

Abstract
The present report is a rare case of Balo Concentric Sclerosis. Most cases have either been diagnosed post mortem or have succumbed to the disease after being diagnosed ante mortem. In our case, the patient showed a dramatic response to treatment, and after a one-year follow-up, he was asymptomatic, with no relapses or residual effect of the illness.
Keywords: Balo concentric sclerosis, demyelinating disorders, magnetic resonance imaging, multiple sclerosis
INTRODUCTION
Demyelinating disorders like multiple sclerosis (MS) is a common cause of neurological morbidity and mortality among the general population. Rare variants of MS like Balo Concentric Sclerosis (BCS) are classically considered to have a rapid progression, poor outcome, and poor response to treatment. However, newer evidences and clinical experiences now challenge this traditional view.[1] Newer diagnostic modalities like magnetic resonance spectroscopy (MRS) have helped in early ante-mortem diagnosis and have also shed light on the pathogenesis of the disorder, which has until now remained largely obscure.
CASE REPORT
A 26-year-old male reported in August 2009, with complaints of acute-onset of loss of speech, deviation of face toward the right, nasal regurgitation of fluids, and altered behavior in the form of irrelevant and persistent smiling or crying, for the last 13 days. A day before, he had a few episodes of vomiting. There was no history of fever, headache, blurring of vision, diplopia, tinnitus, vertigo, seizures, unconsciousness, weakness of limbs, or bladder bowel involvement. There was no previous history of preceding infection or vaccination few days or weeks prior to the onset of neurological symptoms.
During the examination, the patient was conscious, oriented with stable vitals, but aphasic (transient, motor), and left upper motor neuron type facial nerve palsy with ninth and tenth cranial nerve paralysis, in the form of an absent Gag reflex. It was due to the acute demyelinating phase of the disease and was consistent.
Neck rigidity and Kernig's sign were absent; bilateral fundii, pupillary reflex, visual acuity, and color vision were normal with no ophthalmoparesis. The eighth, eleventh, and twelfth cranial nerves were also normal. The sensory and motor system and deep tendon reflexes were normal, the plantars were bilaterally downgoing, the Romberg sign was negative, and coordination was normal. There was no history of diabetes, hypertension, palpitation, breathlessness, photosensitivity, or joint pains in in past. No relevant family history was present.
Blood biochemistry revealed normal blood count, and normal renal and liver function. Human immunodeficiency virus (HIV), anti-nuclear antibody, anti-dsDNA, rheumatoid factor, and anti-phospholipid antibody were negative. Differential diagnosis included confluent acute demyelinating encephalomyelitis (ADEM) and confluent lesions of MS.
Cerebrospinal Fluid (CSF) analysis showed a total white blood cell (WBC) count of 06 cells (all lymphocytes), sugar 36 mg%, protein 97.5 mg%, and adenosine deaminase 7.2 IU. It was negative for oligoclonal bands or IgG. T2-weighted MRI sequences [Figure 1] and fluid-attenuated inversion recovery (FLAIR) sequence images showed bilateral asymmetric hyperintense confluent lesions in the periventricular and centrum semiovale location, suggestive of a demyelinating pathology [Figure 2]. Axial T2WI and gadolinium-enhanced scans showed characteristic concentric and laminated lesions [Figures. 3 and 4]. The lesions did not show any enhancement [Figure 3]. Magnetic resonance spectroscopy obtained as a single voxel image at 135 ms, at the time of presentation, showed a non-specific choline peak, suggestive of a demyelinating pathology [Figure 5].
Figure 1.
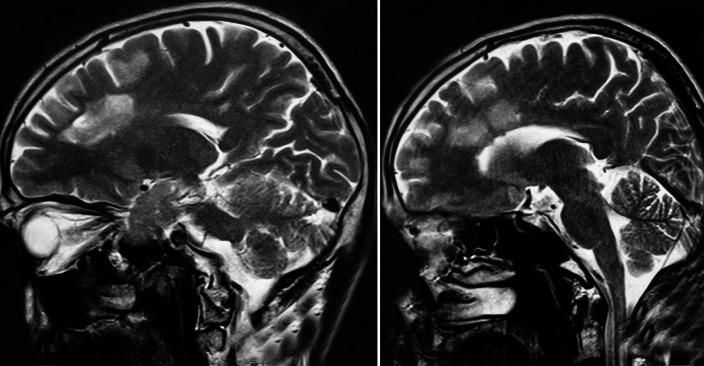
Sagittal T2WI showing confluent hyperintense lesions in the periventricular location
Figure 2.
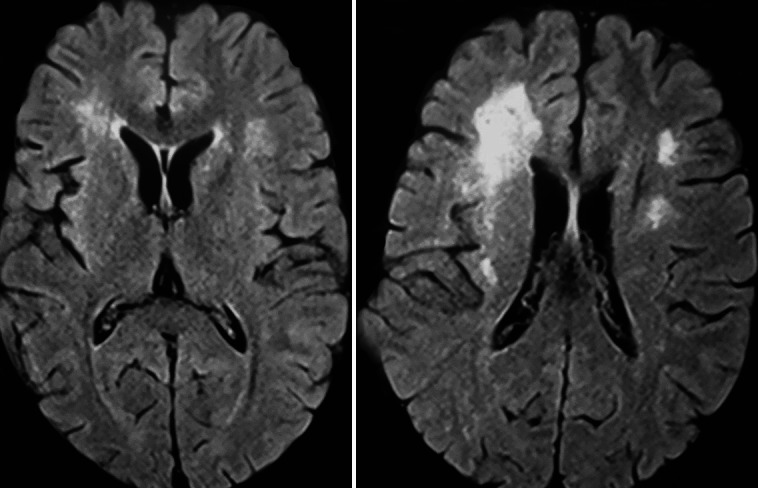
Axial fluid-attenuated inversion recovery image showing hyperintense white matter lesions in the periventricular lesions
Figure 3.
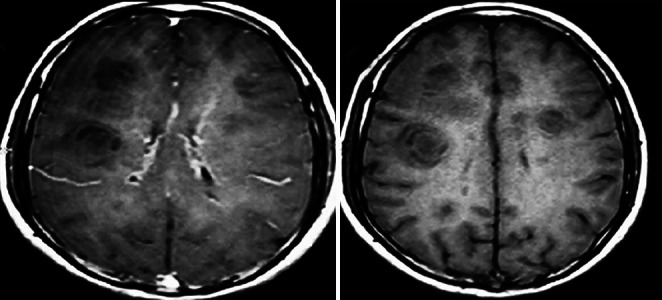
Contrast-enhanced Gadolinium scan showing no enhancement. The concentric laminated pattern of the lesions can be seen
Figure 4.
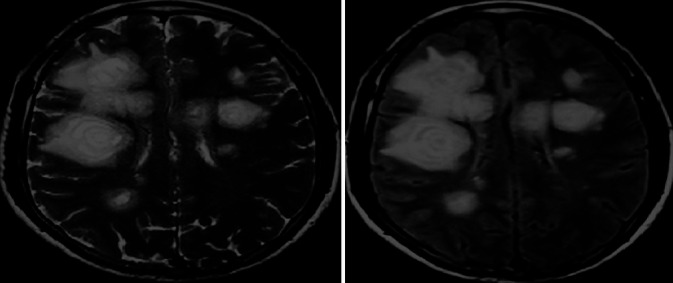
Axial T2WI and fluid-attenuated inversion recovery showing concentric laminated hyperintense lesions characteristic of concentric sclerosis
Figure 5.
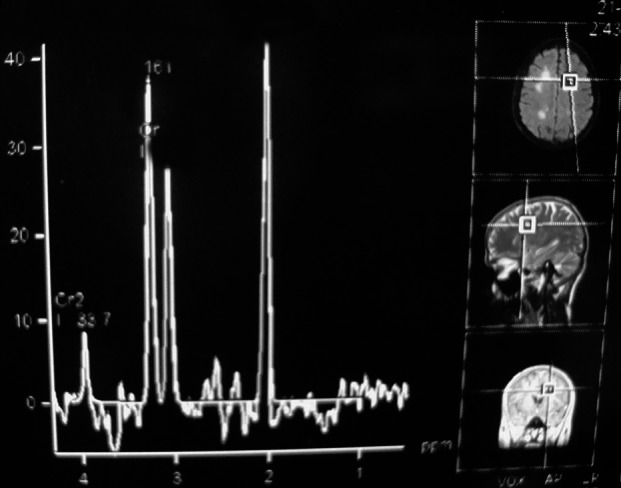
Magnetic resonance spectroscopy single voxel at 135 ms showing a non-specific choline peak
The patient was put on oral prednisolone based on clinical suspicion of an acute demyelinating pathology. The decision to continue with this was based on the dramatic response and clinical improvement of the patient. We started oral prednisolone 1 mg/kg for four weeks, and then tapered it over six weeks. The patient's speech, swallowing, and facial deviation returned to almost normal during the eight days of hospital stay. The patient was normal at the three-, six-, and twelve-month follow-up, with no relapse. Magnetic resonance imaging after 12 months showed reduction in size of the demyelinating plaques. On follow-up scans there was no evidence of dissemination of the disease in time or space. There were no new enhancing lesions, and no TI black holes were noted.
DISCUSSION
Balo concentric sclerosis is considered a rare acute demyelinating disease of the central nervous system, of unknown etiology. The pathophysiology and existence of this entity is controversial. Some consider it as a discrete disorder and some consider it to be a variant of MS. It is more common in young males, presenting as focal neurological deficits like, hemiplegia, hemianesthesia, or coordination defects. Involvement of the cerebellum, spinal cord, and optic chiasm has also been reported.[1,2] Cortical signs like aphasia and mental disturbances are rare.[1] The alternating lamellae of demyelination and normal myelination with perivascular lymphocytic infiltrates and absence of intrathecal IgG synthesis suggests that it is a different disease entity from MS. Several physiochemical, anatomical, and cytotoxic theories have been proposed, to explain the genesis of these typical lesions, the latest being the theory of tissue preconditioning, by Stadelmann et al.[3] Brain biopsy is the gold standard, but with the advent of MRI, many more cases are now being diagnosed ante mortem.[4] Spectroscopy (H+) shows a choline peak due to demyelination as in MS.[1] Earlier it was considered as a disease with poor prognosis, but recent cases and our case show that in a single monophasic event, complete response to therapy and survival is possible. Other presentations are the primary, progressive, and relapsing remitting type. Steroids, plasma exchange, and immunosuppressive therapy have been tried, with variable responses.[5] The present case has shown a dramatic response to oral prednisolone and clinical improvement.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Mowry EM, Woo JH, Ances BM. Balo's concentric sclerosis presenting as a stroke like syndrome. Nat Clin Pract Neurol. 2007;3:349–54. doi: 10.1038/ncpneuro0522. [DOI] [PubMed] [Google Scholar]
- 2.Kreft KL, Mellema SJ, Hintzen RQ. Spinal cord involvement in Balo's concentric sclerosis. J Neurol Sci. 2009;279:114–7. doi: 10.1016/j.jns.2008.12.030. [DOI] [PubMed] [Google Scholar]
- 3.Stadelman C, Ludwin S, Tabira T, Guseo A, Lucchinetti CF, Leel-Ossy L, et al. Tissue preconditioning may explain concentric lesions in Balo's type of multiple sclerosis. Brain. 2005;128:979–87. doi: 10.1093/brain/awh457. [DOI] [PubMed] [Google Scholar]
- 4.Kastrup O, Stude P, Limmroth V. Balo's concentric sclerosis Evolution of active demyelination demonstrated by serial contrast-enhanced MRI. J Neurol. 2002;249:811–4. doi: 10.1007/s00415-002-0718-0. [DOI] [PubMed] [Google Scholar]
- 5.Li Y, Xie P, Fan X, Tang H. Balo's concentric sclerosis presenting with benign clinical course and Multiple sclerosis like lesion on magnetic resonance images. Neurol India. 2009;57:66–8. doi: 10.4103/0028-3886.48815. [DOI] [PubMed] [Google Scholar]