, only relationship was seen between serum vitamin D with body fat.[30] In another study, higher levels of 25-OH-D3 was inversely associated with BMI, hip circumference and total body fat (TBF) among women not men. However, after adjustments for confounder variables, only inverse relationship was observed between TBF and 25-OH-D3.[27] Moy et al. reported, BMI and WC are related to vitamin D insufficiency (less than 50 nmol/l). Increased WC and BMI is associated within adequate intakes of vitamin D, but with adjustment for confounding variables, WC remained significant.[25]
It looks obese people require higher doses of vitamin D compared with lean people to reach the same levels of vitamin D.[31] In a study, increase in serum vitamin Dafter a year, was significantly and inversely related to BMI at baseline.[31] Similarly, Saliba et al., investigated the association between obesity and increase in serum vitamin D after consumption of vitamin D supplementation. Inverse relationship was observed between serum vitamin D levels and BMI. However, after consumption of vitamin D, increase in the serum vitamin D levels were more obvious at the lower primary levels among individuals with normal weight compared to obese people.[32]
Measurement of 25-OH-D and 1,25-(OH)2-dare valuable among obese people.[16] In Norway, the relationship between serum levels of 25-OH-D and 1,25(OH)2D with body composition was assessed among obese patients. 1,25(OH)2D concentrations was 25.4 pmol/l lower in lowest quartile compared to highest quartile of 25-OH-D. A unit increase in BMI was associated with decreased 1 nmol/l in 25-OH-D and decreased 0.9 pmol/l in 1, 25-(OH)2-D.[16]
In this regard, several hypothesis and mechanisms have been determined for relationship between serum vitamin D levels with obesity. First, obese people are less exposed to sun light.[26] Second, obese patients have inadequate intakes of vitamin D.[26] Third, reduced bioavailability of vitamin D among obese patients.[26] Forth, vitamin D is fat-soluble that is mainly sequestered in adipose tissue,[25,33] thus, is low in serum levels of obese patients.[25]
This study has several limitations. First, the current study is cross-sectional, for this reason we cannot determine a causal link, therefore, clinical trial studies are essential to conduct. Second, the sample size of this study is small and more studies are needed to perform with greater sample size. Third, more adjustments for confounding variables such as physical activity and sun exposure must be performed.
CONCLUSIONS
In summary, no association was observed between serum vitamin D levels with BMI and WC among migraine patients. Therefore, more studies are required to conduct with larger sample size.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Janghorbani M, Amini M, Willett WC, Mehdi Gouya M, Delavari A, Alikhani S, et al. First nationwide survey of prevalence of overweight, underweight, and abdominal obesity in Iranian adults. Obesity (Silver Spring) 2007;15:2797–808. doi: 10.1038/oby.2007.332. [DOI] [PubMed] [Google Scholar]
- 2.Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA. 2012;307:491–7. doi: 10.1001/jama.2012.39. [DOI] [PubMed] [Google Scholar]
- 3.Bond DS, Roth J, Nash JM, Wing RR. Migraine and obesity: Epidemiology, possible mechanisms and the potential role of weight loss treatment. Obes Rev. 2011;12:e362–71. doi: 10.1111/j.1467-789X.2010.00791.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bigal ME, Lipton RB, Holland PR, Goadsby PJ. Obesity, migraine, and chronic migraine: Possible mechanisms of interaction. Neurology. 2007;68:1851–61. doi: 10.1212/01.wnl.0000262045.11646.b1. [DOI] [PubMed] [Google Scholar]
- 5.Prakash S, Mehta NC, Dabhi AS, Lakhani O, Khilari M, Shah ND. The prevalence of headache may be related with the latitude: A possible role of Vitamin D insufficiency? J Headache Pain. 2010;11:301–7. doi: 10.1007/s10194-010-0223-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Andıran N, Çelik N, Akça H, Doğan G. Vitamin D deficiency in children and adolescents. J Clin Res Pediatr Endocrinol. 2012;4:25–9. doi: 10.4274/jcrpe.574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Moradzadeh K, Larijani B, Keshtkar AA, Hossein-Nezhad A, Rajabian R, Nabipour I, et al. Normative values of Vitamin D among Iranian population: A population based study. Int J Osteoporosis Metab Disorders. 2008;1:8–15. [Google Scholar]
- 8.Hovsepian S, Amini M, Aminorroaya A, Amini P, Iraj B. Prevalence of vitamin D deficiency among adult population of Isfahan City, Iran. J Health Popul Nutr. 2011;29:149–55. doi: 10.3329/jhpn.v29i2.7857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Prakash S, Shah ND. Chronic tension-type headache with vitamin D deficiency: Casual or causal association? Headache. 2009;49:1214–22. doi: 10.1111/j.1526-4610.2009.01483.x. [DOI] [PubMed] [Google Scholar]
- 10.Turner MK, Hooten WM, Schmidt JE, Kerkvliet JL, Townsend CO, Bruce BK. Prevalence and clinical correlates of vitamin D inadequacy among patients with chronic pain. Pain Med. 2008;9:979–84. doi: 10.1111/j.1526-4637.2008.00415.x. [DOI] [PubMed] [Google Scholar]
- 11.Kjaergaard M, Eggen AE, Mathiesen EB, Jorde R. Association between headache and serum 25-Hydroxyvitamin D; the Tromsø study: Tromsø 6. Headache. 2012;52:1499–505. doi: 10.1111/j.1526-4610.2012.02250.x. [DOI] [PubMed] [Google Scholar]
- 12.Thys-Jacobs S. Vitamin D and calcium in menstrual migraine. Headache. 1994;34:544–6. doi: 10.1111/j.1526-4610.1994.hed3409544.x. [DOI] [PubMed] [Google Scholar]
- 13.Thys-Jacobs S. Alleviation of migraines with therapeutic vitamin D and calcium. Headache. 1994;34:590–2. doi: 10.1111/j.1526-4610.1994.hed3410590.x. [DOI] [PubMed] [Google Scholar]
- 14.Knutsen KV, Brekke M, Gjelstad S, Lagerløv P. Vitamin D status in patients with musculoskeletal pain, fatigue and headache: A cross-sectional descriptive study in a multi-ethnic general practice in Norway. Scand J Prim Health Care. 2010;28:166–71. doi: 10.3109/02813432.2010.505407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wheeler SD. Vitamin D deficiency in chronic migraine. Headache. 2008;48:S52–3. [Google Scholar]
- 16.Lagunova Z, Porojnicu AC, Vieth R, Lindberg FA, Hexeberg S, Moan J. Serum 25-hydroxyvitamin D is a predictor of serum 1,25-dihydroxyvitamin D in overweight and obese patients. J Nutr. 2011;141:112–7. doi: 10.3945/jn.109.119495. [DOI] [PubMed] [Google Scholar]
- 17.Lagunova Z, Porojnicu AC, Lindberg F, Hexeberg S, Moan J. The dependency of vitamin D status on body mass index, gender, age and season. Anticancer Res. 2009;29:3713–20. [PubMed] [Google Scholar]
- 18.Parikh SJ, Edelman M, Uwaifo GI, Freedman RJ, Semega-Janneh M, Reynolds J, et al. The relationship between obesity and serum 1,25-dihydroxy vitamin D concentrations in healthy adults. J Clin Endocrinol Metab. 2004;89:1196–9. doi: 10.1210/jc.2003-031398. [DOI] [PubMed] [Google Scholar]
- 19.Konradsen S, Ag H, Lindberg F, Hexeberg S, Jorde R. Serum 1,25-dihydroxy vitamin D is inversely associated with body mass index. Eur J Nutr. 2008;47:87–91. doi: 10.1007/s00394-008-0700-4. [DOI] [PubMed] [Google Scholar]
- 20.Garanty-Bogacka B, Syrenicz M, Goral J, Krupa B, Syrenicz J, Walczak M, et al. Serum 25-hydroxyvitamin D (25-OH-D) in obese adolescents. Endokrynol Pol. 2011;62:506–11. [PubMed] [Google Scholar]
- 21.Tamer G, Mesci B, Tamer I, Kilic D, Arik S. Is vitamin D deficiency an independent risk factor for obesity and abdominal obesity in women? Endokrynol Pol. 2012;63:196–201. [PubMed] [Google Scholar]
- 22.Lee SH, Kim SM, Park HS, Choi KM, Cho GJ, Ko BJ, et al. Serum 25-hydroxyvitamin D levels, obesity and the metabolic syndrome among Korean children. Nutr Metab Cardiovasc Dis. 2012;22:1–7. doi: 10.1016/j.numecd.2012.04.013. [DOI] [PubMed] [Google Scholar]
- 23.Vashi PG, Lammersfeld CA, Braun DP, Gupta D. Serum 25-hydroxyvitamin D is inversely associated with body mass index in cancer. Nutr J. 2011;10:51. doi: 10.1186/1475-2891-10-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Baradaran A, Behradmanesh S, Nasri H. Association of body mass index and serum vitamin D level in healthy Iranian adolescents. Endokrynol Pol. 2012;63:29–33. [PubMed] [Google Scholar]
- 25.Moy FM, Bulgiba A. High prevalence of vitamin D insufficiency and its association with obesity and metabolic syndrome among Malay adults in Kuala Lumpur, Malaysia. BMC Public Health. 2011;11:735. doi: 10.1186/1471-2458-11-735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Miñambres I, Sánchez-Hernández J, Sánchez-Quesada JL, Rodríguez J, de Leiva A, Pérez A. The association of hypovitaminosis d with the metabolic syndrome is independent of the degree of obesity. ISRN Endocrinol. 2012;2012:691803. doi: 10.5402/2012/691803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jungert A, Roth HJ, Neuhäuser-Berthold M. Serum 25-hydroxy vitamin D3 and body composition in an elderlycohort from Germany: Across-sectional study. Nutr Metab (Lond) 2012;9:42. doi: 10.1186/1743-7075-9-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Khor GL, Chee WS, Shariff ZM, Poh BK, Arumugam M, Rahman JA, et al. High prevalence of vitamin D insufficiency and its association with BMI-for-age among primary school children in Kuala Lumpur, Malaysia. BMC Public Health. 2011;11:95. doi: 10.1186/1471-2458-11-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Goshayeshi L, Saber H, Sahebari M, Rezaieyazdi Z, Rafatpanah H, Esmaily H, et al. Association between metabolic syndrome, BMI, and serum vitamin D concentrations in rheumatoid arthritis. Clin Rheumatol. 2012;31:1197–203. doi: 10.1007/s10067-012-1995-3. [DOI] [PubMed] [Google Scholar]
- 30.Vilarrasa N, Maravall J, Estepa A, Sánchez R, Masdevall C, Navarro MA, et al. Low 25-hydroxyvitamin D concentrations in obese women: Their clinical significance and relationship with anthropometric and body composition variables. J Endocrinol Invest. 2007;30:653–8. doi: 10.1007/BF03347445. [DOI] [PubMed] [Google Scholar]
- 31.Jorde R, Sneve M, Emaus N, Figenschau Y, Grimnes G. Cross-sectional and longitudinal relation between serum 25-hydroxyvitamin D and body mass index: The Tromsø study. Eur J Nutr. 2010;49:401–7. doi: 10.1007/s00394-010-0098-7. [DOI] [PubMed] [Google Scholar]
- 32.Saliba W, Barnett-Griness O, Rennert G. The relationship between obesity and the increase in serum 25(OH) D levels in response to vitamin D supplementation. Osteoporos Int. 2012;25:1147–54. doi: 10.1007/s00198-012-2129-0. [DOI] [PubMed] [Google Scholar]
- 33.Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72:690–3. doi: 10.1093/ajcn/72.3.690. [DOI] [PubMed] [Google Scholar]