

Abstract
Outpatient burden of laboratory-confirmed influenza among children in Knox and Davidson Counties was compared in 2006–2007 when only Knox County had a school-based influenza vaccine campaign. Of 1016 eligible children seeking outpatient care, 87% were enrolled and 20% were influenza-positive. Estimated influenza vaccination coverage was similar in Knox and Davidson for preschool-age children (36% versus 33%) but higher for school-age children (44% versus 12%). Influenza detection was higher among Knox than Davidson County preschool-age children (18% versus 10%) but similar among school-age children (28% versus 27%). These data are consistent with a direct effect of the campaign in school-age children.
Keywords: influenza vaccine, epidemiology, school-based vaccination
1. Introduction
Acute respiratory illnesses (ARIs) are responsible for over 20% of all ambulatory care visits among U.S. children <13 years of age,[1] with influenza accounting for 5%–30% of all outpatient visits during the influenza season annually among children aged <5 years.[2–6] Due to the large burden of influenza, the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC) recommended universal influenza vaccination of all children aged 6–23 months and their household contacts in 2004–2005.[7–10] Beginning in the 2006–2007 season, universal influenza vaccination was extended to all children aged 6–59 months and their household contacts.[11] In 2008, both the ACIP and the American Academy of Pediatrics expanded universal influenza vaccination to all children aged 0.5–18 years.[12;13]
Prior to the 2005–2006 influenza season, a school-based, live-attenuated influenza vaccination program was conducted in Knox County, achieving coverage of 45% of school-age children enrolled in county public schools.[14] Since a similar immunization campaign was launched in Knox County the next season (2006–2007), targeted at 70% coverage, we sought to measure the impact of this program. As part of the CDC-funded New Vaccine Surveillance Network activities we conducted active population-based surveillance for laboratory-confirmed influenza in children aged <13 years in Davidson County, TN, located about 180 miles west of Knox County. Similar outpatient surveillance was established in Knox County with the goal of comparing the proportion of children aged <13 years in outpatient (emergency department (ED) and hospital-based clinic) settings with laboratory-confirmed influenza infections between the two counties.
2. Methods
2.1. School-based vaccination campaign in Knox County
The Knox County Department of Health initiated an extensive, school-based live-attenuated influenza vaccination campaign (LAIV, Medimmune) in both public and private schools between September and December 2006. Across Knox County, 48% of all public and private school children were vaccinated;[15] half of children <9 years received the recommended 2-dose LAIV series (John Lott, personal communication). The campaign was completed well before the influenza season.
2.2. County Descriptions
Knox County, TN has approximately 412,000 residents of whom 6% are <5 years and 16% are 5–17 years of age, 88% are white, 9% are black and 2% are Hispanic. The 2006 median family income was $59,467 and 10% of families were below the poverty level.[16] In comparison, Davidson County, TN has approximately 579,000 residents of whom 8% are <5 years and 16% are 5–17 years of age, 65% are white, 28% are black and 7% are Hispanic. The 2006 median family income was $54,309 and 12% of families were below the poverty level.[16]
2.3. Study Population
All children aged <13 years from Knox or Davidson County who presented to the ED or outpatient clinic at the children’s hospital in each county with a parental report of respiratory symptoms or fever were eligible for enrollment. Although only children ≥6 months are recommended to receive influenza vaccine, we included those too young to be vaccinated, to assess potential indirect benefits. Respiratory symptoms included cough, nasal congestion, wheezing, sore throat, earache, difficulty breathing or fever. Study nurses enrolled approximately 6–8 eligible children per surveillance day in each setting. In each clinic, children were enrolled on average 2 days per week during clinic hours. In the ED, children were enrolled an average of 2 and 4 days per week in Knox and Davidson Counties, respectively, with systematic variation representing all weekdays but time periods from 10am–8pm. If multiple children were available concurrently, nurses approached the first triaged child. Children were not eligible if they had been enrolled in the past 4 days, if the parent/guardian did not speak English, if the parent/guardian was not present or did not give written informed consent, or if age and developmentally appropriate children did not assent. Children whose parents did not speak English accounted for 1% and 5% of the eligible population in Knox and Davidson County, respectively. Approximately 85% and 50% of all county children seeking care for ARIs or fever in any ED presented to the surveillance ED in Knox and Davidson Counties, respectively.
2.4. Ethics
The study was approved by the Institutional Review Boards of East Tennessee Children’s Hospital and Vanderbilt University School of Medicine.
2.5. Settings and Comparison of Vaccination Coverage
Children seen in the ED or outpatient clinic of the children’s hospital in each county were targeted for enrollment. All of these settings serve an urban, underserved population with >80% of children having public insurance. Because analyses by the clinic and ED setting were similar, they are combined. Since the EDs served at least half of each county population, we used vaccination coverage of influenza-negative ED children to estimate the influenza vaccine coverage among county children who seek care in the ED for ARI or fever. In fact, our estimated coverage in Knox County school-age children was close to the county’s estimated percentage of school-age children vaccinated. We had no universal vaccine registry or independent estimate of vaccination rates in Davidson County.
2.6. Data collection
Each enrolled child had a standardized survey administered to the parent/guardian to ascertain demographic characteristics, illness history, medical history, and influenza vaccination status in 2006–2007. Nasal and throat swabs for influenza detection were obtained from all enrolled children. Chart review ascertained insurance status and medical history.
2.7. Influenza Vaccination Status
Parental report of the child’s influenza vaccination status was verified with the Tennessee Immunization Registry (not universal) or the clinic where the child received vaccinations. Children with verified influenza vaccination status were classified as fully vaccinated, partially vaccinated or unvaccinated. Only vaccinations given ≥14 days prior to enrollment were enumerated, which did not impact the vaccination status of any child who received LAIV. For the 2006–2007 season, children were considered fully vaccinated if they were aged ≥9 years and received one dose of the 2006–2007 influenza vaccine; if they were aged 0.5–8 years and received two doses of influenza vaccine at least one month apart; or if they were aged 1–8 years, received one dose of influenza vaccine and had been previously vaccinated. Children were considered partially vaccinated if they were aged 0.5–8 years, received one of two recommended doses of influenza vaccine and were not previously vaccinated. Children were considered unvaccinated if they did not receive any influenza vaccine ≥14 days prior to enrollment. Most (78%, 221/282) first doses of influenza vaccine and 37% (19/51) of second doses were administered prior to the influenza season.
2.8. Definition of Influenza Season
Although surveillance was conducted from November through April, influenza season was defined as the 18-week period from December 10, 2006 through April 14, 2007, which captured all positive influenza results in both counties.
2.9. Laboratory Procedures
Nasal and throat swabs were obtained from all enrolled children and transported in viral transport media on ice and stored at 2–8°C until processing (within 24 hours). Aliquots were diluted with lysis buffer (Roche Applied Science) and stored at −80°C. RNA was extracted from frozen aliquots using automated methods (MagNApure LC, Roche Applied Science). Real-time reverse transcriptase polymerase chain reaction (RT-PCR) assays were performed using influenza A and B primers and probes previously described.[17;18] Each specimen was also tested for β-actin (Applied Biosystems).[19;20] Specimens without detectable β-actin on three separate analyses were considered inadequate and excluded from analysis. Influenza infection was defined as a specimen with detectable β-actin and two positive consecutive PCR assays for influenza A or B (to exclude potential false-positives that can occur with highly sensitive PCR-based assays).[21] A portion of PCR-positive specimens were cultured in primary rhesus monkey kidney cells and sent to the CDC for influenza subtyping.
2.10. Analysis
The primary study outcome compared the proportion of influenza-positive children by county and age groups by binomial distribution for both settings combined and assumed that other causes of ARI would be similar between the two counties. The p-value was computed to test the null hypothesis that p1=p2 in the two counties. The study was powered to detect relatively large differences in the proportion of children with influenza in the two counties based on the assumptions 1) that 70% of Knox County school children were targeted to be vaccinated, 2) that few (<10%) Davidson County school children would be vaccinated in the absence of a national recommendation for school-age children or a school-based campaign, and 3) that mathematical models predicted if 20% of children were vaccinated then the number of influenza cases would decrease by 46%.[22] Given 330 enrolled children <13 years of age in each county and a projected proportion of influenza-positive children in Davidson County of 20%, 10%, or 5%, we had at least 80% power to detect significant differences if the proportion of Knox County visits with influenza infection was 12%, 4%, and 1% or lower, respectively. Assessment of overall vaccination coverage included only those children who were aged 0.5–12 years with verified influenza vaccination status, enrolled in the ED and were influenza-negative. Although influenza-negative children with ARI in the ED may not precisely reflect the overall county vaccination rates, they were used to compare vaccination differences between the two studied counties.
Influenza isolates were sent to the CDC and classified as good match, minor antigenic variant, or poor match to the 2006–2007 vaccine; the results for each county were compared by chi-square test.
3. Results
3.1. Enrollment Characteristics
Knox County: Of 532 eligible children approached during the 18-week influenza season of 2006–2007, 443 (83%) were enrolled. Reasons for non-enrollment were parent or child refusal to participate (88%) or parent was not available (12%). Six children’s samples had no detectable β-actin and were excluded, leaving a study population of 437 children from Knox County.
Davidson County: Of 484 eligible children approached during the influenza season, 447 (92%) were enrolled. Reasons for non-enrollment were parent or child refusal to participate (30%), parent was not available (3%), parent did not speak English (62%) and unknown (5%). Three children had no detectable β-actin and were excluded, leaving a study population of 444 children from Davidson County.
3.2. Demographic Characteristics and Symptoms
More Knox County children were enrolled in the ED (359, 82%) than in the hospital-based clinic (78, 18%); whereas more Davidson County children were enrolled in the hospital-based clinic (255, 57%) than in the ED (189, 43%). Most parents (91%) reported that their child had a regular doctor and 31% reported that their child had previously seen a doctor for this illness prior to the enrollment visit. Enrolled and non-enrolled children differed only in that non-enrolled children were younger and more likely to have unknown insurance status.
Combining both study sites, the demographic characteristics were similar for influenza-positive and influenza-negative children with two exceptions. More black than white children had confirmed influenza (Table 1); more school-age than preschool-age children were influenza-positive (27% versus 14%, p<0.001, Figure 1).
Table 1.
Demographic characteristics and influenza vaccination status of all Knox and Davidson County children.
| Knox County, N (%) N=437 |
Davidson County, N (%) N=444 |
Combined, N (%) N=881 |
|||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Demographics | Influenza + N= 95 |
Influenza − N=342 |
p-value | Influenza + N= 79 |
Influenza − N=365 |
p-value | Influenza + N= 174 |
Influenza − N=707 |
p-value |
|
| |||||||||
| Age group | |||||||||
| 0–<0.5 years | 2 (2%) | 28 (8%) | 0.03 | 1 (1%) | 65 (18%) | <0.001 | 3 (2%) | 93 (14%) | <0.001 |
| 0.5–<5 years | 47 (49%) | 194 (57%) | 23 (29%) | 150 (44%) | 70 (40%) | 344 (49%) | |||
| 5–8 years | 34 (36%) | 82 (24%) | 41 (52%) | 98 (27%) | 75 (43%) | 180 (25%) | |||
| 9–12 years | 12 (13%) | 38 (11%) | 14 (18%) | 52 (14%) | 26 (15%) | 90 (13%) | |||
|
| |||||||||
| Gender | |||||||||
| Male | 55 (58%) | 165 (48%) | 0.10 | 46 (58%) | 200 (55%) | 0.58 | 101 (58%) | 365 (52%) | 0.13 |
|
| |||||||||
| Race | |||||||||
| Black | 32 (34%) | 64 (19%) | 0.001 | 48 (61%) | 168 (46%) | 0.06 | 80 (46%) | 232 (33%) | 0.004 |
| White | 46 (48%) | 232 (68%) | 19 (24%) | 117 (32%) | 65 (37%) | 349 (49%) | |||
| Other | 17 (18%) | 46 (14%) | 12 (15%) | 80 (22%) | 29 (17%) | 126 (18%) | |||
|
| |||||||||
| High-risk | |||||||||
| Yes | 32 (34%) | 103 (30%) | 0.51 | 26 (33%) | 123 (34%) | 0.90 | 58 (33%) | 226 (32%) | 0.73 |
|
| |||||||||
| Insurance | |||||||||
| Private | 16 (17%) | 64 (19%) | 0.87 | 16 (20%) | 65 (18%) | 0.75 | 32 (18%) | 129 (18%) | 0.92 |
| Public | 77 (81%) | 269 (79%) | 63 (80%) | 298 (82%) | 140 (80%) | 567 (80%) | |||
| Unknown | 2 (2%) | 9 (3%) | 0 (0%) | 2 (1%) | 2 (1%) | 11 (2%) | |||
|
| |||||||||
| ** Influenza vaccine status | |||||||||
| Full | 17 (20%) | 71 (24%) | 0.16 | 3 (4%) | 49 (16%) | 0.002 | 20 (12%) | 120 (20%) | 0.002 |
| Partial | 11 (13%) | 58 (20%) | 6 (8%) | 45 (15%) | 17 (10%) | 103 (17%) | |||
| Unvaccinated | 59 (68%) | 169 (57%) | 69 (88%) | 206 (69%) | 128 (78%) | 375 (63%) | |||
Others includes biracial children and children of other race and/or ethnicity.
Limited to verified vaccination status among children eligible for vaccine (≥6 months of age). Influenza vaccination status could not be confirmed for16 influenza negative and 6 influenza-positive children in Knoxville. Two influenza-positive and 28 influenza-negative children were not age-eligible for vaccine from Knox County; in Davidson County the respective numbers of children were 1 and 65.
Figure 1.

Proportion of children 0–12 years of age who were influenza-positive during the 18-week influenza season by age group and county.
More influenza-positive than influenza-negative children had subjective fever (96% versus 74%, p<0.001), nasal congestion (91% versus 85%, p=0.04) and poor appetite (79% versus 62%, p<0.001), whereas cough (91% versus 86%, p=0.09) was similar in both groups. More influenza-positive than influenza-negative children aged 5–12 years had headache (69% versus 54%, p=0.01) and myalgia (43% versus 29%, p=0.02), whereas sore throat (66% versus 62%, p=0.46) was similar in both groups.
3.3. Proportion Influenza-positive
In Knox County, 95 (22%) of 437 eligible children had laboratory-confirmed influenza infections—16% influenza A and 6% influenza B (Figure 2A). In Davidson County, 79 (18%) of 444 eligible children had influenza—10% influenza A and 8% influenza B; one child had both influenza A and B (Figure 2B). The proportion of children with influenza was similar in both counties (p=0.14), with influenza A preceding influenza B in both counties. More Knox than Davidson County children aged 0–4 years had influenza infection (18% versus 10%, p=0.01), whereas similar proportions of children aged 5–12 years had influenza infections (28% versus 27%, p=0.85). Patterns were similar in an analysis confined to the ED; small numbers enrolled in the Knox County clinic setting precluded a separate analysis of that setting.
Figure 2.


Figure 2A. Proportion of children 0–12 years of age who were influenza A or B positive during each week of the 18-week influenza season in Knox County
Figure 2B. Proportion of children 0–12 years of age who were influenza A or B positive during each week of the 18-week influenza season in Davidson County
*One Davidson County child in week 1 had an influenza A and B infection.
3.4. Influenza Match
Thirty-six influenza isolates from Knox (N=22) and Davidson County (N=14) were sent to the CDC for characterization. The proportions characterized as good match, minor antigenic variant, and poor match were similar in Knox and Davidson Counties (50%, 45% and 5% versus 64%, 21% and 14%, p=0.27).
3.5. Vaccination Status
Influenza vaccination status was verified for 95% and 100% of Knox and Davidson County children, respectively. In Knox County, the proportion of children who had influenza vaccination status verified did not differ by age group, influenza disease status, type of insurance (public or private) or enrollment setting. In both counties, children enrolled in the clinic were more likely to be vaccinated than children enrolled in the ED. Although a higher proportion of children aged 5–12 years were vaccinated in Knox than Davidson County in both settings, we limited the analysis to a comparison of children enrolled in the ED only to maximize comparability of the study populations. Similar proportions of children aged 0.5–4 years in the ED had any verified influenza vaccinations in both Knox and Davidson Counties (36% versus 33%, p=0.69, Figure 3). In contrast, more Knox than Davidson County children aged 5–12 years (44% versus 12%, p<0.001) were vaccinated.
Figure 3.
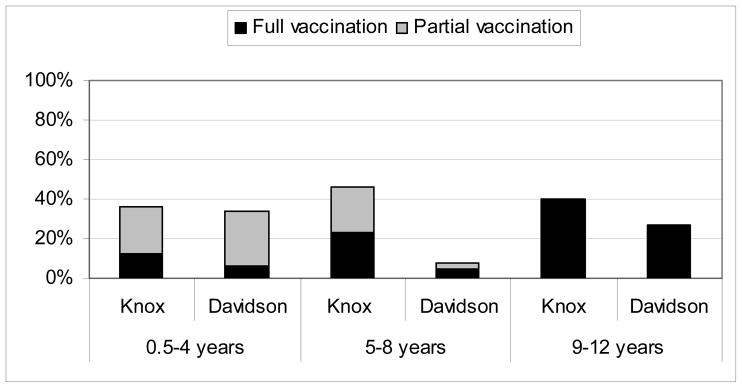
Influenza vaccination status of influenza-negative children 0.5–12 years of age enrolled in the ED by age group in Knox County and Davidson County.
4. Discussion
Our study demonstrated that 20% of children <13 years with ARI or fever in both Tennessee counties during the 2006–2007 season had laboratory-confirmed influenza infections. More school-age than preschool-age children were influenza-positive, indicating the large burden of influenza in school-age children and supporting the expansion of the ACIP recommendations to all school-age children.[23] Estimated influenza vaccine coverage in preschool-age children in both counties was comparable, likely resulting from the ACIP and AAP recommendations for universal annual influenza vaccination of all children aged 0.5–4 years.[11] However, despite similar vaccine coverage, the proportion of preschool children with influenza infection was almost twice as high in Knox as in Davidson County, possibly suggesting that the influenza season was more severe in Knox County. Estimated vaccination coverage among school-age children in the ED was higher in Knox than Davidson County, highlighting the success of the Knox County school-based influenza vaccine campaign. Yet, differences in vaccination coverage in the school-age children did not translate into lower proportion of laboratory-confirmed influenza illnesses in Knox County.
Several reasons may have contributed to our inability to detect a difference in the proportion of all children with laboratory-confirmed influenza infection in the two counties, our primary study objective. First, based on prediction models,[22] our study was only powered to detect 40% less influenza in the intervention than the control county, assuming that the school-based immunization program would have a major effect on county influenza burden. After initiating this study, several published manuscripts suggested that this prediction model likely overestimates the indirect prevention,[24–26] and our results support this conclusion. Certainly, the school-based immunization campaign in Knox County did not stop the influenza epidemic, and we were unable to show large differences between these two counties. The fact that only two counties were studied with more similar vaccine coverage than anticipated limited our ability to detect small differences. An estimated 12% of children aged 5–12 years in Davidson County were vaccinated, which is higher than we anticipated. Hence, we were, in effect, trying to detect direct and indirect benefits of vaccination in children with an estimated absolute difference in vaccination coverage of school-age children in the two counties of only 32% and with no differences in vaccination coverage in younger children. Second, each influenza season varies yearly and by geographic site. Although Knox and Davidson County are only 180 miles apart, the severity of the influenza season between the two counties might have varied, even without the school-based influenza vaccine initiative in Knox County. The higher proportion of influenza-positive preschool children in Knox County with similar vaccine coverage suggests that the influenza season may have been more severe in Knox County. If so, then the similar burden of influenza in school-age children is consistent with a direct benefit of the vaccination campaign in Knox County as compared to Davidson County.
Our study has several other limitations. This study was limited to children aged <13 years, and to only one ED and one outpatient clinic in each county. The impact of vaccinating children on the influenza disease burden of adults is important, especially given recent studies suggesting that previous studies overestimated the influenza vaccine effectiveness in elderly adults.[27] A separate but concurrent study was performed in Knox County that assessed the risk of laboratory-confirmed influenza hospitalizations in adults.[28] Because there is annual variation in influenza severity, geographic variability within each season and variability in the extent to which influenza vaccine matches circulating strains, further studies are needed to better appreciate the impact of school-based vaccinations. The lower than expected vaccine impact might have resulted from the fact that only one (A H1N1) of four circulating strains (other three: A H3N2 and two B strains) was a good match to the 2006–2007 influenza vaccine.[29] Yet, from the 36 samples tested, there was no obvious difference in vaccine match among isolated viral strains between the two counties.
Our results are consistent with several other studies. Influenza is a common cause of ARI and fever among outpatient children with an even higher proportion of ARI visits due to influenza among school-age than preschool-age children.[6] During the 18-week influenza season in 2006–2007, 22% of children aged 0–12 years with fever or ARI had influenza, which is within the reported range of 9% to 39% for laboratory-confirmed influenza in children.[29–31] In Knox and Davidson Counties, providers had similar success in vaccinating the recommended age group of children 0.5–4 years during that season, and estimated vaccination rates were comparable to estimates using immunization information systems.[32] The school-based campaign did increase vaccinations in school-age children and coverage estimates were comparable to other school-based influenza immunization program; 47% vaccinated in 11 schools, 40% vaccinated in 3 elementary schools, and 45% of children in Knox County in the previous season.[14;24;33]
In summary, influenza was associated with a significant burden of illness despite a school-based influenza campaign and moderate adherence to recommendations to vaccinate children aged <5 years. Influenza was responsible for a greater proportion of ARI visits among school-age than preschool-age children, supporting the anticipated expansion of the influenza vaccine recommendation to all children aged 0.5–18 years.[34] The data from the two counties are consistent with a direct benefit of the vaccination campaign for school-age children, but do not suggest any substantial indirect effect in younger children. Herd effects may require higher vaccination rates and/or a better match of vaccines with the circulating influenza strains.
Acknowledgments
We thank our study nurses and coordinators Caroline Graber RN, Jacque Van Audenhove MS, Karen Carson RN, Shirley McDowell RN, and Letty Dolin RN in Knoxville, and Diane Kent RN, Ann Clay RN, Dayna Wyatt RN and Mariah Daly RN in Nashville; Martha Buchanan, MD, Director of the Knox County Health Department; Amy Herrygers and Jody Peters who performed the cultures and polymerase chain reactions; Shannon Dyer who managed the data; Paul Harris, PhD and Carlos Orozco at Vanderbilt University who designed and implemented the data entry system. We thank all the children and their parents who generously participated in this study. We also thank the anonymous reviewers whose insights significantly enhanced this work.
Footnotes
Disclosures:
Funding for this study was through multiple sources. An investigator-initiated grant from MedImmune supported the Knox County surveillance activities and the data analysis. MedImmune had no role in the design and conduct of study, collection, management, analysis, or interpretation; preparation, review, or approval of manuscript.
CDC has funded influenza surveillance among children in Davidson County through the NVSN since 2000. CDC did not fund any other aspects of this study and was not involved with the vaccine evaluation.
Dr. Griffin, Dr. Edwards and Mr. Lott have received grant support from MedImmune. Mr. Lott is a speaker for MedImmune. Dr. Williams has served as a consultant for MedImmune. Dr. Talbot has received research funding from Wyeth and Protein Sciences. Dr. Edwards has received grant support from Sanofi-Pasteur, Wyeth, Novartis and GlaxoSmithKline and serves as consultant to PATH. Knox County Health Department received free vaccine from MedImmune for the school-based program.
Dr. Talbot received salary support and career development from the National Center for Research Resources (5 K12 RR017697-05). Drs. Talbot (K23 AI074863) and Poehling (K23 AI065805) received support from the National Institute of Allergy and Infectious Diseases. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources, National Institute of Allergy and Infectious Diseases or National Institutes of Health. The data management effort was supported by Vanderbilt General Clinical Research Center (M01 RR-00095), supported by the National Center for Research Resources, National Institutes of Health. Dr. Poehling also received support from Wachovia Research Fund.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Hing E, Cherry DK, Woodwell DA. Advance data from vital and health statistics. 374. Hyattsville, MD: National Center for Health Statistics; 2006. National Ambulatory Medical Care Survey: 2004 summary. [PubMed] [Google Scholar]
- 2.Heikkinen T, Silvennoinen H, Peltola V, et al. Burden of influenza in children in the community. J Infect Dis. 2004;190(8):1369–73. doi: 10.1086/424527. [DOI] [PubMed] [Google Scholar]
- 3.Poehling KA, Edwards KM, Weinberg GA, et al. The underrecognized burden of influenza in young children. N Engl J Med. 2006;355(1):31–40. doi: 10.1056/NEJMoa054869. [DOI] [PubMed] [Google Scholar]
- 4.Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpandemic influenza in children younger than 5 years: a 25-year prospective study. J Infect Dis. 2002;185(2):147–52. doi: 10.1086/338363. [DOI] [PubMed] [Google Scholar]
- 5.Fox JP, Hall CE, Cooney MK, Foy HM. Influenzavirus infections in Seattle families, 1975–1979. I. Study design, methods and the occurrence of infections by time and age. Am J Epidemiol. 1982;116(2):212–27. doi: 10.1093/oxfordjournals.aje.a113407. [DOI] [PubMed] [Google Scholar]
- 6.Long CE, Hall CB, Cunningham CK, et al. Influenza surveillance in community-dwelling elderly compared with children. Arch Fam Med. 1997;6(5):459–65. doi: 10.1001/archfami.6.5.459. [DOI] [PubMed] [Google Scholar]
- 7.Bridges CB, Fukuda K, Uyeki TM, Cox NJ, Singleton JA. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2002;51(RR-3):1–31. [PubMed] [Google Scholar]
- 8.Bridges CB, Harper SA, Fukuda K, Uyeki TM, Cox NJ, Singleton JA. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2003;52(RR-8):1–34. [PubMed] [Google Scholar]
- 9.Harper SA, Fukuda K, Uyeki TM, Cox NJ, Bridges CB. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2004;53(RR-6):1–40. [PubMed] [Google Scholar]
- 10.Harper SA, Fukuda K, Uyeki TM, Cox NJ, Bridges CB. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2005;54(RR-8):1–40. [PubMed] [Google Scholar]
- 11.Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA. Prevention and Control of Influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Recomm Rep. 2006;55(RR-10):1–42. [PubMed] [Google Scholar]
- 12.Fiore AE, Shay DK, Broder K, et al. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2008. MMWR Recomm Rep. 2008;57(Early Release):1–60. [PubMed] [Google Scholar]
- 13.Prevention of influenza: recommendations for influenza immunization of children, 2008–2009. Pediatrics. 2008;122(5):1135–41. doi: 10.1542/peds.2008-2449. [DOI] [PubMed] [Google Scholar]
- 14.Carpenter LR, Lott J, Lawson BM, et al. Mass distribution of free, intranasally administered influenza vaccine in a public school system. Pediatrics. 2007;120(1):e172–8. doi: 10.1542/peds.2006-2603. [DOI] [PubMed] [Google Scholar]
- 15.Grijalva CG, Zhu Y, Griffin MR. Evidence of effectiveness from a large county-wide school-based influenza immunization campaign. Under review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.U.S. Census. [Accessed on January 8, 2009];U S Census Bureau. 2006 Available from: URL: www.factfinder.census.gov.
- 17.Kandun IN, Wibisono H, Sedyaningsih ER, et al. Three Indonesian clusters of H5N1 virus infection in 2005. N Engl J Med. 2006;355(21):2186–94. doi: 10.1056/NEJMoa060930. [DOI] [PubMed] [Google Scholar]
- 18.Mehlmann M, Bonner AB, Williams JV, et al. Comparison of the MChip to viral culture, reverse transcription-PCR, and the QuickVue influenza A+B test for rapid diagnosis of influenza. J Clin Microbiol. 2007;45(4):1234–7. doi: 10.1128/JCM.02202-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Raff T, van der GM, Endemann D, Wiederholt T, Paul M. Design and testing of beta-actin primers for RT-PCR that do not co-amplify processed pseudogenes. Biotechniques. 1997;23(3):456–60. doi: 10.2144/97233st02. [DOI] [PubMed] [Google Scholar]
- 20.Fields WR, Desiderio JG, Putnam KP, Bombick DW, Doolittle DJ. Quantification of changes in c-myc mRNA levels in normal human bronchial epithelial (NHBE) and lung adenocarcinoma (A549) cells following chemical treatment. Toxicol Sci. 2001;63(1):107–14. doi: 10.1093/toxsci/63.1.107. [DOI] [PubMed] [Google Scholar]
- 21.Erdman DD, Weinberg GA, Edwards KM, et al. GeneScan reverse transcription-PCR assay for detection of six common respiratory viruses in young children hospitalized with acute respiratory illness. J Clin Microbiol. 2003;41(9):4298–303. doi: 10.1128/JCM.41.9.4298-4303.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Weycker D, Edelsberg J, Halloran ME, et al. Population-wide benefits of routine vaccination of children against influenza. Vaccine. 2005;23(10):1284–93. doi: 10.1016/j.vaccine.2004.08.044. [DOI] [PubMed] [Google Scholar]
- 23.Fiore AE, Shay DK, Broder K, et al. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2008. MMWR Recomm Rep. 2008;57(Early Release):1–60. [PubMed] [Google Scholar]
- 24.King JC, Jr, Stoddard JJ, Gaglani MJ, et al. Effectiveness of school-based influenza vaccination. N Engl J Med. 2006;355(24):2523–32. doi: 10.1056/NEJMoa055414. [DOI] [PubMed] [Google Scholar]
- 25.Davis MM, King JC, Jr, Moag L, Cummings G, Magder LS. Countywide school-based influenza immunization: direct and indirect impact on student absenteeism. Pediatrics. 2008;122(1):e260–5. doi: 10.1542/peds.2007-2963. [DOI] [PubMed] [Google Scholar]
- 26.Piedra PA, Gaglani MJ, Kozinetz CA, et al. Trivalent live attenuated intranasal influenza vaccine administered during the 2003–2004 influenza type A (H3N2) outbreak provided immediate, direct, and indirect protection in children. Pediatrics. 2007;120(3):e553–64. doi: 10.1542/peds.2006-2836. [DOI] [PubMed] [Google Scholar]
- 27.Jackson LA, Jackson ML, Nelson JC, Neuzil KM, Weiss NS. Evidence of bias in estimates of influenza vaccine effectiveness in seniors. Int J Epidemiol. 2006;35(2):337–44. doi: 10.1093/ije/dyi274. [DOI] [PubMed] [Google Scholar]
- 28.Talbot HK, Poehling K, Williams JV, et al. Influenza in Older Adults:Impact of Vaccination of School Children. Under review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Centers for Disease Control and Prevention. [Accessed on January 8, 2009];US Flu Activity. Available from: URL: http://www.cdc.gov/flu/weekly/fluactivity.htm.
- 30.Principi N, Esposito S, Marchisio P, Gasparini R, Crovari P. Socioeconomic impact of influenza on healthy children and their families. Pediatr Infect Dis J. 2003;22 (10 Suppl):S207–10. doi: 10.1097/01.inf.0000092188.48726.e4. [DOI] [PubMed] [Google Scholar]
- 31.Principi N, Esposito S, Gasparini R, Marchisio P, Crovari P. Burden of influenza in healthy children and their households. Arch Dis Child. 2004;89(11):1002–7. doi: 10.1136/adc.2003.045401. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 32.Conklin M, Berry K, Enger K, et al. Influenza vaccination coverage among children aged 6–59 months--six immunization information system sentinel sites, United States, 2006–07 influenza season. MMWR Morbidity and Mortality Weekly Report. 2007;56:963–5. [PubMed] [Google Scholar]
- 33.King JC, Jr, Cummings GE, Stoddard J, et al. A pilot study of the effectiveness of a school-based influenza vaccination program. Pediatrics. 2005;116(6):e868–73. doi: 10.1542/peds.2005-1301. [DOI] [PubMed] [Google Scholar]
- 34.Fiore AE, Shay DK, Broder K, et al. Prevention and control of influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2008. MMWR Recomm Rep. 2008;57(Early Release):1–60. [PubMed] [Google Scholar]