

Abstract
Treatment of concomitant long head of the biceps pathology in the setting of rotator cuff repair is often required. When a tenodesis of the biceps is used, additional anchors and surgical dissection are typically required. This adds additional surgical time, morbidity of additional surgical dissection, and additional anchor load and cost. We describe a novel technique for arthroscopic biceps tenodesis that uses the anterior lateral row anchor of a double-row rotator cuff repair to simultaneously secure the biceps tenodesis and rotator cuff tear. This technique provides a simple, reproducible, cost-effective means of performing a simultaneous biceps tenodesis and double-row rotator cuff repair.
Pathology of the long head of the biceps (LHB) tendon is frequently observed in the setting of rotator cuff tears.1,2 When a significant tear or instability of the LHB tendon is identified during a planned rotator cuff repair, a biceps tenotomy or tenodesis is typically performed. Although there is no consensus regarding choosing tenodesis or tenotomy, proponents of tenodesis describe several theoretic advantages, such as maintained cosmetic appearance; closer reproduction of normal anatomy; avoidance of atrophy, cramping, and fatigue; and an improved ability for return to physical activity.3-5
There are a variety of described methods for performing biceps tenodesis using open and arthroscopic techniques. The LHB tendon is typically released from the origin and secured anywhere along the biceps groove from the glenohumeral joint to the pectoralis major tendon. Methods for securing the tendon have included keyhole and bone tunnel techniques, use of suture anchors, and use of interference screws.6-9
Performing a biceps tenodesis in the same setting as a rotator cuff repair has typically required the use of additional implants and surgical dissection. When double-row repairs of the rotator cuff are performed, the anterior anchor used for the lateral row is often placed in proximity to the biceps groove. The purpose of this report is to describe a novel technique for biceps tenodesis in the setting of a double-row rotator cuff repair. The technique uses suture anchor fixation provided by the anterior anchor used for the rotator cuff lateral row repair. This technique limits the arthroscopic surgical dissection, simplifies the biceps tenodesis, and lowers the overall implant cost and implant load needed to complete the procedure.
Technique
With the patient in the beach-chair position, a standard diagnostic arthroscopy is performed by use of a posterior viewing portal and an anterior portal through the rotator cuff interval. When significant LHB tendon pathology is identified, an anterolateral arthroscopic portal is established just inferior to the anterolateral acromion with the arm in 30° of external rotation. Using this portal and viewing from within the joint, the surgeon releases the posterior edge of the transverse humeral ligament, and a clamp is introduced through this anterolateral portal and placed on the biceps tendon (Fig 1). The clamp is used to create a mark on the biceps tendon that identifies the resection level needed to later tension the biceps appropriately. The biceps is then released by use of a basket punch from the anterior portal (Fig 2), and the tendon is delivered out of the anterolateral portal by pulling on the clamp (Fig 3). The elbow and shoulder are both flexed to take tension off the biceps and allow for the entire tendon to be advanced out of the anterolateral portal. As seen in Video 1, an additional clamp placed around the biceps tendon is used to help retract the skin and expose more of the tendon by pushing the clamp into the shoulder. A No. 2 FiberWire suture (Arthrex, Naples, FL) is then used to place a locking Krackow stitch through the tendon just under the level previously marked by the clamp, and the intra-articular segment is excised (Fig 4). The tendon is allowed to retract back into the shoulder, with the 2 suture limbs parked in the anterolateral portal.
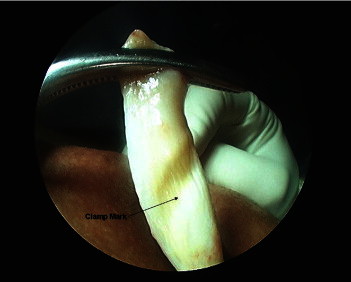
Figure 1.

Arthroscopic image of right shoulder (beach-chair position) from posterior viewing portal within glenohumeral joint. The arm is placed in approximately 30° of external rotation, which aligns the anterolateral portal with the biceps groove. The diseased LHB tendon is grasped by a clamp originating from the anterolateral portal. By use of the same clamp, a mark can be made on the biceps tendon as it enters the joint. This mark will later serve as a reference to the amount of biceps needed to be resected to establish anatomic tension of the tenodesis.
Figure 2.

Arthroscopic image of right shoulder (beach-chair position) from posterior viewing portal within glenohumeral joint. A thin basket punch is advanced from an anterior rotator cuff interval portal. The diseased LHB tendon is released from the supraglenoid tubercle. The clamp remains attached to the biceps tendon to prevent immediate retraction out of the joint.
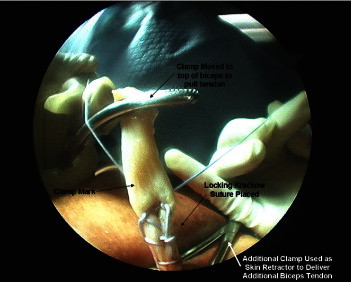
Figure 3.
With the elbow and shoulder both in maximal flexion, the LHB tendon is pulled out of the anterolateral portal. To retract the skin down, the back half of an additional clamp is placed around the biceps. The clamp on the biceps tendon is placed under tension, and the clamp on the skin is pressed downward. This helps to deliver the entire tendon out of the anterolateral portal. The clamp mark can be seen, identifying the level of the upper biceps groove.
Figure 4.
A locked Krackow suture is passed through the LHB tendon, and the intra-articular segment of the LHB tendon is resected. The appropriate resection level is determined by the mark previously made with the clamp, and the sutures are placed just below this level. The segment above the sutures can then be excised.
Attention is next directed to the rotator cuff repair. The camera is repositioned into the subacromial space through a posterior viewing portal. The rotator cuff is mobilized in preparation for a double-row transosseous-equivalent repair, and the greater tuberosity is lightly debrided to create a healing surface. Medial row anchors are placed, and the sutures are passed through the rotator cuff and tied. One suture from each anchor is then combined with the 2 suture limbs from the biceps tendon (Fig 5) and placed into a 5.5-mm polyether ether ketone (PEEK) self-punching SwiveLock anchor (Arthrex). The anchor is introduced into the proximal humerus just posterior to the biceps groove. The rotator cuff sutures are individually tightened, followed by the 2 biceps sutures. The anchor is then advanced, and the ends of the sutures are cut (Fig 6). This allows for the LHB tendon to advance up to the fluted anchor for secure fixation of the biceps tenodesis. The remaining medial row rotator cuff sutures are placed into a posterior lateral row anchor and tensioned, completing a secure transosseous-equivalent suture bridge repair (Figs 7 and 8).
Figure 5.
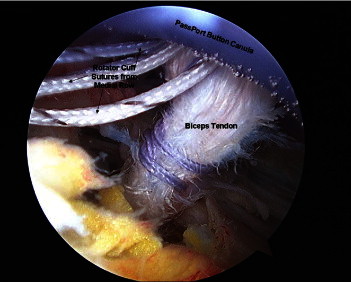
Arthroscopic image from posterior viewing portal in subacromial space (beach-chair position). Sutures from each medial row anchor are combined with the 2 suture limbs from the biceps. These sutures are being placed into a 5.5-mm self-punching PEEK SwiveLock anchor.
Figure 6.
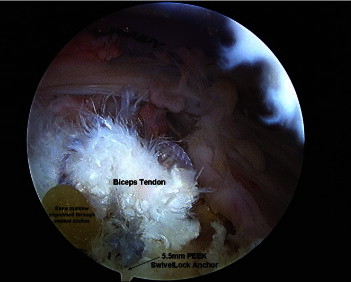
Arthroscopic image from posterior viewing portal in subacromial space (beach-chair position). The anchor is placed just posterior to the biceps groove, resulting in a lateral row repair of the rotator cuff and a secure biceps tenodesis. The fluted anchor allows yellow-appearing bone marrow from the greater tuberosity to be expressed.
Figure 7.
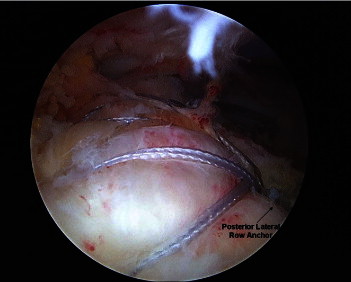
Arthroscopic image from posterior viewing portal in subacromial space (beach-chair position). The posterior lateral row anchor has been placed, resulting in a secure double-row transosseous-equivalent suture bridge repair.
Figure 8.

Arthroscopic image from lateral viewing portal in subacromial space (beach-chair position). The biceps tenodesis is easily visualized with a maintained trajectory of the biceps in line with the biceps groove.
Discussion
The described technique provides a simplified method for arthroscopic biceps tenodesis when performing a double-row rotator cuff repair. Biceps tenodesis is frequently performed together with a rotator cuff repair, because concomitant pathology of the LHB tendon is often seen.1,2 In a recent meta-analysis, Hsu et al.3 observed that 77% of patients treated with biceps tenodesis underwent simultaneous rotator cuff repair. Simultaneous repairs of the rotator cuff and biceps tenodesis can often be technically difficult and typically require additional surgical dissection and additional implants. In cases of challenging rotator cuff repairs, fluid extravasation can make visualization difficult when one is attempting to perform a separate arthroscopic biceps tenodesis.
Various methods for biceps tenodesis have been described,10 with the most common techniques using either suture anchors or interference screw fixation. The strength of suture anchor fixation for biceps tenodesis has been shown in mechanical studies to be equivalent to interference screw fixation7 and has become a commonly used method of fixation for biceps tenodesis with better clinical results than soft-tissue tenodesis techniques.11
Although numerous reports have described techniques, mechanical testing, and surgical outcomes of isolated biceps tenodesis, there are few described methods of simultaneous biceps tenodesis and rotator cuff repair.12-14 Koh et al.13 described a technique that uses a separate suture anchor dedicated for the biceps tendon. In contrast, George14 described a method using a single suture anchor to secure the biceps tendon to the torn edge of the supraspinatus tendon. The technique relies on arthroscopic passage of a simple stitch through both the supraspinatus and LHB tendon and can be limited by the quality of the diseased LHB tendon. Because the biceps tendon is often frayed along the region where these sutures must be passed, the authors warn that the technique should not be performed if the biceps tendon is too frayed.14
By use of the currently described technique, the diseased intra-articular LHB tendon is excised and a locking Krackow stitch is placed. The LHB tendon is then secured to the proximal humerus with a 5.5-mm PEEK threaded SwiveLock anchor (Arthrex), which also secures the lateral row of the rotator cuff repair. This is the first technique to describe use of a suture anchor for the dual purpose of biceps tenodesis and lateral row fixation of the rotator cuff. This is a simple, time-efficient, cost-effective method of arthroscopic biceps tenodesis that does not require excessive surgical dissection or additional implants. The technique can properly estimate appropriate tension by first marking the tendon with a clamp near the level of the ultimate tenodesis. The main disadvantage of the technique is the security of the tenodesis, because a single anchor is being used to secure both the biceps tendon and the lateral row of the rotator cuff. Thus one may wish to protect the biceps along with the rotator cuff during the initial healing process.
Footnotes
The author reports that he has no conflicts of interest in the authorship and publication of this article.
Supplementary data
Described technique. A massive rotator cuff tear is observed together with a torn biceps tendon. Two medial row 5.5-mm Arthrex Metal Corkscrew FT II anchors are used for the medial row, and two 5.5-mm Arthrex Self-Punching SwiveLock anchors are used for the lateral row repair. An Arthrex PassPort Button Cannula is used in the lateral portal.
References
- 1.Chen C.H., Hsu K.Y., Chen W.J., Shih C.H. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears. J Trauma. 2005;58:1189–1193. doi: 10.1097/01.ta.0000170052.84544.34. [DOI] [PubMed] [Google Scholar]
- 2.Murthi A.M., Vosburgh C.L., Neviaser T.J. The incidence of pathologic changes of the long head of the biceps tendon. J Shoulder Elbow Surg. 2000;9:382–385. doi: 10.1067/mse.2000.108386. [DOI] [PubMed] [Google Scholar]
- 3.Hsu A.R., Ghodadra N.S., Provencher M.T., Lewis P.B., Bach B.R. Biceps tenotomy versus tenodesis: A review of clinical outcomes and biomechanical results. J Shoulder Elbow Surg. 2011;20:326–332. doi: 10.1016/j.jse.2010.08.019. [DOI] [PubMed] [Google Scholar]
- 4.Berlemann U., Bayley I. Tenodesis of the long head of biceps brachii in the painful shoulder: Improving results in the long term. J Shoulder Elbow Surg. 1995;4:429–435. doi: 10.1016/s1058-2746(05)80034-5. [DOI] [PubMed] [Google Scholar]
- 5.Boileau P., Krishnan S.G., Coste J.S., Walch G. Arthroscopic biceps tenodesis: A new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18:1002–1012. doi: 10.1053/jars.2002.36488. [DOI] [PubMed] [Google Scholar]
- 6.Jayamoorthy T., Field J.R., Costi J.J., Martin D.K., Stanley R.M., Hearn T.C. Biceps tenodesis: A biomechanical study of fixation methods. J Shoulder Elbow Surg. 2004;13:160–164. doi: 10.1016/j.jse.2003.12.001. [DOI] [PubMed] [Google Scholar]
- 7.Mazzocca A.D., Bicos J., Santangelo S., Romeo A.A., Arciero R.A. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21:1296–1306. doi: 10.1016/j.arthro.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 8.Ozalay M., Akpinar S., Karaeminogullari O. Mechanical strength of four different biceps tenodesis techniques. Arthroscopy. 2005;21:992–998. doi: 10.1016/j.arthro.2005.05.002. [DOI] [PubMed] [Google Scholar]
- 9.Richards D.P., Burkhart S.S. A biomechanical analysis of two biceps tenodesis fixation techniques. Arthroscopy. 2005;21:861–866. doi: 10.1016/j.arthro.2005.03.020. [DOI] [PubMed] [Google Scholar]
- 10.Nho S.J., Strauss E.J., Lenart B.A. Long head of the biceps tendinopathy: Diagnosis and management. J Am Acad Orthop Surg. 2010;18:645–656. doi: 10.5435/00124635-201011000-00002. [DOI] [PubMed] [Google Scholar]
- 11.Scheibel M., Schröder R.J., Chen J., Bartsch M. Arthroscopic soft tissue tenodesis versus bony fixation anchor tenodesis of the long head of the biceps tendon. Am J Sports Med. 2011;39:1046–1052. doi: 10.1177/0363546510390777. [DOI] [PubMed] [Google Scholar]
- 12.Nho S.J., Frank R.M., Reiff S.N., Verma N.N., Romeo A.A. Arthroscopic repair of anterosuperior rotator cuff tears combined with open biceps tenodesis. Arthroscopy. 2010;26:1667–1674. doi: 10.1016/j.arthro.2010.04.008. [DOI] [PubMed] [Google Scholar]
- 13.Koh K.H., Ahn J.H., Kim S.M., Yoo J.C. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38:1584–1590. doi: 10.1177/0363546510364053. [DOI] [PubMed] [Google Scholar]
- 14.George M.S. Arthroscopic biceps tenodesis incorporated into rotator cuff repair using suture anchors. Orthopaedics. 2008;31:552–555. doi: 10.3928/01477447-20080601-10. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Described technique. A massive rotator cuff tear is observed together with a torn biceps tendon. Two medial row 5.5-mm Arthrex Metal Corkscrew FT II anchors are used for the medial row, and two 5.5-mm Arthrex Self-Punching SwiveLock anchors are used for the lateral row repair. An Arthrex PassPort Button Cannula is used in the lateral portal.