

Abstract
Latissimus dorsi transfer is a well-established method for the treatment of posterosuperior massive irreparable rotator cuff tears. We propose using an arthroscopically assisted technique that avoids insult to the deltoid. With the patient in the lateral decubitus position, an L-shaped incision is made along the anterior belly of the latissimus muscle and then along the posterior axillary line. The latissimus and teres major are identified and separated. The tendon insertion of the latissimus is isolated, and a FiberWire traction suture (Arthrex, Naples, FL) is placed, facilitating dissection of the muscle to the thoracodorsal neurovascular pedicle and subsequent mobilization. The interval deep to the deltoid and superficial to the teres minor is developed into a subdeltoid tunnel for arthroscopic tendon transfer. The latissimus tendon is then transferred and stabilized arthroscopically to the lateral aspect of the infraspinatus and supraspinatus footprints by multiple suture anchors.
Massive rotator cuff tears can be associated with severe functional impairment and disabling pain that may not respond to conservative treatment. Although previous studies have shown that conservative treatment options have beneficial outcomes, the long-term results are less promising.1,2 Large tendon tears are associated with severe fatty infiltration1 and atrophy of the respective muscles that can prevent repair by conventional methods.3 These changes are irreversible even if direct repairs are structurally successful.4 The most common of these irreparable rotator cuff tears is loss of supraspinatus and infraspinatus muscle-tendon-bone continuity. Tearing of these tendons leads to loss of active external rotation and the inability to stabilize the arm in space. Transfer of the latissimus dorsi tendon as a treatment option for irreparable rotator cuff tears was originally described by Gerber et al.5 in 1988. The procedure has been supported by biomechanical investigations and clinical reports showing significant improvement in patients’ pain and function.6-12 Therefore latissimus dorsi muscle transfer has become the preferred treatment for active disabled patients with a posterosuperior irreparable cuff tear and a functional deltoid.13 We present an arthroscopically assisted technique for latissimus dorsi transfer for massive irreparable rotator cuff tear that avoids insult to the deltoid.
Technique
Video 1 presents a clear demonstration of our technique. The patient is placed in the lateral decubitus position with the entire arm and hemithorax prepared by sterile technique (Figs 1-4). The operative arm is held throughout the procedure by an articulated hydraulic arm holder (Spider Arm Positioner; Tenet Medical Engineering, Calgary, Alberta, Canada). Exposure of the latissimus dorsi is facilitated by placing the arm into flexion, abduction, and internal rotation. An L-shaped incision is made along the anterior belly of the latissimus muscle and then along the posterior axillary line. Curving the incision laterally at its proximal portion makes exposure of the tendon insertion easier. The latissimus dorsi is dissected from its attachments to the anterior chest wall, and then the interval between the latissimus dorsi and teres major is identified. The 2 muscles may be conjoined at the insertion site in some patients. However, with careful dissection, one is able to accurately identify and separate the 2 insertion sites. The tendon insertion of the latissimus is isolated, and a FiberWire traction suture (Arthrex, Naples, FL) is placed, facilitating resection of the tendon off the humerus. The dissection proceeds proximally to identify and pro-tect the thoracodorsal neurovascular pedicle, which will allow for safe mobilization of the latissimus dorsi musculotendinous unit. The muscle-tendon unit is then mobilized to reach the top of the acromion, avoiding excessive tension on the pedicle. Given the very thin and diminutive nature of the latissimus tendon, we prefer to augment the tendon with allograft tissue. Either a strip of Achilles or double-looped semitendinosus allograft is used for augmentation. This is clearly illustrated in Video 1. In addition to reinforcing the insertion site, the augmentation allows the transfer to be lengthened if needed. In our experience, with identification and protection of the neurovascular pedicle, proper mobilization of the latissimus muscle has not been a problem. The allograft is laid on the superior portion of the latissimus dorsi and then secured from the tendon end distally to the musculotendinous junction. This is achieved with nonabsorbable No. 2 FiberWire suture (Arthrex) along the length of the tendon and graft.
Fig 1.
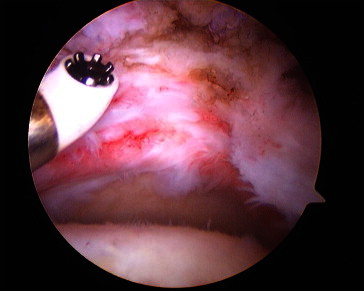
Assessment of subacromial space from standard posterior arthroscopy portal.
Fig 2.
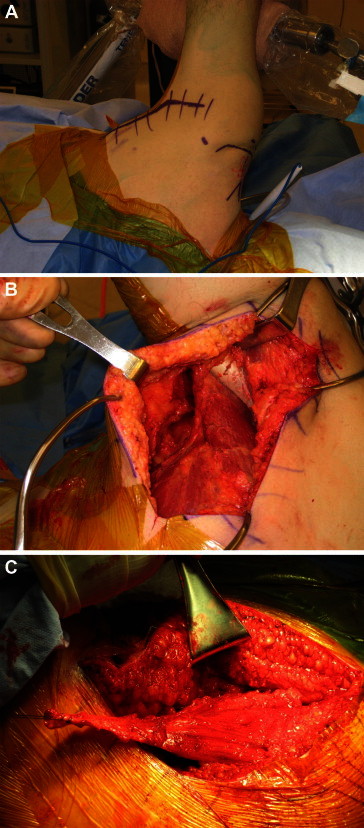
(A) Patient in lateral decubitus position with markings for latissimus dorsi harvest, arthroscopic portals, and mapped-out acromion. (B, C) Harvest of latissimus dorsi.
Fig 3.
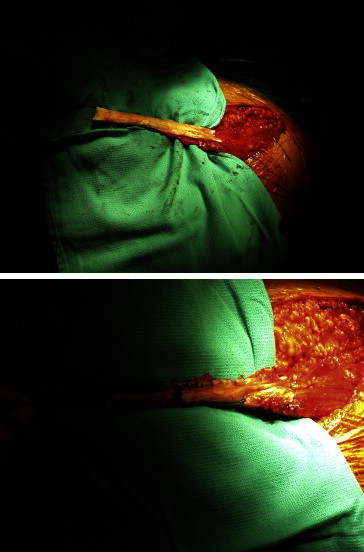
Tendon augmentation with allograft.
Fig 4.
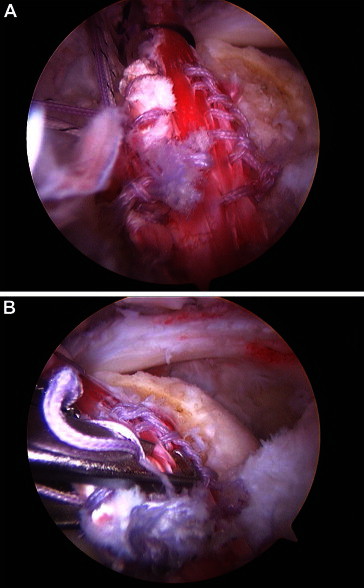
(A) Posterior portal view of arthroscopic transfer of tendon into joint. (B) Suture placement into tendon.
Attention is now turned to diagnostic arthroscopy of the glenohumeral joint and the subacromial space using a standard posterior arthroscopy portal. The remaining rotator cuff is assessed for mobility, and if possible, limited releases are performed to increase some of the excursion of the remaining posterior rotator cuff tissue. The planned insertion site for the tendon transfer is then prepared by lightly decorticating the lateral aspect of the supraspinatus and infraspinatus footprint. A total of 4 to 5 Arthrex 5.5 mm BioCorkscrew suture anchors double loaded with No. 2 FiberWires are placed medially and laterally in a staggered configuration within the lateral aspect of the footprint.
Next, the interval deep to the deltoid and superficial to the teres minor is developed by blunt dissection to create a subdeltoid tunnel. A curved clamp loaded with the traction sutures from the graft is then carefully passed underneath the acromion into the subacromial space under direct arthroscopic visualization. The tendon is transferred arthroscopically into the joint by pulling the traction sutures out of the anterior portal under tension.
Once in the subacromial space, the transferred tendon is pulled over the top of the humeral head. Suture placement into the tendon is accomplished in all-arthroscopic manner by a Scorpion Suture Passer (Arthrex). The working portal for instrumentation is either the anterior-lateral or posterior-lateral portal. The arm is then placed in approximately 45° of abduction and 45° of external rotation to tension the transfer. The transferred tendon is secured to the previously placed suture anchors starting with the posterior-most anchor and working anteriorly. Once secured to the greater tuberosity, the anterior edge of the transferred tendon is then fixed to the subscapularis with free No. 2 FiberWire. Finally, any remaining and sufficiently mobile native posterior rotator cuff is attached to the posterior-medial edge of the transferred tendon with nonabsorbable suture by use of a Scorpion Suture Passer device. The arm is taken through range of motion, and the stability and tension on the transfer are assessed.
Postoperatively, the patient is placed in an abduction and external rotation orthosis for the first 6 weeks to allow the tendon to heal without tension. A physical therapist performs passive motion of the arm in abduction and external rotation, not allowing internal rotation or adduction. At 6 weeks, the patient is allowed to start active-assisted and active range of motion. At 3 to 4 months, initiation of a biofeedback program is begun to retrain the latissimus dorsi muscle, an adductor and internal rotator, to now function as an active elevator and external rotator of the shoulder. Strengthening is begun once the patient has achieved latissimus contraction during elevation.
Discussion
Massive, irreparable rotator cuff tears present a difficult challenge to the clinician. Direct repair of the rotator cuff may not be possible if there is associated irreversible atrophy of rotator cuff muscles and advanced functional impairment.3,14,15 The technique discussed in this article was used exclusively for such irreparable tears occurring to the posterior-superior rotator cuff. Latissimus dorsi transfer, whether performed in an open manner or with arthroscopic assistance, is a technically demanding procedure. As has occurred with many other shoulder procedures, arthroscopic techniques allow for less invasive surgery that often replaces open surgery. Open transfer requires violation of the deltoid for attachment of the transferred latissimus tendon. The main advantage of the arthroscopically assisted latissimus transfer technique presented in this article is the avoidance of any major deltoid damage.
Previous studies evaluating clinical outcome of latissimus transfer have found that both subscapularis and deltoid function can affect the clinical outcome of the procedure.13,16-18 Gumina et al.19 found that when treating massive rotator cuff tears, injury to the deltoid muscle may lead to inferior results. Biomechanically, the deltoid is unable to regain pre-existing strength after an open latissimus dorsi transfer procedure.20 Preserving the deltoid through this arthroscopic technique may provide a better clinical outcome in patients undergoing latissimus dorsi transfer for massive rotator cuff tears. In addition, the known risk and devastating complication of deltoid injury, and possible detachment, after open subacromial surgery is therefore completely avoided.21
The goal of this article is to propose a new surgical technique that may improve upon existing methods. Our experiences with an initial 8 patients who have undergone this surgery show favorable results. All sustained an irreparable rotator cuff injury. These patients (age range, 49-60 years; mean age, 54 years) were examined and followed up extensively for a mean of 14 months. Range of motion, pain (visual analog pain score), and function (shoulder score index) were assessed preoperatively and postoperatively. On average, there was a 2-point reduction (7 to 5) in pain and 7-point improvement (63 to 70) in functional score after surgery. Furthermore, on average, there was a 40° increase in shoulder abduction, an 11° increase in external rotation, and a 33° increase in forward flexion. The preliminary data suggest that the surgical technique may improve patient’s pain, range of motion, and function. We believe that these results warrant further investigation of the technique.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary data
The patient is placed in the right lateral decubitus position, and the arm is placed in flexion, abduction, and internal rotation. An L-shaped incision is marked out along the anterior belly of the latissimus muscle. Partial dissection of the latissimus from the chest wall is performed. The interval between the latissimus and teres major is identified. A FiberWire traction suture is placed in the tendon, facilitating the resection from the humerus. Dissection both to mobilize the latissimus and to identify and protect the neurovascular pedicle is performed. Full mobilization of the muscle-tendon unit is performed to reach the top of the acromion. The latissimus tendon is augmented with an Achilles allograft. The allograft is secured from the tendon end distally with nonabsorbable No. 2 FiberWire suture. An arthroscopic view from the posterior portal of the glenohumeral joint and subacromial space is established. The remaining rotator cuff is assessed for mobility, and a limited release is performed. Preparation of the insertion site is performed by lightly decorticating the lateral aspect of the supraspinatus and infraspinatus footprint. Four BioCorkscrew suture anchors double loaded with No. 2 FiberWires are placed medially and laterally. The interval deep to the deltoid and superficial to the teres minor is developed. The graft is carefully passed through the tunnel into the subacromial space under direct arthroscopic visualization from the anterolateral portal. The traction sutures are pulled out through the anterior portal by use of alligator graspers. The transferred tendon is pulled over the top of the humeral head. The arm is placed in approximately 45° of abduction and 45° of external rotation to tension the transfer. A SwiveLock suture anchor (Arthrex) is used to fix the graft anteriorly. The transferred tendon is secured to the previously placed suture anchors. The remaining native posterior cuff is attached to the posterior-medial edge of the transferred tendon. The patient is placed in an abduction and external rotation orthosis.
References
- 1.Baydar M., Akalin E., El O. The efficacy of conservative treatment in patients with full-thickness rotator cuff tears. Rheumatol Int. 2009;29:623–628. doi: 10.1007/s00296-008-0733-2. [DOI] [PubMed] [Google Scholar]
- 2.Zingg P.O., Jost B., Sukthankar A., Buhler M., Pfirrmann C.W., Gerber C. Clinical and structural outcomes of nonoperative management of massive rotator cuff tears. J Bone Joint Surg Am. 2007;89:1928–1934. doi: 10.2106/JBJS.F.01073. [DOI] [PubMed] [Google Scholar]
- 3.Goutallier D., Postel J.M., Gleyze P., Leguilloux P., Van Driessche S. Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg. 2003;12:550–554. doi: 10.1016/s1058-2746(03)00211-8. [DOI] [PubMed] [Google Scholar]
- 4.Gerber C., Fuchs B., Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82:505–515. doi: 10.2106/00004623-200004000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Gerber C., Vinh T.S., Hertel R., Hess C.W. Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff. A preliminary report. Clin Orthop Relat Res. 1988:51–61. [PubMed] [Google Scholar]
- 6.Schoierer O., Herzberg G., Berthonnaud E., Dimnet J., Aswad R., Morin A. Anatomical basis of latissimus dorsi and teres major transfers in rotator cuff tear surgery with particular reference to the neurovascular pedicles. Surg Radiol Anat. 2001;23:75–80. doi: 10.1007/s00276-001-0075-1. [DOI] [PubMed] [Google Scholar]
- 7.Herzberg G., Urien J.P., Dimnet J. Potential excursion and relative tension of muscles in the shoulder girdle: Relevance to tendon transfers. J Shoulder Elbow Surg. 1999;8:430–437. doi: 10.1016/s1058-2746(99)90072-1. [DOI] [PubMed] [Google Scholar]
- 8.Magermans D.J., Chadwick E.K., Veeger H.E., Rozing P.M., van der Helm F.C. Effectiveness of tendon transfers for massive rotator cuff tears: A simulation study. Clin Biomech (Bristol, Avon) 2004;19:116–122. doi: 10.1016/j.clinbiomech.2003.09.008. [DOI] [PubMed] [Google Scholar]
- 9.Glousman R., Jobe F., Tibone J., Moynes D., Antonelli D., Perry J. Dynamic electromyographic analysis of the throwing shoulder with glenohumeral instability. J Bone Joint Surg Am. 1988;70:220–226. [PubMed] [Google Scholar]
- 10.Myers J.B., Riemann B.L., Ju Y.Y., Hwang J.H., McMahon P.J., Lephart S.M. Shoulder muscle reflex latencies under various levels of muscle contraction. Clin Orthop Relat Res. 2003:92–101. doi: 10.1097/00003086-200302000-00017. [DOI] [PubMed] [Google Scholar]
- 11.Cleeman E., Hazrati Y., Auerbach J.D., Shubin Stein K., Hausman M., Flatow E.L. Latissimus dorsi tendon transfer for massive rotator cuff tears: A cadaveric study. J Shoulder Elbow Surg. 2003;12:539–543. doi: 10.1016/s1058-2746(03)00206-4. [DOI] [PubMed] [Google Scholar]
- 12.Donaldson J., Pandit A., Noorani A., Douglas T., Falworth M., Lambert S. Latissimus dorsi tendon transfers for rotator cuff deficiency. Int J Shoulder Surg. 2011;5:95–100. doi: 10.4103/0973-6042.91002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Warner J.J., Gerber C. Treatment of massive rotator cuff tears: Posterior-superior and anterior-superior. In: Iannotti J.P., editor. The rotator cuff: Current concepts and complex problems. American Academy of Orthopaedic Surgeons; Rosemont, IL: 1998. pp. 59–94. [Google Scholar]
- 14.Patte D., Goutallier D., Debeyre J. Ruptures of the rotator cuff. Results and perspectives of the retrostructure (author’s transl) Orthopade. 1981;10:206–215. (in German) [PubMed] [Google Scholar]
- 15.Postacchini F., Gumina S. Results of surgery after failed attempt at repair of irreparable rotator cuff tear. Clin Orthop Relat Res. 2002:332–341. doi: 10.1097/00003086-200204000-00038. [DOI] [PubMed] [Google Scholar]
- 16.Gerber C., Maquiera G., Espinosa N. Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears. J Bone Joint Surg Am. 2006;88:113–120. doi: 10.2106/JBJS.E.00282. [DOI] [PubMed] [Google Scholar]
- 17.Iannotti J.P., Hennigan S., Herzog R. Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. Factors affecting outcome. J Bone Joint Surg Am. 2006;88:342–348. doi: 10.2106/JBJS.D.02996. [DOI] [PubMed] [Google Scholar]
- 18.Costouros J.G., Espinosa N., Schmid M.R., Gerber C. Teres minor integrity predicts outcome of latissimus dorsi tendon transfer for irreparable rotator cuff tears. J Shoulder Elbow Surg. 2007;16:727–734. doi: 10.1016/j.jse.2007.02.128. [DOI] [PubMed] [Google Scholar]
- 19.Gumina S., Di Giorgio G., Perugia D., Postacchini F. Deltoid detachment consequent to open surgical repair of massive rotator cuff tears. Int Orthop. 2008;32:81–84. doi: 10.1007/s00264-006-0285-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Weening A.A., Willems W.J. Latissimus dorsi transfer for treatment of irreparable rotator cuff tears. Int Orthop. 2010;34:1239–1244. doi: 10.1007/s00264-010-0970-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Groh G., Simoni M., Rolla P., Rockwood C. Loss of deltoid after shoulder operations: An operative disaster. J Shoulder Elbow Surg. 1994;3:243–253. doi: 10.1016/S1058-2746(09)80042-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient is placed in the right lateral decubitus position, and the arm is placed in flexion, abduction, and internal rotation. An L-shaped incision is marked out along the anterior belly of the latissimus muscle. Partial dissection of the latissimus from the chest wall is performed. The interval between the latissimus and teres major is identified. A FiberWire traction suture is placed in the tendon, facilitating the resection from the humerus. Dissection both to mobilize the latissimus and to identify and protect the neurovascular pedicle is performed. Full mobilization of the muscle-tendon unit is performed to reach the top of the acromion. The latissimus tendon is augmented with an Achilles allograft. The allograft is secured from the tendon end distally with nonabsorbable No. 2 FiberWire suture. An arthroscopic view from the posterior portal of the glenohumeral joint and subacromial space is established. The remaining rotator cuff is assessed for mobility, and a limited release is performed. Preparation of the insertion site is performed by lightly decorticating the lateral aspect of the supraspinatus and infraspinatus footprint. Four BioCorkscrew suture anchors double loaded with No. 2 FiberWires are placed medially and laterally. The interval deep to the deltoid and superficial to the teres minor is developed. The graft is carefully passed through the tunnel into the subacromial space under direct arthroscopic visualization from the anterolateral portal. The traction sutures are pulled out through the anterior portal by use of alligator graspers. The transferred tendon is pulled over the top of the humeral head. The arm is placed in approximately 45° of abduction and 45° of external rotation to tension the transfer. A SwiveLock suture anchor (Arthrex) is used to fix the graft anteriorly. The transferred tendon is secured to the previously placed suture anchors. The remaining native posterior cuff is attached to the posterior-medial edge of the transferred tendon. The patient is placed in an abduction and external rotation orthosis.