

Introduction
The lack of emergency preparedness training (EPT) for patient care providers—including clinicians, hospital workers, mental health providers, public safety and law enforcement officials, community volunteers, EMS, HAZMAT and fire personnel—poses significant risks to both patients and patient care providers. During the 1995 Tokyo sarin gas attacks, for example, up to 80% of patients bypassed first responders and reported directly to hospitals where hospital staff suffered secondary exposure to sarin due to inadequate personal protective equipment (PPE) and training.1 Furthermore, during Hurricane Katrina, the lack of EPT was cited as a significant factor contributing to adverse patient outcomes.2–7
Providing comprehensive EPT for medical trainees—including medical, nursing students and other health care trainees—is important to the future success of emergency preparedness operations in the US.8–15 Just weeks prior to the 9/11 terrorist attacks, an American College of Emergency Physicians (ACEP) task force published recommendations for medical students to develop skill-based EPT competencies for nuclear, biological, and chemical incidents.16 Immediately after 9/11, a report by the Association of American Medical Colleges (AAMC)—and later by the Institute of Medicine (IOM)—encouraged early introduction of bioterrorism topics in medical schools.17–18 Unfortunately, US medical schools have been slow to develop stand-alone EPT curricula.17, 19 Few medical schools have defined and implemented EPT core competencies for health professionals19–20 and newly developed EPT programs have largely focused on practicing clinicians and not trainees.21–24
Disasters are rare, complex events involving many patients and environmental factors that are difficult to reproduce inside a classroom. Recent reviews suggest that health care worker EPT programs lack clarity, objectivity, competency-driven goals, scientific rigor, prospective validation, and consistency across medical specialties.25–28
In a prior study, we revealed how medical students can value and rapidly learn some core EPT elements via a novel addition to a medical school’s curriculum.19, 29 Students who completed our 3-hour ‘Disaster 101’ curriculum vastly increased their overall knowledge and comfort level with EPT skills. A significant limitation of our study was the relatively simplistic measurement of EPT performance. In one scenario, students were required to rapidly triage 100 life-sized inflatable mannequins tagged with physical parameters indicating respiratory, circulatory, and mental status. It was suggested from the curriculum review that the validity and reliability of the EPT performance measurement would be better suited in a controlled environment, such as the university human patient simulation laboratory, in which a combination of live actors and human simulated patients could reproduce the ‘chaos’ associated with a clinical disaster. It was further suggested that high fidelity patient simulators could help us evaluate the impact of our EPT on patient outcomes, for example, whether trainees could appropriately triage and intervene medically to save a life.
Here we described the development of a human simulation-based EPT curriculum for patient care providers that recreates a chaotic clinical disaster through a combination of up to 15 live actors and 6 high-fidelity human simulators. Specifically, we detail the Center for Health Professional Training and Emergency Response’s (CHPTER’s) one-day clinical EPT course—provided first to medical students, then to a group of experience disaster medical providers—including its organization, core competency and content development, medical student self evaluation and course assessment. To our knowledge, this is the first published description of a curriculum method that combines high-fidelity, multi-actor scenarios to measure the life-saving performance of patient care providers during a moderately-sized clinical disaster (> 10 patients at once).
Curriculum Development—Organization
In 2009, CHPTER was formed as South Carolina’s first collaborative EPT center for health professionals (www.musc.edu/chpter). A community-wide advisory committee of emergency preparedness stakeholders—including regional hospitals, NGO’s, public health officials, EMS and law enforcement agencies—met to establish goals for CHPTER to enhance regional health security. CHPTER’s established a mission to enhance regional health security and surge capability by giving patient care providers hands-on lessons that will protect and save patient lives during a disaster.
A curriculum task force of the CHPTER Advisory Committee consisting of health professional and emergency preparedness experts met and decided: 1) the EPT course should be no greater than 1 day to ensure increased attendance from busy trainees and other patient care providers, 2) the curriculum should be directed toward the general medical trainee, defined broadly as any patient care provider during a disaster, so it could develop into an interdisciplinary experience 3) the curriculum should be interactive and case-based so trainees could recognize the relevance of disaster medicine knowledge and clinical skills to their work place; 4) human simulation and multi-patient encounters should be used to create realistic clinical disasters; and 5) research metrics should be developed to measure trainee skill acquisition and performance to save lives during a disaster. The task force hypothesized that the newly proposed EPT course would improve patient care provider knowledge, skills, and comfort level necessary to save lives during a disaster. The task force evaluated existing competency objectives and domains from a course given to 4th year university medical students in 2008 and 2009.19, 29 Additional competency and evaluative frameworks considered included those from the Veteran’s Health Administration (VHA), the American Medical Association’s Center for Public Health Preparedness and Disaster Response, the Agency for Health Care Research and Quality (AHRQ), Columbia University and others.30–35
Curriculum Development
Over the course of several months, the task force worked to establish learning objectives for CHPTER trainees (Table 1a). Of the nine learning objectives, we categorized six as ‘discrete knowledge/cognitive,’ three as ‘performance/skill’ and two as ‘attitudinal/affective,’ according to Bloom’s Taxonomy.36–38 Through a modified Delphi process, the task force developed competencies for the course. Dozens of competencies were consolidated into 18, and subsequently assigned to five competency domains: Mobilization, Operations/Communications, Human Safety and Facility Continuity, Demobilization, and Awareness (Table 1b). The task force then developed performance measures to match competency/learning objectives and utilized these to guide content development for the didactic, small group and simulation components of the course. A course itinerary was developed to accommodate the 1-day schedule limit (Table 2).
TABLE 1A.
COURSE LEARNING OBJECTIVES
| A. Define a healthcare disaster and the components of emergency preparedness as it applies to patient providers.1 |
| B. Understand ethical implications of a healthcare disaster and its impact on the community.3 |
| C. Differentiate between NIMS, ICS/HICS and the operational disaster/emergency preparedness plan for a healthcare facility.1 |
| D. Identify functional roles (and appreciate your individual limits) of patient care providers during a disaster.1,3 |
| E. Define and demonstrate ability to function within the chain of command during a patient care disaster scene.1,2 |
| F. Define and respond to vulnerabilities and security risks facing providers, healthcare workers and healthcare facilities during a disaster scenario.1,2 |
| G. Summarize components of teamwork, communication and triage that are essential to an effective response during a healthcare disaster and list specific actions to take and those to avoid during a healthcare disaster.1 |
| H. Demonstrate effective teamwork, communication and triage to protect patient care providers and save the lives during a disaster scenario.2 |
| I. Achieve a great comfort level with knowledge and skill to provide effective patient care during a clinical disaster3 |
Discrete Knowledge/Cognitive Objective
Performance/Skill Objective
Attitudinal/Affective Objective
TABLE 1B.
COURSE COMPETENCY DOMAIN AND PERFORMANCE OBJECTIVE CATEGORIES
| ● Mobilization: Pre-stage Planning and Team Development |
|
| ● Clinical Disaster Operations and Communications |
|
| ● Protect and Preserve Human Life and Continuity of Health Care Facility During a Disaster |
|
| ● Demobilization |
|
| ● Clinical Disaster and Emergency Preparedness Awareness |
|
TABLE 2.
CHPTER COURSE SCHEDULE
| Hour | Event |
|---|---|
| 7:45–8 AM | Pretest and Consent |
| Welcome | |
| Online material (prior to arrival) | |
| Pretest and Self Evaluation | |
| Online learning material | |
|
| |
| On Arrival | Pretest (if not already complete) |
| Consent forms | |
| Sign in sheet | |
|
| |
| 8–8:55 AM | Module 1: The Center for Health Professional Training and Emergency Response, CHPTER (50 minutes) |
| |
|
| |
| 9–9:45 AM | Module 2: Mobilization: Pre-stage Planning and Clinical Teamwork (25 minute slides, 20 minute Small Group) |
| |
|
| |
| 15 min Break/Time Buffer | |
|
| |
| 10–10:45 AM | Module 3: Clinical Disaster Scene Operations and Communications (25 min slides, 20 min Small Group) |
| |
|
| |
| 15 min Break/Time Buffer | |
|
| |
| 11–11:45 AM | Module 4: Protect and Preserve Human Life (25 minutes slides, 20 minutes Small Group) |
| |
|
| |
| 12–1 PM Lunch | |
|
| |
| 1–4 PM | Multi-actor Simulated Disaster |
| CHPTER’s scenario “Influenza-Like Illness” | |
| Education Intervention: Debriefing | |
| Repeat Scenario | |
|
| |
| 4–5 PM | Post Test and Course Assessment |
|
| |
| After Completion of Mass Casualty Scenario | |
|
|
|
| |
| 4–6 months after Course | |
|
|
Small Group Exercise Scenario Development
Small group exercises developed for the Communication, Teamwork, and Triage modules and were designed to prepare students for the afternoon simulation exercise and included interactive training experiences that were administered by trained CHPTER facilitators and core faculty. During the ‘teamwork’ small group exercise, teams of 4–5 trainees were confronted with an image about a disaster scene disguised as a 34 piece puzzle inside an envelope. Four envelopes containing a unique fictional disaster scenario (Scenario 1, Dirty Bomb; Scenario 2, Concert Blast; Scenario 3, Earthquake; and Scenario 4, Flu-Like Illness) were presented to trainees in series. Teams were instructed that they were to complete at least one puzzle using skills their learned during the didactic session. Facilitators timed rated team performance and recorded team feedback about the exercise.
The ‘communications’ small group exercise consisted three scenarios (Scenario 1, Bus Crash; Scenario 2, Factory Explosion; and Scenario 3, Chemical Leak) presented to team members on pre printed handouts. Scenarios were discussed in small group with the help of the facilitator who measured the extent to which the group could effectively communicate clinical disaster information. During the ‘triage’ small group exercise, teams were asked to sort hundreds of small toys with preprinted medical information printed on them according to the START Triage System. Instructors evaluated trainees based on their ability to work as a team to rapidly assess and accurately triage several patients at once.
Human Simulation and Actor Scenario Development
The task force addressed the Advisory Committee goal regarding the development of performance metrics for a clinical disaster scenario by partnering with the university’s Clinical Effectiveness and Patient Safety Center. The center boasts a $2M, 11,000 ft2 patient simulator facility, in-house training engineering staff, computer and software experts and a wide range of research tools including discrete viewing rooms, digital video and software simulation technologies.
Human simulators (SimMan™) in the center have the ability to demonstrate physical exam findings (i.e., pulse, breathing rate, ocular reflexes and remote-triggered verbal statements) and to respond to caregiver procedures (i.e., jaw thrust, bag valve mask, tourniquets, blood pressure measurement, chest tubes and IV/IO medicines). The staff has the ability to program individual patient mannequins to follow variable physiologic “curves” and to observe trainee performance via 1-way observation rooms. (See Figure 1) Some mannequins may be pre-programmed to enter ventricular fibrillation or cardiopulmonary arrest if the airway is not opened and secured in a timely fashion. Other mannequins can be programmed to follow more normal physiologic curves with normal vital signs but have stark physical exam findings (i.e., an open shoulder fracture).
Figure 1.
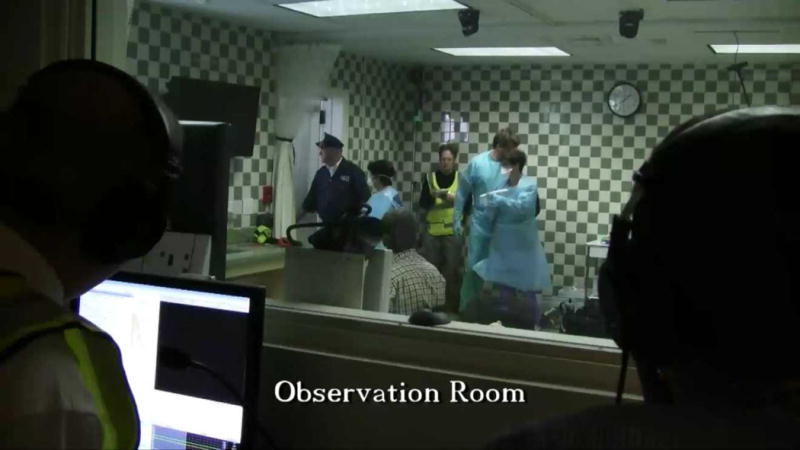
EPT facilitators observing trainees during EPT multi-actor disaster scenario.
Over 6-months, CHPTER worked with center engineers to develop a series of fictional clinical disasters that combined up to six patient simulators and up to 15 trained “actors” to simulate a moderately-sized clinical disaster. We designed one of the center’s larger observation rooms to look like a small emergency waiting room with several chairs, a security guard’s desk, a metal detector and communication devices. There was also a door to the outside of the simulation center that was used to simulate an ED entrance. Not unlike the development of a short film, storyboards and a stage map were developed for the simulated exercise (Figure 2).
Figure 2.
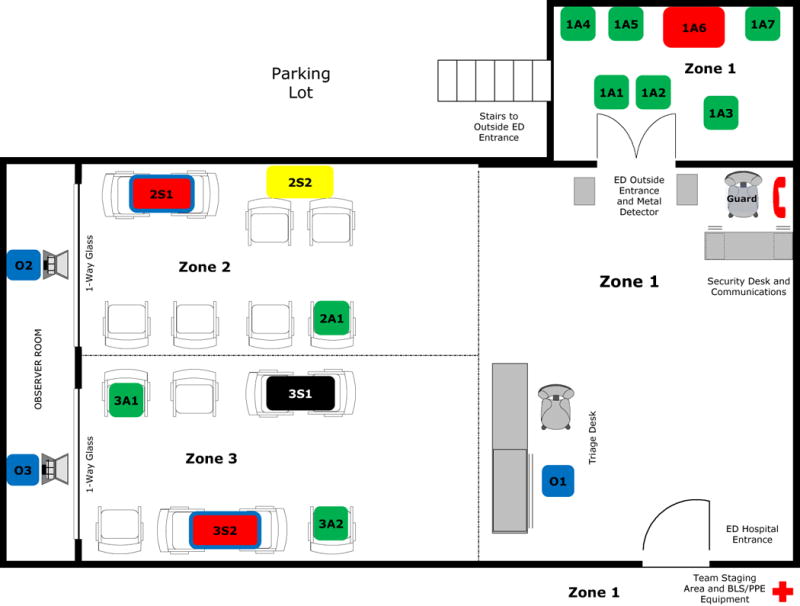
High fidelity simulator and actor staging in simulation lab. Blue: Observer Trainer; Green: Triage Green; Yellow: Triage Yellow; Red: Triage Red; Black: Triage Black; A = Actor; S = High Fidelity Human Simulator; 1 = Zone 1; 2 = Zone 2; 3 = Zone 3. Example: 2S1 (Red) is a High Fidelity Human Simulator Patient who is Triage Red in Zone 2.
CHPTER facilitators and core faculty were trained by the simulation center to operate simulation center equipment and software. Facilitators were assigned to different geographical zones (#1–3) of the scene so that they could more easily focus on performance objectives during the chaotic movement of patients and actors during the scenario.
Two month prior to training, we gathered up to 15 actors—including trained patient actors from the medical university—and provided them pre-scripted roles. To enhance reliability and validity of the expected performance objectives from trainees, actors were taught how to follow specific behaviors when confronted with trainees in a chaotic environment. For example, one actor (patient 3A2) was asked to complain very loudly about his symptoms. If he was not counseled by a trainee, or redirected, he would create a disturbance and interfere with the care of some of the mannequins. If he received any counseling from a trainee, he would simply sit down or follow directions.
Multi-actor Clinical Disaster Scenario: “Influenza-Like Illness”
The clinical casualty scenario developed by the curriculum task force involved the acute presentation of cruise line tourists complaining of cough and shortness of breath. During the six minute scenario (‘Influenza-Like Illness”) both actors and simulators experience various levels of respiratory complaints, several of them waiting to access the ED waiting room. Working in teams of 4 to 6, trainees were required to mitigate the complex scene using skills they learned during didactic and small group lessons. The responders were not aware that some of patients were suffering from inhalation anthrax. They are also unaware that one of the patients waiting to access the emergency department was carrying two bags of powder, presumed to be anthrax.
Of the four human simulators used in this scenario, two were unstable and required active airway maneuvers (i.e., a simple jaw thrust) in order to open their airway. If teams recognized the acuity of the patients and acted prior to four minutes, the simulator’s physiologic curve normalized. If not, CHPTER facilitators allowed the physiologic curve of the simulators to deteriorate irreversibly to cardiac arrest.
Trainees were also confronted with several actors demanding care. The actors were trained to escalate their behavior during the scenario, unless appropriate performance measures were met. Once escorted to the Green Triage waiting area, minor patients changed costumes and presented to the ED entrance as new patients. One actor (the terrorist disguised as a tourist) utilizes a distraction caused by other actors to bypass security and enter the ED waiting room. If teams close the ED door prior to 4 minutes, the terrorist threat is averted. If they do not do this, the actor enters the ED and holds up two bags of powder, exposing all patients and all providers to a simulated lethal dose.
An educational intervention was developed for all teams participating in the mass casualty scenario. Immediately after teams completed their first 6 minute scenario, trainees were escorted to a debriefing room. Using a digital split screen, teams were presented with a playback of their performance using up to 4 different camera viewpoints. CHPTER instructors were trained to reinforce key components of the learning objectives and competencies for the course without providing specifics to remedy the disaster scene. Per study design, teams were permitted to repeat the 6 minute scenario after the debriefing. Team membership and scenario content did not change.
Planning, Logistics and Recruitment
Running concurrent with the curriculum development process was multiple planning operations. Over a two-year period, CHPTER Advisory Committee members worked to brief and receive input from hospital and emergency preparedness leaders about their EPT training needs. Dozens of meetings were required with University officials, including those from the Office of the President, the Board of Trustees, the Office of the Dean, Medical University Hospital Disaster Preparedness Committee, Public Relations, and Public Safety. A statewide survey of hospital Emergency Medicine Directors was completed to further refine our EPT goals, objectives and content.39
The Advisory Committee set a goal to recruit medical students to complete the first demonstration of the EPT curriculum. Working with the College of Medicine, ten 4th year medical students volunteered and were enrolled. A second cohort of 17 practicing clinicians from the Veteran’s Health Administration (VHA) were recruited and voluntarily enrolled in the course. The group represented a VHA committee from the Emergency Management Strategic Health Care Group (EM SHG) and consisted of physicians, nurses and emergency managers from across the US and Puerto Rico. All participants signed a “Consent and Waiver” prior the course. The project was approved by the University Institutional Review Board (IRB).
Research Metrics
The task force developed an online pre-test and two post-tests for trainees utilizing a pool of questions developed to meet the learning objectives and competencies of the course. The pre-test consisted of two parts. In the first part, Likert-scale self-assessment questions measure trainees’ sense of personal capability and comfort level to handle a disaster. The second part included 23 discrete multiple choice questions.
The post-test consisted of three parts. The first part was identical to the first part of the pre-test (Likert-scale self assessment questions). The second part of the post-test contained 23 discrete multiple choice questions. In order to ensure that students were not answering by memory, some answer orders and questions stems were modified. For example, one post-test question described the same patient triage scenario in the pre-test but assigned different vital signs to the patient so the triage answer was “Red” instead of “Yellow”. The third part of the post-test consisted of Likert-scale and open-ended questions for trainees to evaluate course content and instructors. Trainees were asked to complete the same post-test 4–6 months following the training.
Patient outcomes during the mass casualty scenario were central to our experimental focus and were measured primarily using performance criteria “checked off” by CHPTER researchers observing trainees in the human performance lab. The end product was a single list of “met” performance objectives for each team performance. Observers had the opportunity to complete any part of the checklist they did not have time to finish with the help of the digital playback. Once a single list was complete, we simply recorded the percentage of “met” performance objectives from each group. Any data missing from an evaluation checklist was considered an “unmet” performance objective.
Descriptive statistics such as means, standard deviations, medians, etc, were used to describe elements of the EPT training, as appropriate. Wilcoxon rank sum tests were used to compare the pre- and post-test values within the cohorts of COM students and VHA trainees. Because many of the pre- and post-tests were completed by the same individuals, and because the test was completed anonymously (thus making it impossible to conduct paired testing), the p-values obtained from the Wilcoxon rank sum tests are conservative estimates. In other words, if we had been able to link subject’s pre- and post-test scores and perform a paired analysis, the resulting p-values would have been smaller than what was observed in the independent testing done by the Wilcoxon rank sum test. 40
Training Days
Prior to arriving at the training session, participants completed the pre-test and some online training modules discussing basic concepts and terminology of EPT. (The same pretest, post test, actors, facilitators, slides, small group exercises and simulated disaster scenario were utilized for all trainees.) On the day of training, students signed consent forms and were given the pre-test—via laptops available in the classroom—if they had not already completed it online. During Module 1, participants were given a presentation about CHPTER and expectations for the course (Table 2). For Module 2 trainees watched a presentation about pre-stage planning and clinical teamwork, and they also performed a small group exercise in teamwork. For Module 3, participants listened to a presentation about clinical disaster scene operations, and they engaged in a small group exercise about clinical disaster communication. In Module 4 the course trainees received a presentation on personal safety and triage and they worked to complete a table top triage exercise. All small group exercises lasted for 20 minutes in the given modules. After a one hour lunch break, participants were randomly assigned to a small group to participate in the clinical casualty scenario, “Influenza-Like Illness.” Participants were faced with deciding how to prepare for dealing with the given scenario, what PPE to use, how to triage patients presenting to the ER, and how to deal with unexpected complications that arose during the six-minute exercise. Participants worked with both standardized patients (actors) and high-fidelity simulation manikins (Figures 3–7).
Figures 3–7.





Trainees interacting with actors and human simulators during multi-actor disaster scenario.
The MCI exercise lasted approximately 3 hours. After completing the first scenario, each team received a debriefing in a private viewing room with digital playback screens. (Figure 8) The last hour of the course was dedicated to completing the post-test and a course evaluation. Trainees were notified that they would receive the follow up test, online by email, in 4–6 months.
Figure 8.

Post-scenario debriefing with trainees using recorded digital feeds of student performance.
Student Assessment
Ten medical students received approximately 9 hours of training at the university simulation center and 17 physicians, nurses, and emergency managers from the Department of Veterans Affairs Emergency Management Strategic Health Care Group (EMSHG) were provided the same 9-hour course. A review of the data supplied by the College of Medicine shows that the medical students significantly valued the curriculum and felt their EPT knowledge and skill increased. Most (70%) of the trainees considered their EPT knowledge and/or skill average or below average before the training experience. After the curriculum, 100% of trainees considered their EPT knowledge and/or skill above average, and 90% would recommend the course to other patient care providers (Tables 3, 4, Figure 9). The performance data of both cohorts will be presented in a follow-up publication.
TABLE 3.
PERCENT OF MEDICAL TRAINEES WHO WOULD RECOMMEND THE CHPTER EPT COURSE
| Q: “I would recommend this course to next year’s class” | ||
|---|---|---|
| No Answer | 0 | 0 |
| Strongly Disagree | 0 | 0 |
| Disagree | 0 | 0 |
| Neutral | 1 | 10% |
| Agree | 1 | 10% |
| Strongly Agree | 8 | 80% |
| Total | 10 | 100 |
Source: College of Medicine 2011 course evaluation
TABLE 4.
MEDICAL TRAINEE SELF ASSESSMENT OF EPT KNOWLEDGE OR SKILL
| Q: “My overall knowledge (or skill) of this topic before the course was…” | “My overall knowledge (or skill) of this topic after the course was…” | |||
|---|---|---|---|---|
| No Answer | 0 | 0 | 0 | 0 |
| Poor | 1 | 10% | 0 | 0 |
| Below Average | 4 | 40% | 0 | 0 |
| Average | 2 | 20% | 2 | 20% |
| Above Average | 1 | 10% | 4 | 40% |
| Outstanding | 2 | 20% | 4 | 40% |
| Total | 10 | 100% | 10 | 100% |
Source: College of Medicine 2011 course evaluation
Figure 9.
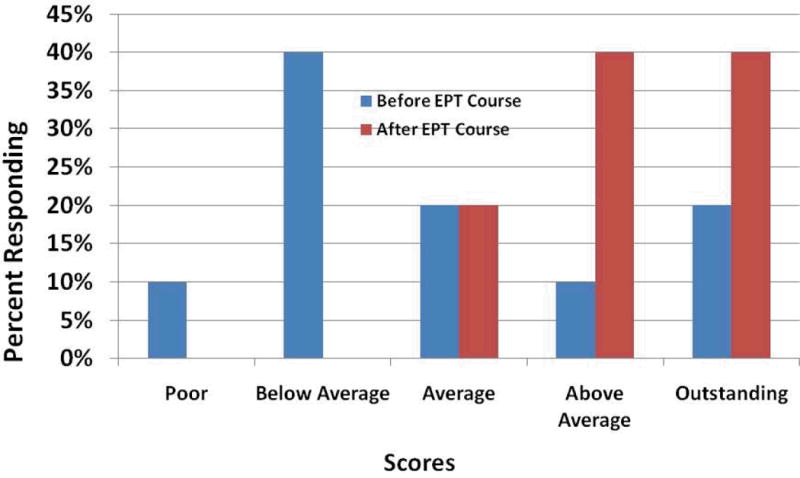
Medical trainee self assessment of EPT knowledge or skill (Source: College of Medicine 2011 course evaluation).
Discussion
Efforts to foster EPT to medical trainees in a simulated environment date back to the 1950s when researchers assessed the use of movies to augment students’ training for military and disaster events.41 The Institute of Medicine’s 1999 report, “To Err is Human,” spurred new development of the use of human patient simulators to train medical providers.42 In the 1990’s, lessons learned from the aviation industry’s Cockpit Resource Management (CRM) led a group of anesthesiologists to pioneer the Acute Crisis Resource Management (ACRM) training module that uses human patient simulators to help reduce error during emergent clinical events.43–45 Subsequent research has suggested a potential benefit of human simulators to train patient care providers for clinical emergencies.46–51 Research also suggests that simulators are warmly received by health professional students and can enhance their learning experience.52–56
Early applications of simulation to emergency medicine include its efficacy to provide emergency medicine team training,57 a pilot study of simulation to provide Emergency Medicine Crisis Resource Management (EMCRM) training58 and the theoretical use of multiple patients during simulation to replicate the chaotic environment in the Emergency Department.59 Other descriptions of simulation in emergency and military medicine are available.9, 13, 27, 57, 60–67
We performed a literature search in the PubMed database using the MeSH controlled vocabulary terms “Disasters” and “Disaster Planning”. We then searched for the keywords “training,” “education” or “simulation.” We then combined the three sets, limiting to evidence-based articles. To augment this search, we also performed a PubMed search looking for “simulation AND training AND disaster.” Additional online searches were completed to capture government reports from, for example, AHRQ (www.ahrq.gov). Our search yielded approximately 350 articles and reports.
Several evidence-based studies were found that established the efficacy of human simulation to train patient care providers for a disaster. Kyle used a combination of human actors and simulators to recreate a Weapons of Mass Destruction (WMD) exercise.68 Lerner used a combination of actors and simulators to test the accuracy of SALT triage.69 Subbarao used a combination of video and high fidelity human simulators to train teams of EMS/Fire medical providers to treat victims of chemical, biological, radiological, nuclear and explosive (CBRNE) disasters.32 Summerhill utilized a prospective cohort design to help show how human simulation increased internal medicine resident’s scores on bioterrorism written tests.70 Miller showed that health professionals (mostly EMS) would improve their confidence after using human simulators in a HAZMAT scenario.12 Vincent had medical students listen to podcasts about triage and then showed that students would improve triage accuracy after repeating scenarios with human patient simulators.63 Finally Gillett utilized paired scenarios consisting of one simulator and one actor to measure the value of simulation versus actors in EPT for physicians, residents, nurses and medical students.71
We found only one study that utilized a multi actor clinical disaster scenario to measure the life saving performance of medical trainees. Wallace quantified the disparity between the times required to resuscitate simulators and actors during a simulated disaster drill. Six simulators and six actors were presented to triage teams in waves of three patients at a time.72 Because the maximum number of patients during an individual triage encounter was limited in Wallace study, it is not clear whether the tested curricula would have an impact on trainees during a moderately sized clinical disaster (> 10 patients at once).
Here we present the methodology for the development CHPTER’s one-day clinical EPT course for patient care providers. We also present the self assessment and course evaluation data provided by the College of Medicine for students who took the course. Students who completed the course improved their overall knowledge and comfort level with EPT skills. In subsequent study, we will present comprehensive data of our medical student and practicing clinician cohorts, including their self assessment, pre and post cognitive performance, small group and MCI scenario performance and course assessment. To our knowledge, this is the first published description of a curriculum method that combines high-fidelity, multi-actor scenarios to measure the life-saving performance of patient care providers during a moderately-sized clinical disaster (> 10 patients at once).
We believe this course, and the comprehensive validation data to follow, represents the first step of the next generation of EPT for patient care providers. Our course creates a loud and chaotic clinical disaster that measures life saving performance, not just life saving knowledge. Our course is short, addressing a primary obstacle to EPT in our region and a request from providers that course be limited to one day.39 Our EPT is ‘all hazards’ and applies toward multiple disaster environments. Finally, our EPT includes First Receivers (i.e., clinicians, hospital workers, mental health providers, public safety officials and community volunteers) who may receive and care for patients during a disaster, but will not necessarily participate on the disaster scene. This addresses a critique of some widely available EPT programs that tend to focus on First Responders (EMS, Hazmat and Fire personnel) who mitigate a disaster scene.73 Because 60–85% of patients will circumvent First Responders during a large scale disaster,1, 74–79 we strongly support the broadening of traditional EPT programs in the US to recognize the unique training needs of First Receivers.
Limitations
We set out to develop a realistic multi-actor disaster scenario that includes research metrics to measure EPT performance. In some respects, the more real our disaster EPT scenarios became, the harder it was to control the testing environment, reducing the accuracy of our measurements. We sought to enhance reliability in this study with the use of technology that enabled us to 1) repeat the same educational intervention (i.e., small group exercise and simulated disaster) over and over without significant deviation of training events 2) multiple training facilitators assigned in a “zone” format to ensure that trainee actions were not missed 3) laptop computers linked to high fidelity mannequins that permitted time-stamped recordings of trainee-patient interventions and 4) a total of 4 digital video feeds that permitted both facilitators and trainees opportunity to review scenario performance. With the help of 1-way glass and headphones, facilitators were able to communicate in relative isolation to mitigate loud noise and other distractions. While still possible that observers missed performance objectives, we feel this potential was minimized.
It is important to note that when we estimate trainee performance in this study, team performance is used as a proxy for individual performance. We could have reorganized the study to measure individual trainee actions during the disaster scenario. We did not do this primarily for time constraints but also because we felt that patient care providers are more likely to work within a team during a disaster. Team performance is, therefore, a valid performance endpoint for our study.
We did not perform a cost per student assessment and recognize that in the era of declining budgets, cost performance metrics are key to ensure scalability and wide spread dissemination of training. In addition, the power assessment of this demonstration project (n = 27) is low and the external validity of this curriculum has not been established. A larger scale study, or preferably a multi-center trial with cost assessment, would allow us to further expand upon the impact, validity and scalability of our curriculum.
Conclusion
Here we present the methodology for the development of a one-day clinical EPT course for patient care providers, including its organization, core competency and content development, medical student self evaluation and course assessment. To our knowledge, this is the first published description of a curriculum method that combines high-fidelity, multi-actor scenarios to measure the life-saving performance of patient care providers during a moderately-sized clinical disaster (> 10 patients at once). A larger scale study, or preferably a multi-center trial, is needed to further study the impact of this curriculum and its potential to protect provider and patient lives. For further information regarding the curriculum, including a short video that details the patient care provider experience, please visit www.musc.edu/chpter.
Contributor Information
Lancer A. Scott, Department of Emergency Medicine, Medical University of South Carolina, Charleston, SC 29425.
P. Tim Maddux, Medical University of South Carolina, Charleston, SC 29425.
Jennifer Schnellmann, Department of Clinical Pharmacy and Outcomes Sciences, Medical University of South Carolina, Charleston, SC 29425.
Lauren Hayes, Medical University of South Carolina, Charleston, SC 29425.
Jessica Tolley, Medical University of South Carolina, Charleston, SC 29425.
Amy Wahlquist, Medical University of South Carolina, Charleston, SC 29425.
References
- 1.Tokuda Y, Kikuchi M, Takahashi O, Stein GH. Prehospital management of sarin nerve gas terrorism in urban settings: 10 years of progress after the Tokyo subway sarin attack. Resuscitation. 2006 Feb;68(2):193–202. doi: 10.1016/j.resuscitation.2005.05.023. [DOI] [PubMed] [Google Scholar]
- 2.Barkemeyer BM. Practicing neonatology in a blackout: the University Hospital NICU in the midst of Hurricane Katrina: caring for children without power or water. Pediatrics. 2006 May;117(5):S369–374. doi: 10.1542/peds.2006-0099F. Pt 3. [DOI] [PubMed] [Google Scholar]
- 3.Currier M, King DS, Wofford MR, Daniel BJ, Deshazo RA. Katrina experience: lessons learned. The American journal of medicine. 2006 Nov;119(11):986–992. doi: 10.1016/j.amjmed.2006.08.021. [DOI] [PubMed] [Google Scholar]
- 4.Edwards TD, Young RA, Lowe AF. Caring for a surge of Hurricane Katrina evacuees in primary care clinics. Annals of family medicine. 2007 Mar-Apr;5(2):170–174. doi: 10.1370/afm.646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hamm LL. Personal observations and lessons from Katrina. The American journal of the medical sciences. 2006 Nov;332(5):245–250. doi: 10.1097/00000441-200611000-00014. [DOI] [PubMed] [Google Scholar]
- 6.Kline DG. Inside and somewhat outside Charity. Journal of neurosurgery. 2007 Jan;106(1):180–188. doi: 10.3171/jns.2007.106.1.180. [DOI] [PubMed] [Google Scholar]
- 7.Leder HA, Rivera P. Six days in Charity Hospital: two doctors’ ordeal in Hurricane Katrina. Compr Ther. 2006 Spring;32(1):2–9. doi: 10.1385/comp:32:1:2. [DOI] [PubMed] [Google Scholar]
- 8.Ciraulo DL, Frykberg ER, Feliciano DV, et al. A survey assessment of the level of preparedness for domestic terrorism and mass casualty incidents among Eastern Association for the Surgery of Trauma members. J Trauma. 2004 May;56(5):1033–1039. doi: 10.1097/01.ta.0000127771.06138.7d. discussion 1039–9041. [DOI] [PubMed] [Google Scholar]
- 9.Bartley BH, Stella JB, Walsh LD. What a disaster?! Assessing utility of simulated disaster exercise and educational process for improving hospital preparedness. Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation. 2006 Jul-Aug;21(4):249–255. doi: 10.1017/s1049023x00003782. [DOI] [PubMed] [Google Scholar]
- 10.Galante JM, Jacoby RC, Anderson JT. Are surgical residents prepared for mass casualty incidents? J Surg Res. 2006 May;132(1):85–91. doi: 10.1016/j.jss.2005.07.031. [DOI] [PubMed] [Google Scholar]
- 11.Martin SD, Bush AC, Lynch JA. A national survey of terrorism preparedness training among pediatric, family practice, and emergency medicine programs. Pediatrics. 2006 Sep;118(3):e620–626. doi: 10.1542/peds.2005-1875. [DOI] [PubMed] [Google Scholar]
- 12.Miller GT, Scott JA, Issenberg SB, et al. Development, implementation and outcomes of a training program for responders to acts of terrorism. Prehosp Emerg Care. 2006 Apr-Jun;10(2):239–246. doi: 10.1080/10903120500541191. [DOI] [PubMed] [Google Scholar]
- 13.Scott JA, Miller GT, Issenberg SB, et al. Skill improvement during emergency response to terrorism training. Prehosp Emerg Care. 2006 Oct-Dec;10(4):507–514. doi: 10.1080/10903120600887072. [DOI] [PubMed] [Google Scholar]
- 14.Sklar DP, Richards M, Shah M, Roth P. Responding to disasters: academic medical centers’ responsibilities and opportunities. Acad Med. 2007 Aug;82(8):797–800. doi: 10.1097/ACM.0b013e3180d0986e. [DOI] [PubMed] [Google Scholar]
- 15.Coico R, Kachur E, Lima V, Lipper S. Guidelines for preclerkship bioterrorism curricula. Acad Med. 2004 Apr;79(4):366–375. doi: 10.1097/00001888-200404000-00019. [DOI] [PubMed] [Google Scholar]
- 16.American College of Emergency Physicians. Task Force of Health Care and Emergency Services Professional on Preparedness for Nuclear, Biological and Chemical Incidents, Executive Summary. 2001. [Google Scholar]
- 17.American Association of Medical Colleges. Report of the Expert Panel on Bioterrorism Education. 2008. Training Future Physicians About Weapons of Mass Destruction. [Google Scholar]
- 18.Institute of Medicine Committee. Hospital-based emergency care: at the breaking point Institute of Medicine Committee on the Future of Emergency Care in the US Health System. Washington, DC: National Academies Press; 2006. [Google Scholar]
- 19.Scott LA, Carson DS, Greenwell IB. Disaster 101: a novel approach to disaster medicine training for health professionals. J Emerg Med. 2010 Jan 14; doi: 10.1016/j.jemermed.2009.08.064. [DOI] [PubMed] [Google Scholar]
- 20.Association of American Medical Colleges. Number of US Medical Schools Teaching Selected Topics 2004–4005. 2005 NOTE: This webpage is no longer available; http://services.aamc.org/currdir/section2/04_05hottopics.pdf. Accessed November 1 2008.
- 21.Rico E, Trepka M, Zhang G, et al. Knowledge and attitudes about bioterrorism and smallpox: a survey of physicians and nurses. Epidemiology Monthly Report. 2002;3:1–7. [Google Scholar]
- 22.Lanzilotti SS, Galanis D, Leoni N, Craig B. Hawaii medical professionals assessment. Hawaii Med J. 2002 Aug;61(8):162–173. [PubMed] [Google Scholar]
- 23.Gershon RR, Canton AN, Magda LA, DiMaggio C, Gonzalez D, Dul MW. Web-based training on weapons of mass destruction response for emergency medical services personnel. Am J Disaster Med. 2009 May-Jun;4(3):153–161. [PubMed] [Google Scholar]
- 24.Chen J, Wilkinson D, Richardson RB, Waruszynski B. Issues, considerations and recommendations on emergency preparedness for vulnerable population groups. Radiat Prot Dosimetry. 2009 Jun;134(3–3):132–135. doi: 10.1093/rpd/ncp083. [DOI] [PubMed] [Google Scholar]
- 25.Subbarao I, Lyznicki JM, Hsu EB, et al. A consensus-based educational framework and competency set for the discipline of disaster medicine and public health preparedness. Disaster Med Public Health Prep. 2008 Mar;2(1):57–68. doi: 10.1097/DMP.0b013e31816564af. [DOI] [PubMed] [Google Scholar]
- 26.Williams J, Nocera M, Casteel C. The effectiveness of disaster training for health care workers: a systematic review. Ann Emerg Med. 2008 Sep;52(3):211–222. 222, e211–212. doi: 10.1016/j.annemergmed.2007.09.030. [DOI] [PubMed] [Google Scholar]
- 27.Hsu EB, Jenckes MW, Catlett CL, et al. Training to hospital staff to respond to a mass casualty incident. Evid Rep Technol Assess (Summ) 2004 Apr;(95):1–3. [PMC free article] [PubMed] [Google Scholar]
- 28.Improving Patient Safety Through Simulation Research. 2004 http://www.ahrq.gov/qual/simulproj.htm. Accessed March 2, 2012.
- 29.Scott LA. Disaster 101: a novel approach to health care students’ disaster medicine and emergency preparedness training. Disaster Med Public Health Prep. 2009 Oct;3(3):139–140. doi: 10.1097/DMP.0b013e3181b7e666. [DOI] [PubMed] [Google Scholar]
- 30.Barbera JA, Yeatts DJ, Macintyre AG. Challenge of hospital emergency preparedness: analysis and recommendations. Disaster Med Public Health Prep. 2009 Jun;3(2 Suppl):S74–82. doi: 10.1097/DMP.0b013e31819f754c. [DOI] [PubMed] [Google Scholar]
- 31.The George Washington University Institute for Crisis Disaster and Risk Management. VHA-EMA Certification Program, Healthcare Emergency Management Professional Certification Program, Final Program Recommendations. Deliverable 9.11 2007. [Google Scholar]
- 32.Subbarao I, Bond WF, Johnson C, Hsu EB, Wasser TE. Using innovative simulation modalities for civilian-based, chemical, biological, radiological, nuclear, and explosive training in the acute management of terrorist victims: A pilot study. Prehosp Disaster Med. 2006 Jul-Aug;21(4):272–275. doi: 10.1017/s1049023x00003824. [DOI] [PubMed] [Google Scholar]
- 33.Agency for Healthcare Research and Quality. AHRQ Publication No 08-0019. Rockville, MD: 2008. Tool for Evaluating Core Elements of Hospital Disaster Drill. [Google Scholar]
- 34.King HB, Battles J, Baker DP, et al. Team STEPPS: Team Strategies and Tools to Enhance Performance and Patient Safety (Performance and Tools) 2008 Aug;3 [PubMed] [Google Scholar]
- 35.Markenson D, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005 Jun;80(6):517–526. doi: 10.1097/00001888-200506000-00002. [DOI] [PubMed] [Google Scholar]
- 36.Bloom B, Engelhart M, Furst E, Hill W, Krathwohl D. Taxonomy of educational objectives: the classification of educational goals. New York: Longmans, Green; 1956. [Google Scholar]
- 37.Krathwohl D, Bloom B, Masia B. Taxonomy of educational objectives; the classification of educational goals. New York: Longman, Green; 1964. [Google Scholar]
- 38.Smith P, Ragan T. Instructional design. 1999 New York. [Google Scholar]
- 39.Scott L, Ross A, Schnellmann J, Wahlquist A. Surge Capacity: CHPTER and the South Carolina Healthcare Worker Preparedness. The Journal of the South Carolina Medical Society. 2011;107:74–77. June 2011. [PMC free article] [PubMed] [Google Scholar]
- 40.Diehr P, Martin D, Koepsell T, Cheadle A. Breaking the matches in a paired /-test for community interventions when the number of pairs is small. Statistics in Medicine. 1995;14:1491–1504. doi: 10.1002/sim.4780141309. [DOI] [PubMed] [Google Scholar]
- 41.Ruhe DS, Byfield GV. Audiovisual aids for disaster and military medicine in the medical schools. J Med Educ. 1954 Aug;29(81):59–62. doi: 10.1097/00001888-195408000-00011. [DOI] [PubMed] [Google Scholar]
- 42.Kohn LT, Corrigan J, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academy Press; 2000. [PubMed] [Google Scholar]
- 43.Howard SK, Gaba DM, Fish KJ, Yang G, Sarnquist FH. Anesthesia crisis resource management training: teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med. 1992 Sep;63(9):763–770. [PubMed] [Google Scholar]
- 44.Wiener EL, Kanki BG, Helmreich RL. Cockpit resource management. San Diego: Academic Press; 1993. [Google Scholar]
- 45.Murray DJ, Boulet JR, Kras JF, Woodhouse JA, Cox T, McAllister JD. Acute care skills in anesthesia practice: a simulation-based resident performance assessment. Anesthesiology. 2004 Nov;101(5):1084–1095. doi: 10.1097/00000542-200411000-00007. [DOI] [PubMed] [Google Scholar]
- 46.Wayne DB, Didwania A, Feinglass J, Fudala MJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of care during cardiac arrest team responses at an academic teaching hospital: a case-control study. Chest. 2008 Jan;133(1):56–61. doi: 10.1378/chest.07-0131. [DOI] [PubMed] [Google Scholar]
- 47.Wayne DB, Butter J, Siddall VJ, et al. Mastery learning of advanced cardiac life support skills by internal medicine residents using simulation technology and deliberate practice. J Gen Intern Med. 2006 Mar;21(3):251–256. doi: 10.1111/j.1525-1497.2006.00341.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rosenthal ME, Adachi M, Ribaudo V, Mueck JT, Schneider RF, Mayo PH. Achieving housestaff competence in emergency airway management using scenario based simulation training: comparison of attending vs housestaff trainers. Chest. 2006 Jun;129(6):1453–1458. doi: 10.1378/chest.129.6.1453. [DOI] [PubMed] [Google Scholar]
- 49.Tsai TC, Harasym PH, Nijssen-Jordan C, Jennett P. Learning gains derived from a high-fidelity mannequin-based simulation in the pediatric emergency department. J Formos Med Assoc. 2006 Jan;105(1):94–98. doi: 10.1016/S0929-6646(09)60116-9. [DOI] [PubMed] [Google Scholar]
- 50.Shavit I, Keidan I, Hoffmann Y, et al. Enhancing patient safety during pediatric sedation: the impact of simulation-based training of nonanesthesiologists. Arch Pediatr Adolesc Med. 2007 Aug;161(8):740–743. doi: 10.1001/archpedi.161.8.740. [DOI] [PubMed] [Google Scholar]
- 51.DeVita MA, Schaefer J, Lutz J, Wang H, Dongilli T. Improving medical emergency team (MET) performance using a novel curriculum and a computerized human patient simulator. Qual Saf Health Care. 2005 Oct;14(5):326–331. doi: 10.1136/qshc.2004.011148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Franc-Law J, Ingrassia P, Ragazzoni L, Corte F. The effectiveness of training with an emergency department simulator on medical student performance in a simulated disaster. Cjem. 2010 Jan;12(1):27–32. doi: 10.1017/s1481803500011982. [DOI] [PubMed] [Google Scholar]
- 53.Gordon JA, Shaffer DW, Raemer DB, Pawlowski J, Hurford WE, Cooper JB. A randomized controlled trial of simulation-based teaching versus traditional instruction in medicine: a pilot study among clinical medical students. Adv Health Sci Educ Theory Pract. 2006 Feb;11(1):33–39. doi: 10.1007/s10459-004-7346-7. [DOI] [PubMed] [Google Scholar]
- 54.Morgan PJ, Cleave-Hogg D, Desousa S, Lam-McCulloch J. Applying theory to practice in undergraduate education using high fidelity simulation. Med Teach. 2006 Feb;28(1):e10–15. doi: 10.1080/01421590600568488. [DOI] [PubMed] [Google Scholar]
- 55.Ten Eyck RP, Tews M, Ballester JM. Improved medical student satisfaction and test performance with a simulation-based emergency medicine curriculum: a randomized controlled trial. Ann Emerg Med. 2009 Nov;54(5):684–691. doi: 10.1016/j.annemergmed.2009.03.025. [DOI] [PubMed] [Google Scholar]
- 56.Wong G, Jenkins C, Yao TJ, Irwin M. A trend toward improved learning of cardiovascular pathophysiology in medical students from using a human patient simulator: results of a pilot study. Adv Physiol Educ. 2007 Dec;31(4):372. doi: 10.1152/advan.00073.2007. [DOI] [PubMed] [Google Scholar]
- 57.Small SD, Wuerz RC, Simon R, Shapiro N, Conn A, Setnik G. Demonstration of high-fidelity simulation team training for emergency medicine. Acad Emerg Med. 1999 Apr;6(4):312–323. doi: 10.1111/j.1553-2712.1999.tb00395.x. [DOI] [PubMed] [Google Scholar]
- 58.Reznek M, Smith-Coggins R, Howard S, et al. Emergency medicine crisis resource management (EMCRM): pilot study of a simulation-based crisis management course for emergency medicine. Acad Emerg Med. 2003 Apr;10(4):386–389. doi: 10.1111/j.1553-2712.2003.tb01354.x. [DOI] [PubMed] [Google Scholar]
- 59.Kobayashi L, Shapiro MJ, Gutman DC, Jay G. Multiple encounter simulation for high-acuity multipatient environment training. Acad Emerg Med. 2007 Dec;14(12):1141–1148. doi: 10.1197/j.aem.2007.05.015. [DOI] [PubMed] [Google Scholar]
- 60.Andreatta PB, Maslowski E, Petty S, et al. Virtual reality triage training provides a viable solution for disaster-preparedness. Acad Emerg Med. 2010 Aug;17(8):870–876. doi: 10.1111/j.1553-2712.2010.00728.x. [DOI] [PubMed] [Google Scholar]
- 61.Eaves RH, Flagg AJ. The U.S. Air Force pilot simulated medical unit: a teaching strategy with multiple applications. J Nurs Educ. 2001 Mar;40(3):110–115. doi: 10.3928/0148-4834-20010301-05. [DOI] [PubMed] [Google Scholar]
- 62.Decker SI, Galvan TJ, Sridaromont K. Integrating an exercise on mass casualty response into the curriculum. J Nurs Educ. 2005 Jul;44(7):339–340. doi: 10.3928/01484834-20050701-12. [DOI] [PubMed] [Google Scholar]
- 63.Vincent DS, Burgess L, Berg BW, Connolly KK. Teaching mass casualty triage skills using iterative multimanikin simulations. Prehosp Emerg Care. 2009 Apr-Jun;13(2):241–246. doi: 10.1080/10903120802706088. [DOI] [PubMed] [Google Scholar]
- 64.Coule PL, Schwartz RB. The national disaster life support programs: a model for competency-based standardized and locally relevant training. J Public Health Manag Pract. 2009 Mar;15(2 Suppl):S25–30. doi: 10.1097/01.PHH.0000345982.34551.99. [DOI] [PubMed] [Google Scholar]
- 65.Fritz PZ, Gray T, Flanagan B. Review of mannequin-based high-fidelity simulation in emergency medicine. Emerg Med Australas. 2008 Feb;20(1):1–9. doi: 10.1111/j.1742-6723.2007.01022.x. [DOI] [PubMed] [Google Scholar]
- 66.LeRoy Heinrichs W, Youngblood P, Harter PM, Dev P. Simulation for team training and assessment: case studies of online training with virtual worlds. World J Surg. 2008 Feb;32(2):161–170. doi: 10.1007/s00268-007-9354-2. [DOI] [PubMed] [Google Scholar]
- 67.Schumacher J, Runte J, Brinker A, Prior K, Heringlake M, Eichler W. Respiratory protection during high-fidelity simulated resuscitation of casualties contaminated with chemical warfare agents. Anaesthesia. 2008 Jun;63(6):593–598. doi: 10.1111/j.1365-2044.2008.05450.x. [DOI] [PubMed] [Google Scholar]
- 68.Kyle RR, Via DK, Lowy RJ, Madsen JM, Marty AM, Mongan PD. A multidisciplinary approach to teach responses to weapons of mass destruction and terrorism using combined simulation modalities. J Clin Anesth. 2004 Mar;16(2):152–158. doi: 10.1016/j.jclinane.2003.09.003. [DOI] [PubMed] [Google Scholar]
- 69.Lerner E, Schwartz R, Coule P, Pirrallo R. Use of SALT triage in a simulated mass-casualty incident. Prehosp Emerg Care. 2010;14:21–25. doi: 10.3109/10903120903349812. [DOI] [PubMed] [Google Scholar]
- 70.Summerhill EM, Mathew MC, Stipho S, et al. A simulation-based biodefense and disaster preparedness curriculum for internal medicine residents. Med Teach. 2008;30(6):e145–151. doi: 10.1080/01421590802047257. [DOI] [PubMed] [Google Scholar]
- 71.Gillett B, Peckler B, Sinert R, et al. Simulation in a disaster drill: comparison of high-fidelity simulators versus trained actors. Acad Emerg Med. 2008 Nov;15(11):1144–1151. doi: 10.1111/j.1553-2712.2008.00198.x. [DOI] [PubMed] [Google Scholar]
- 72.Wallace DGB, Wright B, Stetz J, Arquilla B. Randomized controlled trial of high fidelity patient simulators compared to actor patients in a pandemic influenza drill scenario. Resuscitation. 2010;81(7):872–876. doi: 10.1016/j.resuscitation.2010.02.026. [DOI] [PubMed] [Google Scholar]
- 73.Kaji AH, Coates W, Fung CC. A disaster medicine curriculum for medical students. Teach Learn Med. 2010 Apr;22(2):116–122. doi: 10.1080/10401331003656561. [DOI] [PubMed] [Google Scholar]
- 74.Van Sickle D, Wenck MA, Belflower A, et al. Acute health effects after exposure to chlorine gas released after a train derailment. Am J Emerg Med. 2009 Jan;27(1):1–7. doi: 10.1016/j.ajem.2007.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Wenck MA, Van Sickle D, Drociuk D, et al. Rapid assessment of exposure to chlorine released from a train derailment and resulting health impact. Public Health Rep. 2007 Nov-Dec;122(6):784–792. doi: 10.1177/003335490712200610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Ball LJ, Dworak J. Disaster in Graniteville. S C Nurse. 2005 Apr-Jun;12(2):1. [PubMed] [Google Scholar]
- 77.Buckley RL, Hunter CH, Addis RP, Parker MJ. Modeling dispersion from toxic gas released after a train collision in Graniteville, SC. J Air Waste Manag Assoc. 2007 Mar;57(3):268–278. doi: 10.1080/10473289.2007.10465329. [DOI] [PubMed] [Google Scholar]
- 78.Mitchell J, Edmonds A, Cutter S, et al. Evacuation Behavior in Response to the Graniteville, South Carolina, Chlorine Spill. University of South Carolina; 2005. Accessed 2005. [Google Scholar]
- 79.Centers for Disease Control. Public Health Consequences from Hazardous Substances Acutely Released During Rail Transit—South Carolina, 2005; Selected States, 1999–9004. MMWR Morb Mortal Wkly Rep. 2005;54 [PubMed] [Google Scholar]