

Abstract
The labrum is essential for stability, movement, and prevention of arthritis in the hip. In cases of labral damage where repair of a labral tear is not possible, reconstruction can be a useful alternative. Several different autografts have been used, including the iliotibial band (ITB), the ligamentum teres capitis, and the gracilis tendon. Authors have reported both open and arthroscopic techniques for reconstruction with good preliminary results. However, an all-arthroscopic labral reconstruction technique including the graft harvest and reconstruction portions of a labral reconstruction procedure using an ITB autograft has not been previously described. We describe a technique for an all-arthroscopic labral reconstruction performed using a novel method for arthroscopic harvest of the ITB. The decreased invasiveness of our described technique for labral reconstruction may potentially minimize scarring, bodily disfigurement, infection, and postoperative pain associated with the graft harvesting incision.
Numerous advances have been made recently in the arthroscopic management of hip pain and instability. The labrum is essential for stability and movement of the hip,1,2 and thus, in cases where repair of a labral tear is not possible, reconstruction can be a useful alternative.3 An intact labrum can also help to prevent hip degeneration and osteoarthritis of the hip that arises from labral pathology.1,2 For patients with particularly severe injury or degeneration of the hip labrum, in whom labral repair is not a viable option, labral reconstruction techniques have been reported using an iliotibial band (ITB) autograft to replace the irreparable labrum.4 Labral reconstruction may also be indicated in patients who have an insufficient amount of labrum from previous labrum debridement surgery and continue to have symptoms.3
Several different autografts have been used to reconstruct the labrum, including the ITB,4 the ligamentum teres capitis,5 and the gracilis tendon.6 Philippon et al.3,4 reported an arthroscopic labral reconstruction technique using an ITB autograft with an open harvest of the autograft through an incision over the greater trochanter and showed good preliminary results using this technique in a series of 95 patients with a mean follow-up of 18 months. Sierra and Trousdale5 reported a labral reconstruction technique using an open harvest of the ligamentum teres capitis in 5 patients. Matsuda6 recently reported an arthroscopic reconstruction technique using a gracilis tendon autograft harvested through a 2-cm open incision. In addition, Tey et al.7 reported a reconstruction of the labrum using an allogeneic transplant and a mini-anterior open approach. To our knowledge, no reports have described an all-arthroscopic labral reconstruction technique including the graft harvest and reconstruction portions of a labral reconstruction procedure using an ITB autograft. We describe 2 cases of an all-arthroscopic labral reconstruction performed with a novel method for arthroscopic harvest of the ITB.
Clinical Presentation
Case 1
A 37-year-old woman presented initially with symptoms of pain and instability of the left hip. An anteroposterior radiograph showed a mild crossover sign on the acetabulum. Magnetic resonance imaging showed a labral tear and tear of the ligamentum teres. The patient underwent hip arthroscopy, at which point the labrum was deemed irreparable, and the patient subsequently received a debridement of the tear by the senior author (M.A.T.). After 18 months of postoperative pain relief, the patient's symptoms reappeared. The patient also had anterior hip pain with walking and lying down, as well as a decrease in muscle strength, which limited her activities of daily living. Repeat radiographs showed mild subchondral sclerosis (Tönnis grade 1) in the acetabular roof, a magnetic resonance arthrogram showed slight calcification of the remaining labrum, and the articular cartilage showed slight inhomogeneity without any cartilage delamination or flaps. At this time, the patient opted to undergo a labral reconstruction with an ITB autograft performed by the same surgeon. The patient reported resolution of all symptoms at 6 weeks from surgery, and her Vail Hip Score improved from 33 preoperatively to 94 at 1 year postoperatively. Radiographs at 1 year postoperatively did not show any progression of Tönnis grading.
Case 2
A 29-year-old man presented with an 8- to 10-month history of left hip pain after an ice hockey injury, with significantly worsening symptoms in the 2 months before presentation. The magnetic resonance arthrogram showed significant undersurface fraying of the anterosuperior labrum, along with inhomogeneity of the cartilage at the weight-bearing surface. The patient underwent a labral reconstruction because the labrum was irreparable. After labral reconstruction surgery, his Vail Hip Score improved from 41 preoperatively to 90 at 1 year postoperatively.
Surgical Technique
Setup
Each patient undergoes general anesthesia and is placed in a supine position on a Smith & Nephew Hip Distractor (Andover, MA). An extra-wide post is used to protect the perineum, and traction is applied to the ipsilateral extremity to achieve a minimum of 10 to 12 mm of distraction at the hip joint necessary to perform hip arthroscopy. The operative hip is positioned with 10° to 15° of flexion, neutral rotation, and neutral abduction. Fluoroscopy is used to ensure that hip joint distraction is achieved. The traction time is monitored, and the traction is released after every 45 minutes.
Diagnostic Hip Arthroscopy
After a thorough diagnostic arthroscopy with a Smith & Nephew Hip Arthroscopy System, all intra-articular loose bodies are removed. In addition, any fibrous debris overlying the damaged portion of the labrum is excised. At this point, the extent of labral damage is delineated, and the integrity of the remaining labral tissue is assessed. During this diagnostic arthroscopy, if the labrum is deemed unsuitable for repair, the decision is made to proceed with reconstruction with an ITB autograft. Our hip arthroscopy portals used in this procedure are shown in Fig 1 and from an outside view in Fig 2. The recipient site of the acetabular rim is prepared with a Smith & Nephew 4.5-mm full-radius shaver blade and burr if associated retroversion (or crossover sign) needs to be addressed. If not, the recipient site is debrided and roughened to create a bed of healthy bleeding bone. Finally, the recipient site length/deficit is measured with a calibrated probe. The prepared acetabular rim is shown in Fig 3.
Fig 1.
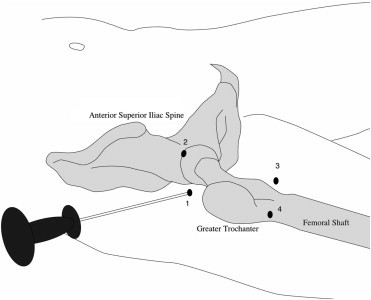
Routine portals for hip arthroscopy: (1) lateral (1 cm proximal and anterior to tip of trochanter), (2) anterior (1 cm lateral to intersection of anterior superior iliac spine line and greater trochanter line), and (3) distal anterolateral for anchor placement (approximately 7-8 cm distal to anterior portal forming a triangle), as well as (4) an additional portal for ITB graft harvest 7 to 8 cm distal and in line with the lateral portal.
Fig 2.

Outside view of surgeon working on arthroscopic graft harvest.
Fig 3.
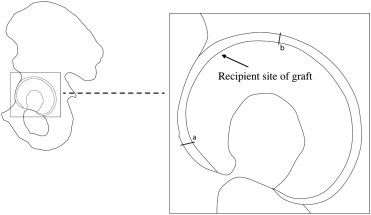
Acetabular rim prepared for labral reconstruction. The section of the acetabular rim prepared as the recipient site is shown from a to b.
Arthroscopic ITB Autograft Harvesting and Preparation of Graft
The hip is taken out of traction, and the femoral cam lesion, if present, is addressed with careful debridement and osteoplasty (Video 1). After decompression of femoroacetabular impingement lesions, attention is diverted to the ITB graft harvest. The peritrochanteric region is then visualized with a 30° arthroscope, and the ITB is delineated. The proximal extent and distal extent of graft harvest sites are confirmed by intraoperative fluoroscopy. A calibrated probe is used to measure the necessary graft. The arthroscopically harvested grafts in the reported cases both measured 2.0 × 6.0 cm. The graft is then prepared with a single modified Krackow locking stitch with No. 2-0 FiberWire (Arthrex, Naples, FL) to make it a tubular structure (Fig 4).
Fig 4.
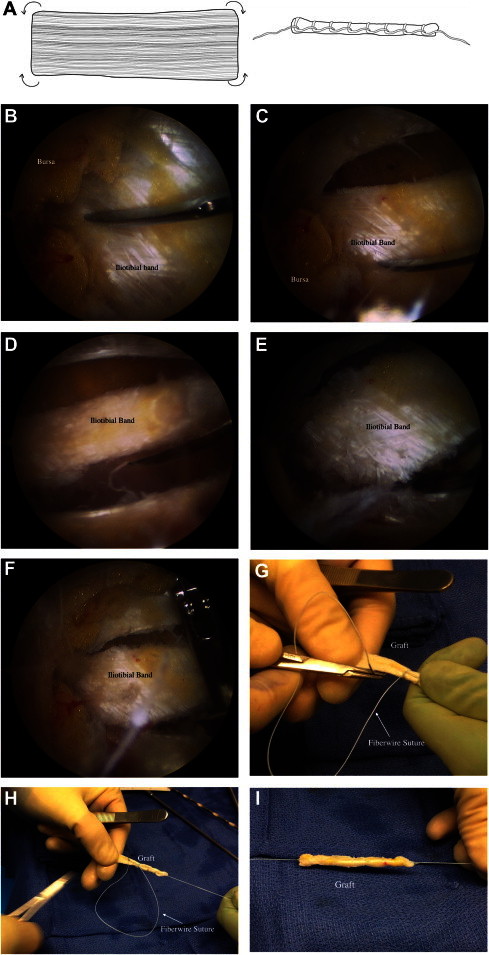
(A) Sketch of ITB graft tissue after harvest and after preparation. (B) The ITB is shown before the start of graft harvest. (C-F) The ITB harvest is completed. (G-I) The harvested ITB is prepared with a single modified Krackow locking stitch.
Insertion of Graft and Suture Management
Traction is reapplied for the reconstruction portion of the procedure. We prefer 8.5 × 110–mm clear-tipped cannulas to assist in graft passage. A low-profile Osteoraptor 2.3-mm suture anchor (Smith & Nephew) with a sliding suture is placed at the most anteromedial portion of the acetabulum that underlies the tear. One end of the Krackow suture on the autograft is attached to the sliding stitch of the suture anchor right next to the graft (Fig 5). The autograft is then pulled into the hip joint through the anterior portal and is secured to the acetabulum with arthroscopic knots. Four to five additional suture anchors are placed 1 cm apart to secure the graft to the acetabular rim. The technique used for securing the remainder of the graft is similar to the technique used for repairing large labral tears. The completed labral reconstruction is shown in Fig 6.
Fig 5.
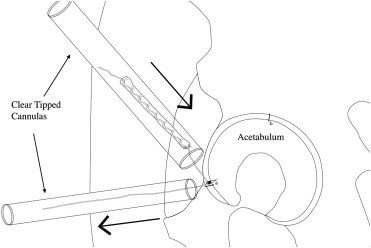
The ITB autograft is inserted into the hip joint through the use of 2 clear-tipped cannulas and a suture anchor containing a sliding suture.
Fig 6.
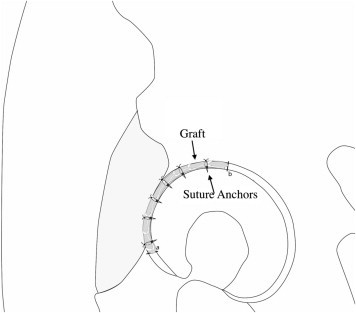
The completed labral reconstruction is shown with suture anchors holding the autologous ITB graft in place.
Postoperative Treatment and Rehabilitation
Labral reconstruction patients are discharged from the outpatient surgery center on the day of surgery. Patients maintain strict non–weight bearing in the operative extremity for 6 weeks and wear a custom-made hip spica brace (Orthomerica, Newport Beach, CA) to limit hip flexion to 30°. Physical therapy focusing on range of motion is implemented from 6 to 12 weeks. Six weeks after surgery, both patients reported no hip pain and were able to return to normal daily activities when use of the hip brace was discontinued. Nonsteroidal anti-inflammatory drugs are specifically avoided during the postoperative period to prevent potential disruption of healing, because previous studies in animal models have shown the detrimental effects of such drugs on healing at the bone-tendon interface.8
Discussion
Arthroscopic labral reconstruction with arthroscopic harvest of the ITB autograft is a minimally invasive option to address a severely damaged labrum. Previous orthopaedic studies have shown potential benefits of minimally invasive approaches for patients. In total hip arthroplasty, Dorr et al.9 have shown that a smaller incision increased patient satisfaction after surgery and gave patients a more positive body image postoperatively, as compared with patients who received a standard-length incision. Mancuso et al.10 found that in patients who underwent total hip arthroplasty, the appearance of a scar was a reason why some patients were dissatisfied with the procedure. Our technique attempts to address this significant patient concern.
Overall, we believe that the advantages of our minimally invasive technique include potential for decreased scarring, bodily disfigurement, and infection after a labral reconstruction procedure. Furthermore, an all-arthroscopic approach minimizes blood loss compared with an open procedure. The risks include the possibility of injury to the ITB during graft harvest, as well as neurovascular injury without proper anatomic knowledge and surgical technique. However, we think that with proper surgical preparation and training, this technique may provide excellent outcomes.
Other reports and preliminary studies of arthroscopic labral reconstruction have shown promising results.3,4 We describe a novel technique to harvest an ITB graft through 2 arthroscopic portals, rather than making an open incision. In addition to possibly reducing the risk of infection and visible scarring of the skin, the use of arthroscopic portals for the graft harvest may also limit postoperative pain associated with the graft harvesting incision. Decreased pain and comorbidity from an all-arthroscopic technique can expedite patient recovery and potentially limit overnight admissions. Both the arthroscopic harvest and reconstruction described earlier require surgeon comfort and skill with hip arthroscopy. Cadaveric simulation may be an appropriate first step in preparing for this surgical technique. We believe an all-arthroscopic technique adds another tool to the hip arthroscopist's surgical armamentarium (Tables 1 and 2).
Table 1.
Potential Prerequisites for All-Arthroscopic ITB Labral Reconstruction
|
Table 2.
Key Points of Procedure
|
Acknowledgment
The authors acknowledge Matthew Wang for his assistance in drawing the figures for this article.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary data
Demonstration of arthroscopic ITB autograft harvest.
References
- 1.Bowman K.F., Jr., Fox J., Sekiya J.K. A clinically relevant review of hip biomechanics. Arthroscopy. 2010;26:1118–1129. doi: 10.1016/j.arthro.2010.01.027. [DOI] [PubMed] [Google Scholar]
- 2.Crawford M.J., Dy C.J., Alexander J.W. The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res. 2007;465:16–22. doi: 10.1097/BLO.0b013e31815b181f. [DOI] [PubMed] [Google Scholar]
- 3.Philippon M.J., Schroder e Souza B.G., Briggs K.K. Labrum: Resection, repair and reconstruction sports medicine and arthroscopy review. Sports Med Arthrosc. 2010;18:76–82. doi: 10.1097/JSA.0b013e3181de376e. [DOI] [PubMed] [Google Scholar]
- 4.Philippon M.J., Briggs K.K., Hay C.J., Kuppersmith D.A., Dewing C.B., Huang M.J. Arthroscopic labral reconstruction in the hip using iliotibial band autograft: Technique and early outcomes. Arthroscopy. 2010;26:750–756. doi: 10.1016/j.arthro.2009.10.016. [DOI] [PubMed] [Google Scholar]
- 5.Sierra R.J., Trousdale R.T. Labral reconstruction using the ligamentum teres capitis: Report of a new technique. Clin Orthop Relat Res. 2009;467:753–759. doi: 10.1007/s11999-008-0633-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Matsuda D.K. Arthroscopic labral reconstruction with gracilis autograft. Arthrosc Tech. 2012;1:e15–e21. doi: 10.1016/j.eats.2011.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tey M., Erquicia J.I., Pelfort X., Miquel J., Gelber P.E., Ribas M. Allogenic labral transplantation in hip instability following arthroscopic labrectomy. Hip Int. 2011;21:260–262. doi: 10.5301/HIP.2011.6524. [DOI] [PubMed] [Google Scholar]
- 8.Ferry S.T., Dahners L.E., Afshari H.M., Weinhold P.S. The effects of common anti-inflammatory drugs on the healing rat patellar tendon. Am J Sports Med. 2007;35:1326–1333. doi: 10.1177/0363546507301584. [DOI] [PubMed] [Google Scholar]
- 9.Dorr L.D., Thomas D., Long W.T., Polatin P.B., Sirianni L.E. Psychologic reasons for patients preferring minimally invasive total hip arthroplasty. Clin Orthop Relat Res. 2007;458:94–100. doi: 10.1097/BLO.0b013e31803212dc. [DOI] [PubMed] [Google Scholar]
- 10.Mancuso C.A., Salvati E.A., Johanson N.A., Peterson M.G., Charlson M.E. Patients' expectations and satisfaction with total hip arthroplasty. J Arthroplasty. 1997;12:387–396. doi: 10.1016/s0883-5403(97)90194-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Demonstration of arthroscopic ITB autograft harvest.